

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of aortic stenosis (AS) is increasing with the aging of society, and is estimated as 1.3% among individuals in their sixties and up to 9.8% among octogenarians.1 Furthermore, as echocardiography has become widely adopted, a considerable number of asymptomatic patients with mild to moderate AS are diagnosed. Although asymptomatic AS is generally considered to have a good prognosis, several studies have demonstrated that asymptomatic mild to moderate AS is associated with poor clinical outcomes, thus suggesting that even mild disease should not be overlooked.234
The mechanism of disease progression overlaps that of coronary artery disease (CAD) including active inflammatory process, and it is well known that CAD is an important risk factor of AS, as well as the severity of AS.567 However, drugs effective in CAD failed to slow the hemodynamic progression of AS, and the guidelines do not support any of them in patients with AS.89 Because there is an incomplete understanding of the natural course of AS and a lack of solid evidence to support treatment,10 the only recommendation in the current guideline is regular follow up with echocardiography.11
The purpose of the present study was to analyze the clinical course of patient with asymptomatic mild to moderate AS and to assess its association with CAD.
METHODS
Study population
We reviewed the records of 1,092 patients diagnosed with aortic sclerosis and AS using echocardiography between January 2004 and December 2010 using the Clinical Data Warehouse system at Seoul National University Bundang Hospital (Fig. 1). We identified 982 asymptomatic patients with mild to moderate AS using the following criteria: peak aortic valve velocity 2.0–3.9 m/sec, aortic valve area more than 1.0 cm2, and mean pressure gradient less than 40 mmHg. Patients who complained of mild dyspnea or chest discomfort were included because of the lack of specificity of these symptoms.12 We excluded patients with severe mitral disease, prosthetic valve in situ, infective endocarditis, heart failure, or an ejection fraction less than 50%. We further excluded patients with death within 30 days of the index echocardiography. The remaining 787 patients were analyzed. In addition, general population cohort data were obtained from the National Health Insurance Service to allow comparisons between the patient cohort and the general population.
Study outcomes and data collection
Co-primary outcomes were cardiac death and aortic valve replacement (AVR) including both surgical transaortic AVR for AS. The composite outcome of cardiac death and AVR was also assessed. Data on cardiac death was obtained from the Statistics Korea and cross checked with the mortality data from the Korean Ministry of Security and Public Administration. The ICD-10 codes included for the definition of cardiac death were: I01–I15, I20–I25, I30–I48, I50–I51, and I70–I77. The last date of death confirmation was November 27, 2017. Confirmation of AVR for AS was done by reviewing electronic medical record. Documentation of CAD was as follows: 50% stenosis on coronary angiography or coronary computed tomography angiography, or a perfusion defect on single-photon emission computed tomography. Statin and other drug use were determined using the reimbursement system database of the National Health Insurance Service.
Statistical analysis
Continuous variables, expressed as mean ± standard deviation, were compared using the Student's unpaired t-test. Categorical variables, presented as frequencies and percentages, were compared using the χ2 or Fisher's exact test.
For the comparison of cardiac death between patients with mild to moderate AS and the general population, patients were matched (1:50 ratio) to Korea National Health Insurance Service Cohort 2.0 (n = 39,350 [male, 23,500; female, 15,850]) based on age and sex. The Kaplan-Meier method and log-rank test were used to visualize the survival probabilities. The adjusted hazard ratio (HR) was calculated to adjust difference in covariates. The covariates that were included in the Cox proportional hazard modeling were age, sex, hypertension, diabetes mellitus, CKD, CAD, AS etiology, and peak aortic valve velocity, aspirin, beta-blockers, and renin-angiotensin system (RAS) inhibitors. The collinearity among all significant variables was tested using variance inflation factors, and a cutoff value of 3.0 was applied to identify collinearity. To determine the best multivariable linear regression model, the stepwise regression method under Akaike's information criterion was performed. All reported P values are 2-tailed, and P ≤ 0.05 was considered statistically significant. All statistical analyses were performed using R statistical software/environment (version 3.4.0; The R foundation for Statistical Computing, Vienna, Austria).
RESULTS
Baseline characteristics
The 787 included patients had a median follow-up period of 92 months (48–119 months). Baseline characteristics are shown in Table 1. The mean age of the patient cohort was 71.2 ± 12.2 years, and 59.7% were male. Degenerative change was a dominant etiology of AS (91.0%). Patients with established CAD was 176 (22.4%), and 51.7% of patients were taking statin.
Table 1
Baseline characteristics

Data are shown as mean ± standard deviation or number (%), unless otherwise specified.
BMI = body mass index, CAD = coronary artery disease, CKD = chronic kidney disease, AV = aortic valve, AVA = aortic valve area, MSPG = mean systolic pressure gradient, EDV = end diastolic volume, EF = ejection fraction, RAS = renin-angiotensin system.
Cardiac death
The probability of cardiac death at 10 years was 16.5% (95% confidence interval [CI], 13.2%–19.7%) in the patient cohort (Fig. 2). When patients with mild to moderate AS was compared to the age- and sex-matched general population cohort, the patient cohort went through substantially worse clinical course. The probability of cardiac death rate in the patient cohort was much higher (HR, 17.16; 95% CI, 13.65–21.59, P < 0.001), and the separation between the two curves continued to increase during the follow-up period.
Fig. 2
Prognosis of patients with mild to moderate aortic stenosis compared to the general population.
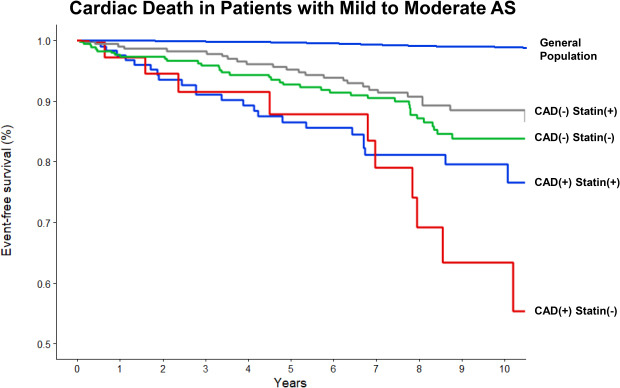
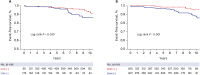
As expected, the 10-year incidence of cardiac death was significantly higher in patient with established CAD (log rank P = 0.002) (Fig. 3). The adjusted risk of cardiac death was 1.62 (95% CI, 1.04–2.53; P = 0.033) (Table 2). The 10-year incidence of cardiac death was not different between statin users and non-users (log rank, P = 0.5). But, the curve diverged after 7 years, and the landmark analysis showed statistical difference (log rank P = 0.04) (Supplementary Fig. 1). Moreover, the adjusted risk of cardiac death was significantly lower in statin users (adjusted HR, 0.64; 95% CI, 0.41–0.98; P = 0.041).
Fig. 3
Kaplan-Meier curves for cardiac death. (A) The presence of established CAD and (B) the use of statin.
CAD = coronary artery disease.
Table 2
Risk of adverse events according to the presence of established CAD and the use of statin over 10 years

Data are shown as number (%), unless otherwise specified. Adverse events expressed in number (%) are crude events over 10 years.
CAD = coronary artery disease, HR = hazard ratio, CI = confidence interval, CV = cardiovascular, AVR = aortic valve replacement.
aHR with 95% CI was adjusted with age, sex, hypertension, diabetes mellitus, chronic kidney disease, CAD, aortic stenosis etiology, and peak aortic valve velocity, aspirin, beta-blockers, and renin-angiotensin system inhibitors.
AVR
A total of 37 (4.7%) patient underwent AVR during 10-year follow-up, and the median time to AVR was 7.3 years (3.8–9.6 years). The 10-year incidence of AVR was 8.3% (Supplementary Fig. 2). Patients with established CAD underwent more AVR (log rank P = 0.030) (Fig. 4), yet the difference was not significant when adjusted (1.63; 95% CI, 0.51–3.51; P = 0.214). Similarly, more patient in statin group underwent AVR (log rank P < 0.001), but adjusted HR was not statistically significant (1.86; 95% CI, 0.76–4.58; P = 0.177).
Composite outcome
The 10-year incidence of composite outcome was significantly higher in patient with established CAD (log rank P < 0.001) (Supplementary Fig. 3), but was not different between statin user and non-users (log rank P = 0.100). However, both the presence of established CAD and the use of statin were not associated with 10-year risk of composite outcome in multivariable analysis (Table 2).
DISCUSSION
Using a study cohort with a long follow-up period, the present study demonstrated that patients with asymptomatic mild to moderate AS have a substantially worse clinical outcome than the general population. CAD was associated with higher risk of cardiac death, and statin use seemed to be associated with lower risk of cardiac death. The risk of undergoing AVR seems to be similar regardless of CAD and statin use.
The natural course of patients with severe AS is well-validated and extensive studies have been conducted to guide its treatment.1213141516 On the other hand, the natural course of patients with mild to moderate AS is still not fully understood. A previous landmark prospective study by Otto et al.17 reported that patients with aortic sclerosis without hemodynamic obstruction have a 50% increase in the risk of cardiovascular death. A subsequent study reported that the event-free survival of patients with mild to moderate AS was 60% at 5 years, and mortality was 1.8 folds higher than expected.3 In the present study, we confirmed that the natural course of patients with mild to moderate AS is grave, relative to that in an age- and sex-matched cohort comprising approximately 39,000 people from the general population. Although the SEAS trial, a well-designed clinical randomized trial, reported favorable clinical outcomes in this patient group, the discrepancy in results can be explained by the fact that the patients in the SEAS trial had isolated aortic valve disease with minimal cardiovascular risk factors while the present study population represented the real world setting.18
The pathophysiology of AS has similarities to that of other medical conditions, such as atherosclerosis, hypertension, and osteoporosis.5 Although some therapeutic targets have been suggested based on these findings, there are no effective medical treatments to modify the disease course. Several retrospective studies have suggested the effectiveness of statins and RAS blockers.192021 However, no large prospective clinical trial has been conducted with RAS blockers, and randomized clinical studies have demonstrated negative results for statins.182223
In present study, CAD was clearly associated with a higher risk of cardiac death in patients with mild to moderate AS (Supplementary Fig. 4). Otto et al.17 underscored the fact that half of all-cause death in patients with AS resulted from cardiovascular death, implying the importance of vascular factors reflecting atherosclerosis. Large clinical trials enrolled patients with isolated AS and with a relatively less risk factor, and they did not have CAD. In SEAS trial, death from cardiovascular cause was low (6.0% in placebo group and 5.0% in statin group).18 However, composite of ischemic events was significantly higher in placebo group (20.1% vs. 15.7%; P = 0.02), and placebo group had more coronary bypass surgery (10.8% vs. 7.3%; P = 0.02). The present study population had more cardiovascular risk factors, and 22.4% of patients had documented CAD at the index echocardiography. Although statin users tend to be a higher risk group, they had better clinical outcome in cardiac death. These findings suggest that statin use can be beneficial in patients with AS, as the population overlaps with not only the CAD population, but also the subclinical CAD population who are at risk.
Progression of AS is associated with various factors such as age, C-reactive protein, diabetes, hypertension, dyslipidemia, and CAD.242526 In this study, patients with CAD tend to undergo more AVR, and statin use was not associated with lower incidence of AS, but rather increasing tendency. These results comply with previous literatures as patients with CAD or on statin are higher risk subset for progression of AS. One other possible explanation is that physicians may perform surgical intervention relatively earlier if patients have both CAD and severe AS.
Our study has several limitations. Because the present study was retrospective in nature, we cannot exclude selection biases. We excluded patients those who died within 30 days of the index echocardiography to minimize a selection bias related to the indication of echocardiography. To further control the effect of covariates, Cox proportional hazard model was performed. In addition, the cardiac death of patients with mild to moderate AS was higher than that previously reported. This was probably due to the nature of our hospital, which is a tertiary and referral center for several diseases. Unfortunately, we did not have follow up echocardiography data to evaluate progression of AS. Lastly, we only had prescription data at the time of index echocardiography. Patients generally continue statins once they are on, yet the fact that we do not have data on exact duration of statin use is a major limitation.
In conclusion, the present study demonstrated that mild to moderate AS needs to be considered a serious condition associated with higher cardiovascular mortality. CAD was associated with higher cardiac death, and statin use seemed to be associated with a lower mortality risk in patients with mild to moderate AS. However, CAD and statin had no clear relation to the risk of AVR.
 XML Download
XML Download