

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The influenza virus causes seasonal epidemics and pandemics, with medical problems occurring in 5%–20% adults.1 Pregnant women are considered high-risk groups for influenza as they are more likely to develop severe influenza and have fetus-related complications than non-pregnant women.23 Maternal cell-mediated immunity is suppressed during pregnancy to improve the tolerance of fetal antigens. Compared to the general population, pregnant women have increased morbidity and mortality owing to pregnancy-related hormonal changes, increased cardiac output, increased oxygen consumption, and reduced lung capacity.45 The effects of influenza infection on the fetus are not well established, but the virus is not thought to cross the placental barrier and infect the fetus.6 However, experiments with the influenza virus in animals have shown histological changes in the fetal brain due to inflammatory factors passing through the placenta without direct transmission of the virus.7 Further, congenital anomalies have been reported in infants exposed to the influenza virus during gestation.8910
To prevent such complications, pregnant women are considered a priority group for influenza vaccination. However, despite long-standing public health recommendations, the influenza vaccination coverage rate in pregnant women in Korea is low, as we reported in 2006–2007 (4.0%).11 Subsequent influenza (2009) and the Middle East respiratory syndrome (2015) outbreaks have increased public concern regarding infectious diseases.1213 These concerns may have led to altered perceptions and increasing vaccination coverage rates; however, there has been no definitive investigation of this issue. In a previous study of the 2012–2013 influenza season, the influenza vaccination coverage rate in pregnant women was 48.6%.14 Another study conducted in 2008–2012 reported a vaccination rate of 38.6% in pregnant women or women planning to become pregnant.15 However, these studies could not analyze the changes in vaccination coverage rates and perceptions regarding vaccination. We, therefore, designed the present study to evaluate changes in influenza vaccination coverage rates and related factors that influence them in pregnant women.
Go to : 
METHODS
Study population
In 2007, we had conducted a study at Inha University Hospital, Incheon, Korea, surveying pregnant women during the 2006–2007 influenza season regarding vaccination against influenza.11 To expand these data, we also conducted further investigations on influenza vaccination in pregnant women during 2011–2012 and 2018–2019 flu season in August 2012 and 2019, respectively. The 2006–2007 and 2011–2012 surveys only included women in their second or third trimester during the influenza season. However, in the 2018–2019 study, women at all stages of pregnancy were included. Therefore, when comparing the three seasons, only data on pregnant women in their second and third trimesters were used from the 2018–2019 study.
Interview method
Contact information of women who were pregnant during the study period was obtained from the hospital's medical records. The same interview protocol was used in 2007, 2012, and 2019. Women who provided informed consent were asked about underlying diseases and comorbidities, antenatal care, delivery method, influenza vaccination status, reasons for undergoing or not undergoing vaccination, and perceptions regarding influenza vaccination. Perceptions regarding influenza vaccination were assessed using seven questions on the safety, efficacy, and cost of the influenza vaccine, with scores ranging from 0 to 7 (Table 1). Higher scores reflected greater knowledge regarding influenza vaccine. Questions on physician recommendations and pre-pregnancy influenza vaccination histories were also asked. For validation, we evaluated the concordance between medical records and survey responses on vaccination history; 39 respondents had been vaccinated at Inha University Hospital, and all responses corresponded with the medical records.
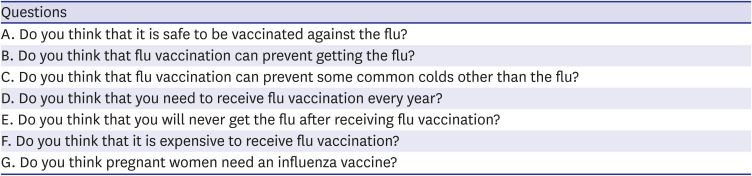
Table 1
Questionnaire on the understanding of influenza
![]()
Data analysis
One-way analysis of variance and the χ2 test (with Bonferroni correction) were used to compare the basic characteristics of the three groups (2007, 2012, and 2019). Student's t-test (for perception score) and the chi-square test (for physician recommendation rate) were used to compare vaccinated and unvaccinated pregnant women. A P value of < 0.05 was considered statistically significant. Data analysis was performed using SPSS statistical software, version 18 (SPSS Inc., Chicago, IL, USA).
Ethics statement
Ethical approval from the Institutional Review Board (IRB) of Inha University Hospital (Incheon, Korea) was obtained before this study and informed consent was waived by the board (IRB No.: 2019-06-009). All patient records were anonymized.
Go to :
RESULTS
General characteristics of the respondents
A total of 550 pregnant women responded to the survey (227/506 [44.8%] in 2006–2007; 152/301 [50.8%] in 2011–2012; and 171/265 [64.5%] in 2018–2019, P < 0.001). The response rate and mean age of the respondents were significantly different between the three surveys (44.8% and 31.5 years in 2007, 50.8% and 34.2 years in 2012, 64.5% and 33.2 years in 2019, P < 0.001). However, there were no significant differences in antenatal care or delivery methods between the three surveys (Table 2).
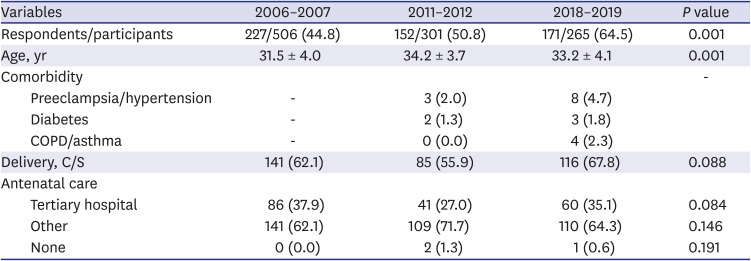
Table 2
General characteristics of the respondents
Data are presented as number (%) or mean ± standard deviation.
COPD = chronic obstructive pulmonary disease, C/S = caesarean section.
![]()
Changes in influenza vaccination coverage, perception score, and physician recommendations
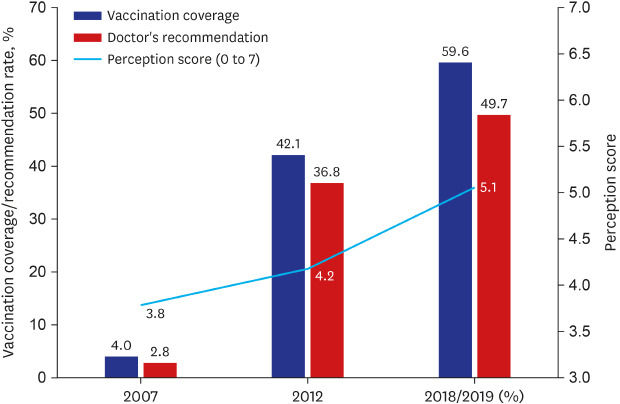
In 2006–2007, the influenza vaccination coverage rate was 4%, the mean perception score was 3.79, and the physician recommendation rate was 4.8%. These parameters increased to 42.1%, 4.17, and 36.8% in 2011–2012 and 59.6%, 5.06, and 49.7% (63.0%, 5.10, and 50.1% if including pregnant women in their first trimester) in 2018–2019 (Fig. 1).
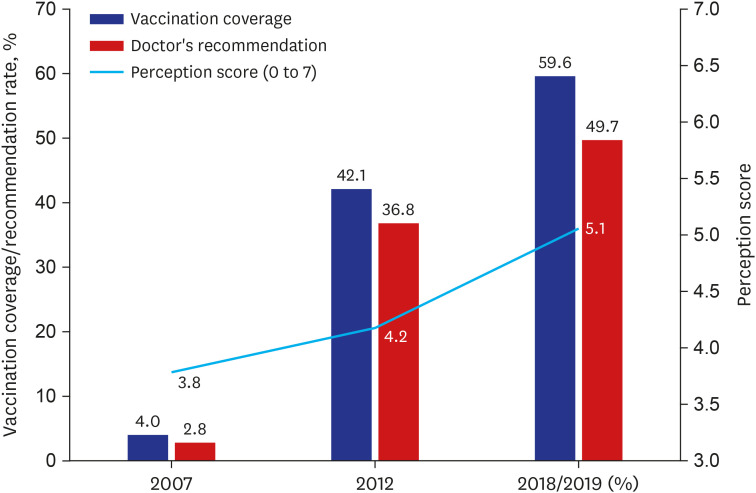 | Fig. 1The change of influenza vaccine coverage rate and perception score. Fig. 1 shows alternations in the influenza vaccine coverage rate, physician recommendation rate, and perception scores. Influenza vaccine coverage rate and physician recommendation rate are presented in percentile and perception score is presented by mean value.
|
Comparisons between vaccinated and unvaccinated women
The mean perception score in vaccinated women from all surveys was 5.1 (standard deviation [SD], 1.1) compared to 3.9 (SD, 1.4) in unvaccinated women; the difference was statistically significant (P < 0.001). The combined vaccination coverage rate was significantly higher in women who received a physician recommendation for vaccination than in women who did not (69.1% vs. 8.4%; P < 0.001) (Table 3).

Reasons for vaccination/vaccination and other related factors
Overall, the common reasons for receiving the vaccine were preventing influenza (49.7%) and ensuring fetal health (46.3%) (Table 4). The most common reason for not receiving vaccination was a lack of enough information regarding vaccination (36.9%). In 2006–2007, 48.5% respondents did not receive influenza vaccination because they did not have enough information regarding the vaccine. However, in 2018–2019, only 18.8% respondents provided this reason. The belief that influenza vaccination is contraindicated during pregnancy was expressed by 36.4% respondents (Table 5). In 2018–2019, many respondents provided various answers (n = 29) for the reason for non-vaccination—“because I thought I missed the proper timing” (n = 9), “because I wasn't feeling well” (n = 7), “because I was too healthy to get influenza” (n = 5), “allergy to influenza vaccine” (n = 1), “because I have never received an influenza vaccine” (n = 1), and “no response” (n = 6).

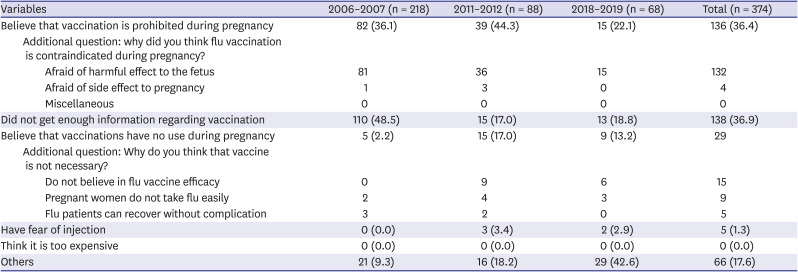
Table 4
Major reasons for receiving vaccination
![]()
Table 5
Major reasons for not receiving vaccination
![]()
In 2018–2019, the respondents were asked about their primary source of information on childbirth at the time of pregnancy. The principal sources of information were websites (39.8%), followed by physicians (28.1%), internet communities (16.4%), books and magazines (8.2%), and friends and family members (7.6%).
Go to :
DISCUSSION
In the 2006–2007 survey, we found that the influenza vaccination coverage rate of pregnant women in Korea was only 4.0%, which is considerably lower than the rate reported for other influenza risk groups (61.3%), such as cardiovascular disease, diabetes mellitus, chronic pulmonary disease, chronic liver disease, and malignant tumor.16 Moreover, the perception score was 3.2%, and only 4.8% physicians had recommended influenza vaccination.
In the 2011–2012 survey, the influenza vaccination coverage rate increased to 42.1%. Compared to the 2006–2007 survey, more physicians had recommended influenza vaccination (4.8% vs. 30.2%) and the perception scores increased. We speculate that physician recommendations and improved perceptions regarding the influenza vaccine played an important role in increasing the vaccination coverage rate. The 2009 influenza pandemic may have also played an important role in this process. Pandemics/epidemics can increase awareness regarding infectious disease among both physicians and the general public.1718 In this study, 34.8% respondents stated that the pandemic had increased their awareness regarding the need for vaccination.19 Perception scores and vaccination coverage rates were higher in 2018–2019 than in 2011–2012, but the vaccination coverage rate was only 60%. In September 2019, the government decided to vaccinate pregnant women free of charge.20 Because our results did not find the cost of vaccination to be a barrier to receiving the vaccine (Table 3), extensive education and publicity among pregnant women and physicians are needed.
During the entire study period, although 70.9% pregnant women received influenza vaccination at least once before the target pregnancy, only 31.8% received the vaccine during pregnancy. This supports our results that many women believe that vaccination is contraindicated during pregnancy. Respondents also expressed concerns regarding potential fetal complications from vaccination, and many lacked confidence in the safety of the vaccine. However, influenza vaccine has fewer severe side effects than other common vaccines and is generally associated with only mild side effects such as local reactions, mild fever, and myalgia. Moreover, many studies have found that influenza vaccination is not harmful to fetuses and infants.21 Compared to 2007, favorable perceptions regarding influenza vaccine increased in 2011–2012 and 2018–2019. However, many pregnant women still have low knowledge regarding influenza vaccination; hence, accurate publicity and education regarding influenza vaccination are needed.
Physician recommendations are an essential factor in vaccination coverage.22 However, only 36.8% (2011–2012) and 49.7% (2018–2019) pregnant women reported that their physician had recommended an influenza vaccination. Although these rates were higher than those noted in our 2007 study, they were still low. Therefore, education regarding influenza vaccination is required among physicians and pregnant women.22 In the 2018–2019 survey, information was more frequently obtained from the internet or via community and social network systems than from physicians. Thus, education and publicity regarding influenza vaccination must be implemented in various ways.
The representative strategies used by the Korea Centers for Disease Control and Prevention for encouraging vaccination are public campaigns, posters, and free vaccination in public health care centers. However, as antepartum care is mostly provided in obstetrics clinics and not in health care centers in Korea, it is unclear whether public relations and prescriptions are appropriately managed in obstetrics clinics. Advertising targeted to physicians at local clinics, in many ways, is also essential. Refresher education for physicians and an automatic prescription system can be considered. It will be a great help if the local government can introduce a pregnant-management system. It will become increasingly important to use public advertisements and social network systems to target pregnant women.
The present study has several limitations. First, it was performed in a single tertiary hospital and may not represent the entire population of pregnant women in Korea. Second, the sample size was relatively small. Third, women in the first trimester were excluded from the 2006–2007 and 2011–2012 influenza seasons. Fourth, the survey was telephonically conducted, and the overall response rate was only 51.3%; therefore, bias may have been introduced during the surveys. Fifth, it is difficult to identify the various causes of vaccination/non-vaccination because multiple responses were not allowed in this study. However, the purpose of our study was not to evaluate the vaccination coverage rate accurately, but to confirm the trend of coverage rates over time and evaluate the factors that influence them. We believe that the limitations mentioned above will not have a significant impact on the results of this study.
In conclusion, the influenza vaccination coverage rate during pregnancy appears to have significantly increased between the 2006–2007 and 2018–2019 influenza seasons. Increased favorable perceptions regarding the influenza vaccine and rising physician recommendation rates likely had important roles in increasing vaccination coverage. To attain even better influenza vaccination coverage rates, extensive publicity and education regarding influenza vaccination are needed among physicians and pregnant women.
Go to :
 XML Download
XML Download