

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acute myocardial infarction (AMI) remains the leading cause of mortality and morbidity worldwide. For reducing mortality and improving prognosis, the rapid and accurate diagnosis of AMI is important, and medical treatment, including revascularization, is crucial at the appropriate time.123 Electrocardiogram (ECG) and cardiac troponin (cTn) play critical roles in the diagnosis and prognosis of AMI.456 Especially in patients without definite ECG changes, cTn has a major role in the diagnosis of acute coronary syndrome (ACS), and recent use of the high-sensitive cardiac troponin (hs-cTn) assay enables rapid diagnosis and provides higher accuracy than conventional cTn assays.2378 Although the advent of hs-cTn has permitted an early diagnosis and the reliable ‘rule out’ algorithm of AMI, unmet clinical needs remain as cTn can be detected only after myocardial necrosis occurs with a delay of a few hours.269
Heart-type fatty acid-binding protein (H-FABP) is a small cytoplasmic protein involved in the transport of fatty acid in cardiomyocytes.101112 It is mainly present in the myocardium and, following myocardial injury, it is rapidly released from the cytosol into circulation.1112 After identification as an early diagnostic marker of AMI,1314 H-FABP has been recognized as a prognostic marker, predicting long-term mortality in patients with ACS along with troponin, highly sensitive C-reactive protein, and B-type natriuretic peptide.1516 However, as mentioned above, the evidence for the early diagnostic and prognostic value of the hs-cTn test is accumulating, the question remains whether additional new cardiac markers such as H-FABP are needed.217 Subsequent studies have demonstrated that H-FABP has additional prognostic value in addition to hs-cTn in patients with suspected ACS, but no additional diagnostic value.181920 Another study has reported that the sensitivity and specificity of H-FABP are higher than hs-cTn within 2 hours from the onset of chest pain, and it could serve as an early diagnostic marker.21
In this study, we examined the diagnostic and prognostic value of H-FABP in patients with suspected ACS who visited the emergency room (ER), using both laboratory analysis and point-of-care testing (POCT).
Go to : 
METHODS
Study design
This observational single-center cohort study was conducted at the Seoul National University Bundang Hospital (SNUBH) from August 2018 until June 2019. The equipment for laboratory analysis and POCT was provided by Genematrix Inc. (Seongnam, Republic of Korea). The company and institute were not involved in the data collection, analysis, or writing of the manuscript, but were provided the opportunity to review the final manuscript version before submission.
Study population
In this study, the patients were 30 years of age or older and presented to the ER within 24 hours following the onset of chest pain and/or dyspnea. Additionally, to be eligible for study inclusion, patients had to be referred for suspected ACS and agree to participate in the study. Exclusion criteria were as follows: 1) decreased consciousness and/or neurological abnormalities; 2) comorbidities other than ACS that require hospital admission; 3) presentation to the ER out of the working hours of laboratory for H-FABP; 4) diagnosis and treatment for malignant neoplasm; and 5) Creatinine clearance < 30 mL/min or a patient undergoing dialysis.
The enrolled patients were divided into two groups. One group visited the ER within 4 hours of the onset of chest pain and/or dyspnea; the other group visited the ER between 4 and 24 hours following the onset of symptoms. The number of subjects in each group was not predetermined.
Study protocol
At presentation, patients underwent routine clinical examination and a 12-lead ECG. The first venous blood sample was collected at the ER and used for both laboratory analysis and POCT of cardiac markers, including H-FABP, troponin I (TnI), and creatine kinase-myocardial band (CK-MB). The second and third venous samplings were performed for the serial laboratory analyses of cardiac markers. For each patient, the first, second, and third sampling times varied as the venous blood sampling interval was not fixed (Fig. 1).
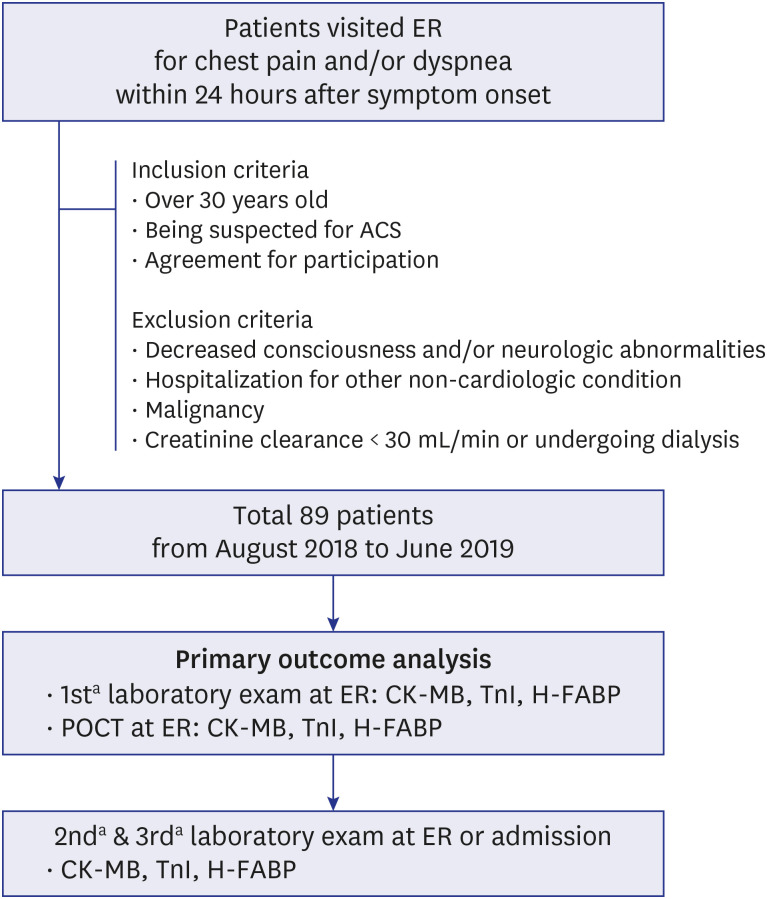 | Fig. 1Study flow.ER = emergency room, ACS = acute coronary syndrome, CK-MB = creatine kinase-myocardial band, TnI = troponin I, H-FABP = heart-type fatty acid-binding protein, POCT = point-of-care testing.
aFirst, second and third sampling times varied as the blood sampling interval was not fixed.
|
Laboratory analysis of H-FABP was performed using a machine utilizing the domestically developed latex turbidimetric immunoassay (LTIA) method. POCT of cardiac markers was performed with rapid kits using a domestically developed immunochromatography (ICA) method. The laboratory results of each cardiac marker were reported within an hour. It took 10 to 15 minutes to obtain POCT result for each cardiac markers. Both laboratory analysis and POCT were performed by a blinded tester.
Study endpoint
The primary outcome was the diagnostic value of H-FABP in the early diagnosis of AMI, determined from the first venous sample at the ER. H-FABP was measured using both laboratory analysis and POCT and compared with other cardiac markers, including TnI and CK-MB. When diagnosing AMI with POCT, positive and negative values were visually judged. The fourth universal definition of myocardial infarction (MI) was utilized for assessments with laboratory analysis.6
The secondary outcome was the prognostic value of the cardiac markers in relation to left ventricular (LV) dysfunction and extent of coronary artery disease (CAD) using laboratory analysed results from 1st, 2nd, and 3rd venous samples. The degree of LV dysfunction was assessed with the left ventricular ejection fraction (LVEF) and wall motion score index (WMSI), which measured by transthoracic echocardiography performed after the ER visit. The extent of CAD was evaluated by coronary angiography (CAG), and significant lesion was defined as stenosis of > 50% of the reference coronary arterial diameter.
Statistical analysis
We presented continuous variables as mean ± standard deviation (SD) or median with interquartile range (IQR), and categorical variables as frequencies. For comparisons between two groups, the Student's t-test and Mann-Whitney U test was performed for continuous variables, and χ2 test and fisher's exact test for categorical variables. To assess their diagnostic accuracy, receiver operating characteristic (ROC) curves were generated for each laboratory analysis of cardiac markers. Then, we compared the area under the ROC curve (AUC) value of H-FABP and TnI using Delong's test. The confusion matrix and McNemar's test were used to assess the POCT accuracy.
Kruskal-Wallis test with Bonferroni post-hoc analysis was used for multiple comparison. Spearman correlation analysis was used to examine relationship between cardiac markers and degree of LV dysfunction.
Statistical analyses were conducted using the R programming, version 4.0.2 (http://www.R-project.org; The R Foundation for Statistical Computing, Vienna, Austria). A P value < 0.05 was considered statistically significant.
Ethics statement
This investigation conformed to the principles outlined in the Declaration of Helsinki and the Institutional Review Board at SNUBH approved the study protocol (B-1702-382-301). Written informed consent was obtained from every patient at the point of inclusion in the study.
Go to :
RESULTS
In total, 89 patients were included in the study. The baseline characteristics are summarized in Table 1. The mean age was 62.3 years, with more male than female patients included. As conventional cardiovascular risk factors, the occurrence of hypertension (HTN), diabetes mellitus (DM), dyslipidemia, and current smoking was 48.3%, 22.5%, 28.1%, and 38.2%, respectively. Additionally, 14 patients had previously received primary coronary interventions and 1 patient had undergone coronary artery bypass graft surgery.
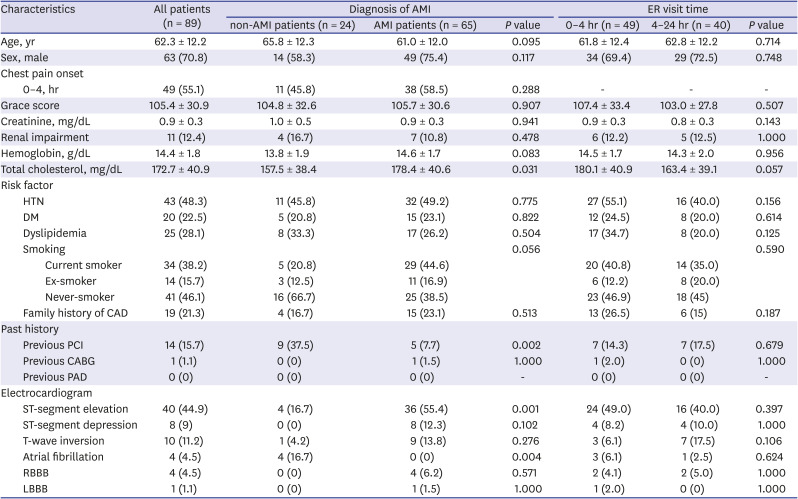
Table 1
Baseline characteristics according to diagnosis of AMI and, ER visit time
Values are presented as mean ± standard deviation, or number (%). Renal impairment was defined as eGFR lower than 50 mL/min/1.73 m2.
ER = emergency room, AMI = acute myocardial infarction, HTN = hypertension, DM = diabetes mellitus, CAD = coronary artery disease, PCI = percutaneous coronary intervention, CABG = coronary artery bypass graft, PAD = peripheral artery disease, RBBB = right bundle branch block, LBBB = left bundle branch block, eGFR = estimated glomerular filtration rate.
![]()
Sixty-five patients were finally diagnosed with AMI, of which 37 patients were ST-elevation myocardial infarction (STEMI) and 28 patients were non-ST-elevation myocardial infarction (NSTEMI). There were five patients with unstable angina (UA), 17 patients with other cardiac disease, and two patients with non-cardiac disease. We compared the baseline characteristics according to whether diagnosed as AMI (Table 1). There was no difference in cardiovascular risk factors except cholesterol level which was higher in AMI patients. Non-AMI patients received more primary coronary interventions and had more atrial fibrillation.
We also compared baseline characteristics according to ER visit time. Forty-nine patients visited the ER within 4 hours after the onset of chest pain and/or dyspnea, and there was no significant difference between two groups.
Diagnostic accuracy of H-FABP vs. TnI and CK-MB using laboratory analysis
The diagnostic accuracy of cardiac markers for AMI in all patients is shown in the Fig. 2A. The AUC values of H-FABP, TnI, and CK-MB were 0.771 (95% confidence interval [CI], 0.674–0.868), 0.759 (95% CI, 0.664–0.854), and 0.690 (95% CI, 0.580–0.801), respectively. The AUC value of H-FABP was the highest, and statistically significant difference was not observed between H-FABP and TnI (P = 0.81, Delong's test).
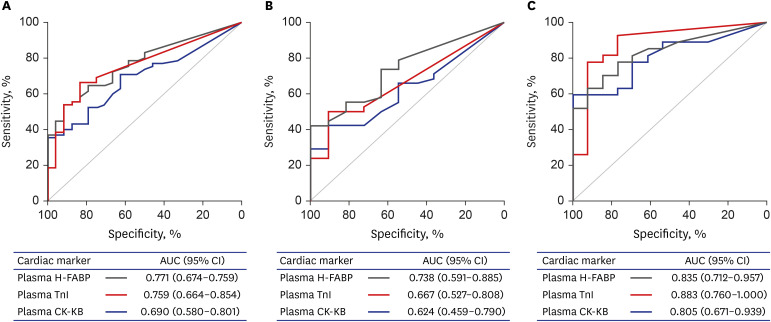 | Fig. 2ROC curve describing the diagnostic accuracy of H-FABP (black line), TnI (red line), and CK-MB (blue line) for acute myocardial infarction. (A) All patients (n = 89). (B) Patients presenting at the emergency room within 4 hours after onset of chest pain and/or dyspnea (n = 49). (C) Patients presenting at the emergency room between 4 and 24 hours after onset of chest pain and/or dyspnea (n = 40).CI = confidence interval, ROC = receiver operating characteristic, AUC = area under the ROC curve, H-FABP = heart-type fatty acid-binding protein, TnI = troponin I, CK-MB = creatine kinase-myocardial band.
|
All patients included in this study were classified according to ER visit time after symptom onset. In the group presenting at the ER within 4 hours (n = 49), the AUC value of H-FABP for quantifying diagnostic accuracy was 0.738 (95% CI, 0.591–0.885). The AUC values of TnI and CK-MB were 0.667 (95% CI, 0.527–0.808) and 0.624 (95% CI, 0.459–0.790), respectively (Fig. 2B). Only the AUC value of H-FABP was above 0.7, without statistical difference with TnI (P = 0.37, Delong's test). In the group presenting at the ER between 4 and 24 hours, the AUC values of H-FABP, TnI, and CK-MB were 0.835 (95% CI, 0.712–0.957), 0.883 (95% CI, 0.760–1.0), and 0.805 (95% CI, 0.671–0.939), respectively (Fig. 2C). No statistically significant difference was observed between H-FABP and TnI (P = 0.50, Delong's test).
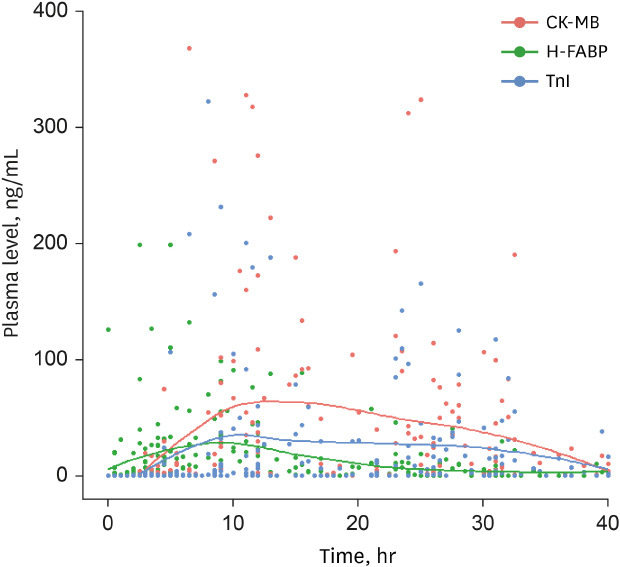
We compared all cardiac marker levels according to ER visit time and final diagnosis (Table 2). Most cardiac markers did not show significant differences in the initial and second measurements according to the ER visit time, but the initial level of TnI was higher in patients visiting ER between 4 and 24 hours (P = 0.01, Mann-Whitney U test). In patients finally diagnosed with STEMI or NSTEMI, all cardiac markers were significantly higher than those diagnosed with UA or non-CAD. Fig. 3 shows serial changes in each cardiac marker levels after symptom onset. H-FABP was first detected within 2 to 3 hours after symptom onset, followed by TnI and CK-MB.

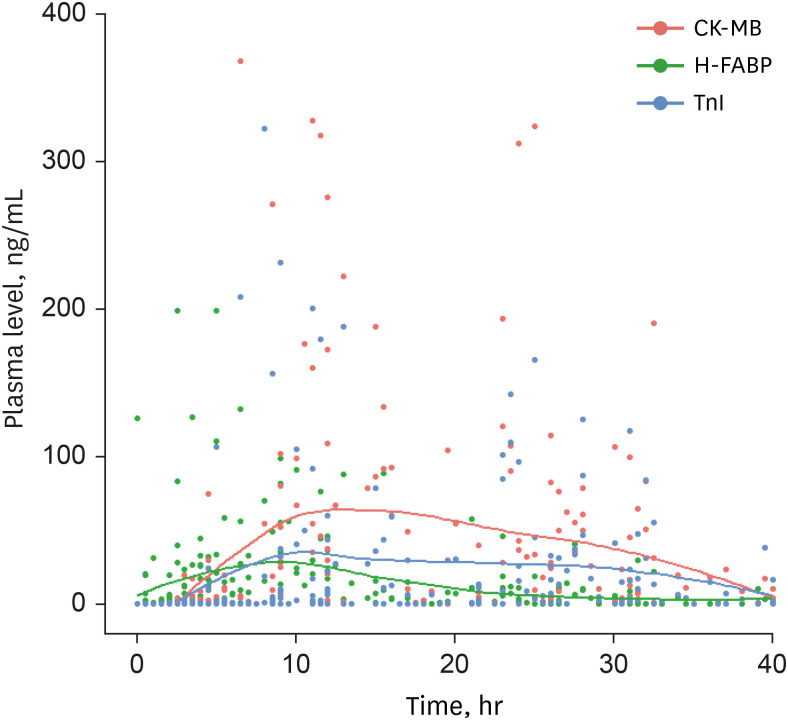 | Fig. 3Changes over time in plasma H-FABP (green dot and line), TnI (blue dot and line), and CK-MB (red dot and line) after chest pain and/or dyspnea onset.H-FABP = heart-type fatty acid-binding protein, TnI = troponin I, CK-MB = creatine kinase-myocardial band.
|
Table 2
Level of cardiac markers according to emergency room visit time and final diagnosis
Values are presented as median (interquartile range).
H-FABP = heart-type fatty acid-binding protein, TnI = troponin I, CK-MB = creatine kinase-myocardial band.
![]()
Diagnostic accuracy of H-FABP vs. TnI and CK-MB by POCT
The diagnostic accuracy of H-FABP for AMI was 56% (95% CI, 45–67); for TnI and CK-MB, the diagnostic accuracies were 37% (95% CI, 27–48) and 35% (95% CI, 25–46), respectively. Hence, the accuracy of H-FABP and TnI differed significantly (P < 0.05).
Prognostic value of H-FABP vs. TnI and CK-MB
We evaluated the prognostic value of H-FABP in association with LV dysfunction and CAD extent, and compared it with TnI and CK-MB. All cardiac markers showed significant correlation with LV dysfunction, WMSI and LVEF. TnI and CK-MB showed correlation only in the second and third measurements, whereas H-FABP showed weak but significant correlation from the initial measurement (Fig. 4A and B).
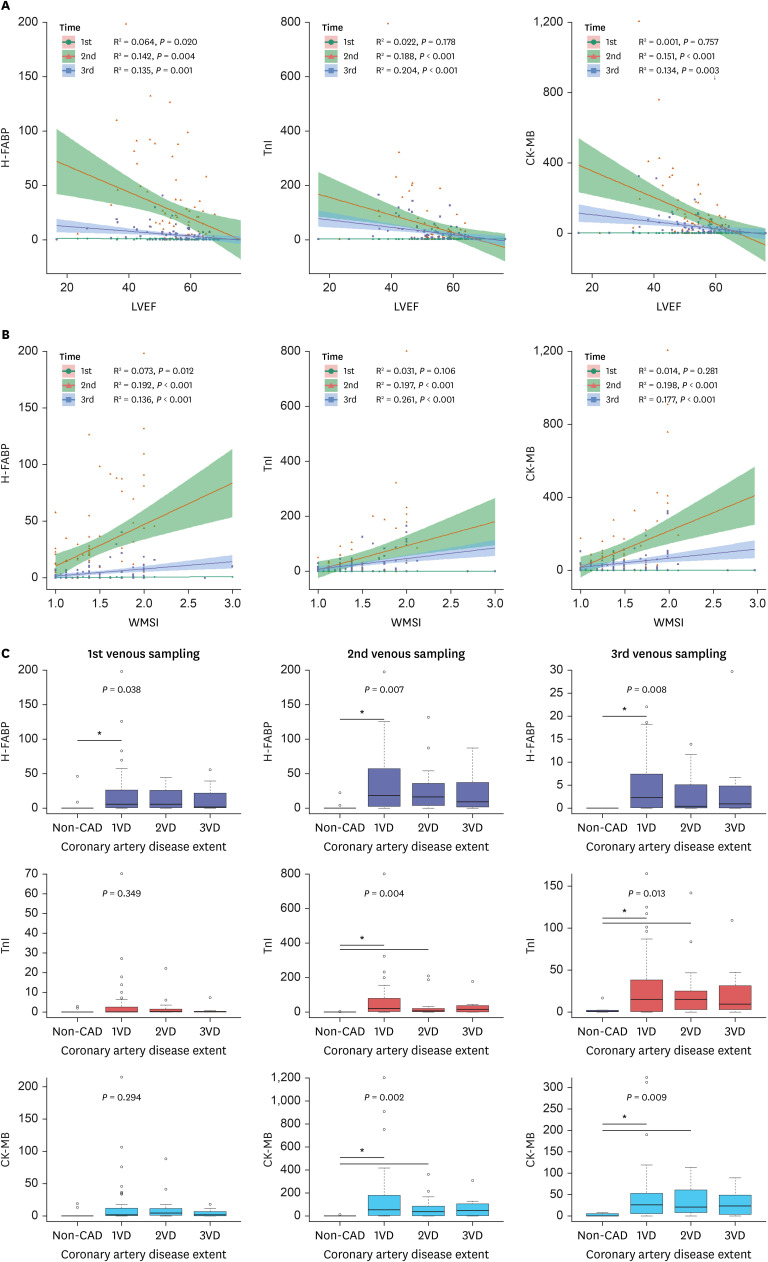 | Fig. 4Relationship between cardiac markers and left ventricular dysfunction and extent of coronary artery disease with 1st, 2nd, and 3rd measurements. (A) Negative relationship between cardiac markers and LVEF. (B) Positive relationship between cardiac markers and WMSI. (C) Relationship between cardiac markers and coronary artery disease extent.WMSI = wall motion score index, LVEF = left ventricular ejection fraction, H-FABP = heart-type fatty acid-binding protein, TnI = troponin I, CAD = coronary artery disease, CK-MB = creatine kinase-myocardial band, 1VD = 1 vessel disease, 2VD = 2 vessel disease, 3VD = 3 vessel disease.
|
Level of H-FABP was not relevant in predicting the extent of CAD, but showed significant difference between CAD and non-CAD (Fig. 4C). Levels of TnI and CK-MB also showed similar result.
Go to :
DISCUSSION
This observational study aimed to investigate the diagnostic and prognostic value of H-FABP in patients suspected with ACS. We hypothesized that H-FABP might be beneficial in the early diagnosis of AMI based on the different circulatory release times of cardiac markers following myocardial injury.1112152223 The accuracy of H-FABP and TnI in the diagnosis of AMI using laboratory analysis demonstrated no statistical difference as quantified by the AUC values. However, patients who presented at the ER within 4 hours after symptom onset showed the highest diagnostic accuracy in H-FABP, while TnI demonstrated the highest diagnostic value in patients presenting between 4 and 24 hours, with no statistical significance observed. The rapid POCT kit for H-FABP demonstrated superior accuracy than TnI in the early-visit patients. Therefore, for physicians managing patients complaining of acute onset of chest pain and/or dyspnea, H-FABP could aid the rapid diagnosis of patients with ACS.
Although consensus on the diagnostic utility of H-FABP has not been established, some studies have suggested that H-FABP is useful in the early diagnosis of AMI. McCann et al.23 have analyzed 664 patients admitted to the cardiology department with acute chest pain for a duration of < 24 hours. They have observed that assessment of H-FABP within the first 4 hours of symptom onset is superior to cTn T for the detection of MI. In the present study, H-FABP was first detected within 2 to 3 hours following myocardial injury, followed by TnI and CK-MB (Fig. 3). Notably, as H-FABP is a small soluble protein, it is easily released into systemic circulation compared to other proteins. Its low threshold also attributes to early detection.
Kellens et al.24 have evaluated 203 patients referred for suspected ACS or presented at the ER with typical chest pain, using plasma high-sensitive troponin T (hs-TnT) and point-of-care H-FABP testing concomitantly performed at admission, and after 6 and 15 hours. For assessments performed within 3 hours of chest pain onset, the diagnostic accuracy of H-FABP and hs-TnT was comparable. In our study, POCT for H-FABP showed better diagnostic ability and convenience in performing and analyzing, thus it might be useful in early detection and exclusion of AMI at emergency medical service or ER.
We also evaluated the prognostic value of H-FABP. It was not relevant in predicting the extent of CAD, but helpful in predicting the extent of LV dysfunction after myocardial injury. Only initial level of H-FABP showed significant correlation with LVEF and WMSI although the correlation coefficient was very low. This is presumed to reflect H-FABP's characteristic which being detected at early stage of myocardial injury.
This study has a few limitations. First, the number of enrolled patients was small. Second, there exists a selection bias. Registration was carried out in patients who were referred to cardiology department after primary emergency care, so patients presenting ER for dyspnea and/or chest pain were not consecutively collected. This resulted in an unbalanced distribution of data, with about 73% of patients finally diagnosed with AMI. Third, the interval between each venous sample was irregular. Because the consent was obtained after the diagnostic work-up and management were already conducted, we could not control the timing of blood collection.
In conclusion, H-FBAP is a useful cardiac marker for early diagnosis of AMI and prediction of myocardial injury. Differences in the circulatory release timeline of cardiac markers explain its utility in early stage of myocardial injury. Further large-scale clinical studies could help establish consensus regarding H-FABP test in Korea and compensate for the limitation of cTn test.
Go to :
 XML Download
XML Download