

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to the World Health Organization, nearly 800,000 people die of suicide every year.1 As of 2018, the rate of suicide among all Organisation for Economic Co-operation and Development (OECD) member countries was highest in Korea (24.6 per 100,000 people),2 and suicide is a major disease burden in this country.34 According to the 2018 National Survey on Suicide, 1.5% of the Korean population reported having experienced suicide attempts.5 Not all suicide attempts lead to suicide; previous studies have shown that only 3.4%–5.4% of suicide attempters actually complete suicide.67 There is a need for a selective approach focusing on suicide attempts that are more likely to lead to death later.
A previous study conducted in the United States reported that the risk of suicide completion varies depending on the method of suicide attempt.8 In another study conducted in Korea, a comparison of methods between suicidal attempters and completers also showed a greater risk of suicide completion in more fatal methods.9 Accordingly, patients who choose fatal methods can be considered to be at a greater clinical risk. If the risk factors for suicide attempters to choose fatal methods are identified, this knowledge may be useful in evaluating an individual's suicide risk.
Meanwhile, various evidences suggest that traumatic experiences in childhood constitute a risk factor for suicide-related behavior.101112 In many well-structured large-scale prospective or case-control studies, early trauma, such as neglect,13 physical and emotional abuse,1415 and parental economic problems,16 was a risk factor for suicide attempts. In another meta-analysis, childhood sexual abuse experiences increased the risk of PTSD, depression, and suicide.17 Regarding how early trauma actually leads to suicide-related behavior, reports have shown that traumatic experiences alter one's temperament and character,1819 and decrease emotional and behavioral control skills.20
According to Cloninger's unified biopsychosocial theory of temperament and character, human personality can be explained by dividing it into four temperament and three character dimensions.21 Cloninger saw temperament as inheritable with respect to the neurotransmitter system and as comprising harm-avoidance, novelty-seeking, reward-dependence, and persistence, whereas character reflects different behaviors depending on the maturity of personality development and social adaptability, comprising self-directedness, cooperativeness, and self-transcendence.
There have been few papers studying changes in Temperament and Character Inventory (TCI) in early trauma. In one cross-sectional study of the general population, early trauma was associated with high harm avoidance and novelty seeking, and low reward dependence, persistence, self-directedness, and cooperativeness.22 Another study of soldiers reported that low self-directedness and cooperativeness were associated with early trauma.23
Meanwhile, various studies have reported the relationship between personality traits evaluated by TCI and suicide-related behaviors. High harm avoidance,24252627 low self-directedness,25262728 low cooperativeness,2526 and high self-transcendence262829 have been reported to be associated with suicide-related behaviors. However, in previous studies that included bipolar disorder patients and suicide completers who responded to psychological autopsy, respectively, there was no significant difference in the subscale of TCI between violent and non-violent suicide methods.3031 However, these studies did not statistically correct for demographic variables such as age and sex. Considering previous studies that reported violent suicide attempts to be significantly more frequent among men and those of younger age,323334 there are limitations in interpreting the results of these studies.
Two previous studies dealt with the association between suicide attempt method and TCI. In a study of suicide attempters in Korea, novelty-seeking was higher in the group who tried both non-suicidal self-injury (NSSI) and suicide attempt than the group who tried only suicide attempt.35 Also, in a previous study in Iran, both novelty-seeking and self-transcendence were higher and self-directedness and cooperativeness lower in non-violent suicide attempters than in the normal control group, and these subscales were found to mediate non-violent suicide attempts, respectively.36 It is unclear whether the high novelty-seeking found in these studies is associated with the risk of non-violent methods or non-suicidal intent of self-injury. Therefore, it is necessary to limit research subjects to suicide attempters, adjust demographic variables such as age and sex, and compare the temperaments and characters of groups who used fatal and non-fatal methods of suicide to find temperament traits to predict fatal method of suicide attempt.
Mediation analysis was used in previous studies of the effects of childhood trauma on temperament and character and related mental health problems.373839 Traumatic experiences in childhood not only cause structural changes in the limbic system of the brain, but also cause permanent changes in social cognitive aspects such as emotional regulation and social trust.40 These changes lead to a decrease in stress coping ability that is reflected in changes in temperament and character, thereby causing a variety of psychopathology in the future. If so, the influence of childhood trauma on suicide-related behavior could also be explained as a mediating effect of temperament and personality.
Using the data from the Korean Cohort for the Model Predicting a Suicide and Suicide-related Behavior (K-COMPASS), we studied the populations with a history of suicide attempts. We verified differences in scores on the Temperament and Character Inventory-Revised (TCI-R) between 1) participants with and without early trauma, and 2) participants with and without a history of use of fatal methods of suicide attempt. We also investigated whether these differences mediate the relationship between early trauma and fatal methods of suicide attempts.
Go to : 
METHODS
Participants and procedure
K-COMPASS is a cohort study that tracks the long-term course of suicidal ideators and suicide attempters. In this project, two cohorts were tracked simultaneously: a community-based cohort (n = 241) and a hospital-based cohort (n = 559), each consisting of suicidal ideators and suicide attempters. The study began on September 1, 2015, and an extended study has been underway since July 1, 2019.
The community-based cohort recruited people from selected community visits or other community facilities at eight community-based mental health centers across the country, and the hospital-based cohort was organized by eight tertiary hospitals in major regions of Korea, recruiting patients who came to the outpatient or emergency room. Suicide ideators were defined as those who complained of serious suicide ideation at the time of registration, and suicide attempters as those who attempted to end their lives within one month of registration. People with intellectual disabilities or organic brain disease were excluded. For more details on the research performance of this study or the underlying characteristics of the participants, please refer to the authors' previous papers.4142
Among the 800 participants who were registered by May 31, 2019, 118 participants who completed all the clinical assessments (described in Measurements) were included. Among them, 92 participants who reported a history of suicide attempts were analyzed. Participants under the age of 19 were excluded from analysis because they had completed the Junior Temperament and Character Inventory (J-TCI) instead of the TCI for adults.
Measurements
Socio-demographic and clinical variables
At the first visit, socio-demographic and clinical characteristics were assessed by psychiatrists, research nurses, and social workers. Medical and psychiatric history, including current and previous suicidal thoughts and attempts, were evaluated based on the participants' self-report. Among the 17 people who reported that they had bipolar disorder, 13 reported that they also had major depressive disorder. According to the diagnostic criteria of the DSM-IV-TR, these subjects were classified as having bipolar disorder only. Psychiatric diagnosis was also made using the Korean version of the Mini International Neuropsychiatric Interview (K-MINI). The K-MINI is a semi-structured interview tool for psychiatric diagnosis43 using the Diagnostic and Statistical Manual of Mental Disorder, Fourth Edition, Text Revision (DSM-IV-TR) criteria.44 It was verified in Korean, showing good validity compared to the diagnosis of a psychiatrist (κ = 0.71 for major depressive disorder).45 Psychiatric rating scales were also performed and evaluated. All assessors had formal training sessions and consensus meetings before administering the scales, and the research coordinator from each research site participated in Internet-based video conference every month to preserve the quality of the research. Among the scales and characteristics that were evaluated, the major tools used in this study are as follows.
Early Trauma Inventory Self-Report Short Form (ETISR-SF)
The ETISR-SF is a self-report questionnaire that assesses the existence of physical, emotional, sexual abuse and overall traumatic experience, consisting of 27 items grouped into four categories of trauma: general trauma, physical abuse, emotional abuse, and sexual abuse.46 Participants were instructed to list all the items they had experienced before the age of 18 and check the item that had the greatest impact on themselves. Participants were regarded to have experienced early trauma only if they felt strong fear, horror, or helplessness, or feel separated from the body or as if they were in a dream during the event. The Korean version of the ETISR-SF has been reported to have good convergent and divergent validity.47 In order to evaluate the validity of the Korean version of the ETISR-SF, they compared its correlations with the Childhood Trauma Questionnaire-Short Form (CTQ-SF),48 Beck Depression Inventory (BDI),49 and Beck Anxiety Inventory (BAI).50 The measure was more strongly correlated with the CTQ-SF (r = 0.691) than with the BDI (r = 0.424) or BAI (r = 0.397) and was regarded as having good validity. The internal consistency of the ETISR-SF was also excellent, with a value of Cronbach's α = 0.869.47
TCI-R
The TCI is a self-report questionnaire consisting of 240 items based on Cloninger's unified biopsychosocial model. The latest version is the TCI-R.51 It evaluates four temperament and three-character dimensions that persist in an individual. Of the temperament dimensions, novelty seeking is characterized by frequent exploratory behavior and strong excitement for new stimuli. Harm avoidance tends to react strongly to painful stimuli and avoids punishment. Reward dependence is a trait with sensitivity to rewards and tendency to maintain the behavior for the sake of rewards in the future. Persistence refers to maintaining existing behavior despite frustration and fatigue. Of the character dimensions, self-directedness is the ability to adjust and adapt one's behavior to individual values and goals; cooperativeness involves social tolerance, empathy, compassion, and a tendency to help others; and self-transcendence is spiritual maturity, identification with others, and altruism. Each dimension comprises five to ten questions scored on a Likert scale.
Assessment of fatal methods of suicide attempts
Interviews evaluated the most fatal attempts of suicide in the participants' life among those who had a history of suicide attempts at or before the time of study participation. According to previous studies of suicide attempts and committed suicides in the U.S. and Korea, drug poisoning and stabbing showed relatively low fatality, while gas poisoning, pesticide poisoning, hanging, drowning, and jumping showed high fatality.8952 Based on the results of these studies, we regarded drug poisoning and self-injury as non-fatal methods of suicide attempt, and methods such as hanging, pesticide poisoning, jumping, gas inhalation, drowning, and gunfire as fatal methods. In the case of a participant who committed multiple suicide attempts using fatal and non-fatal methods, respectively, the participant was evaluated as being in the fatal group.
Statistical analysis
All analyses were performed using SPSS 23 (IBM SPSS Statistics for Windows, Version 23.0; IBM Corps, Armonk, NY, USA), and were considered statistically significant when P < 0.05. The differences in the socio-demographic and clinical characteristics among the participants were compared according to the presence or absence of early trauma and use of fatal methods of suicide attempt. The continuous variables were compared with Student's t-tests and categorical variables with χ2 tests.
When comparing the fatal and non-fatal groups on the socio-demographic and clinical variables, sex and presence of a psychiatric history were statistically significantly different. Therefore, an analysis of covariance (ANCOVA) was performed on the differences in TCI-R scores of the groups with and without early trauma and with and without suicide attempts using fatal methods, respectively, adjusted for age, sex, and presence of a psychiatric history. To evaluate the mediating effect of self-transcendence in the relationship between early trauma and fatal methods of suicide attempt, PROCESS macro for SPSS was used. PROCESS is a method to check the confidence interval of the effect of the independent variable on the dependent variable using bootstrapping.53 In this analysis, the mediation effect is significant when the 95% confidence interval for the indirect effect does not contain zero. Early trauma was used as an independent variable, fatal methods of suicide attempt as a dependent variable, and self-transcendence as a mediator. A simple mediation model (PROCESS Model 4) was used with 5,000 bootstraps, and age, sex, and presence of a psychiatric history was adjusted as covariates.
Ethics statement
This study was reviewed and approved by the Institutional Review Board of Seoul National University Hospital (H-1505-050-671) and all other participating centers. Informed consent was submitted by all subjects when they were enrolled.
Go to :
RESULTS
Comparisons of socio-demographic and clinical characteristics
Among the 92 participants analyzed, 34 reported a history of suicide attempts using fatal methods and 58 reported non-fatal methods. Table 1 shows the difference in socio-demographic and clinical characteristics between the two groups.
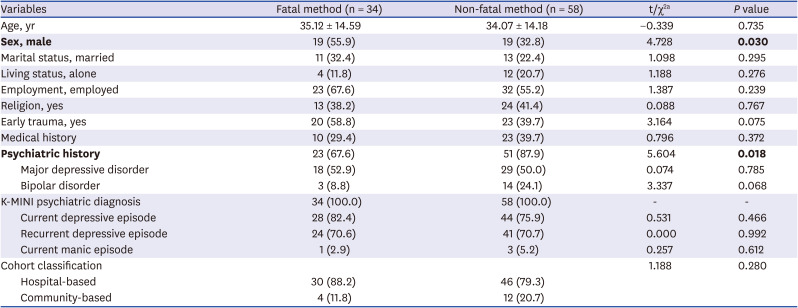
Table 1
Comparisons of characteristics between the fatal and non-fatal suicide method groups
Values are presented as mean ± standard deviation or number (%). Bold indicates statistically significant results.
aχ2 test for categorical variables and Student's t-test for continuous variables were performed.
![]()
The proportion of males was greater in the fatal group than the non-fatal group (55.9% vs. 32.8%, P = 0.030). Other socio-demographic variables did not differ significantly between the two groups. On the other hand, among the clinical variables, the fatal group reported significantly fewer participants with a psychiatric history (67.6% vs. 87.9%, P = 0.018), but no difference were found between the two groups in K-MINI diagnosis, because all participants were evaluated as having psychiatric disorders. There was no difference in the other variables.
Comparisons of TCI-R
The fatal group showed statistically significantly higher self-transcendence values than the non-fatal group (27.71 ± 13.78 vs. 20.97 ± 12.27, F = 6.854, P = 0.010) (Table 2). Among the three subscales of self-transcendence, transpersonal identification (subscale 2) was higher in the fatal group (7.91 ± 5.49 vs. 3.69 ± 4.01, F = 17.698, P < 0.001), while there was no difference in the other two subscales. There were no significant differences between the two groups in the other dimensions of TCI-R.
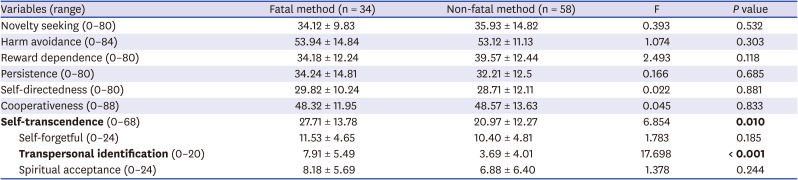
Table 2
Comparisons of TCI-R between the fatal and non-fatal suicide method groups (ANCOVA)
Values are presented as mean ± standard deviation. Bold indicates statistically significant results. All variables were adjusted for age, sex, and presence of a psychiatric history.
TCI-R = Temperament and Character Inventory-Revised, ANCOVA = analysis of covariance.
![]()
On the other hand, of the 92 participants analyzed, 43 reported a history of early trauma and 49 did not, and TCI-R was also compared between these two groups (Table 3). As a result, the early trauma group also showed statistically significantly higher self-transcendence than the group without early trauma (28.05 ± 14.30 vs. 19.43 ± 10.73, F = 13.503, P < 0.001). All three subscales of self-transcendence, self-forgetful (subscale 1: 12.53 ± 4.07 vs. 9.31 ± 4.85, F = 11.116, P = 0.001), transpersonal identification (subscale 2: 6.88 ± 5.83 vs. 3.82 ± 3.67, F = 10.805, P = 0.001), and spiritual acceptance (subscale 3: 8.63 ± 6.26 vs. 6.24 ± 5.88, F = 6.493, P = 0.013), were higher in the early trauma group.
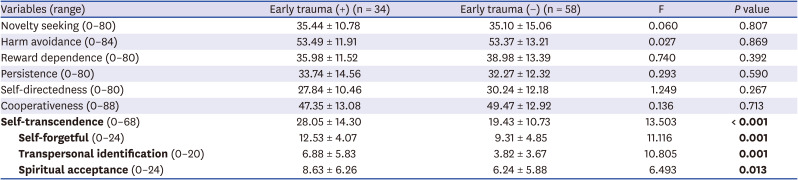
Table 3
Comparisons of TCI-R between groups with and without a history of early trauma (ANCOVA)
Values are presented as mean ± standard deviation. Bold indicates statistically significant results. All variables were adjusted for age, sex, and presence of a psychiatric history.
TCI-R = Temperament and Character Inventory-Revised, ANCOVA = analysis of covariance.
![]()
Mediation model
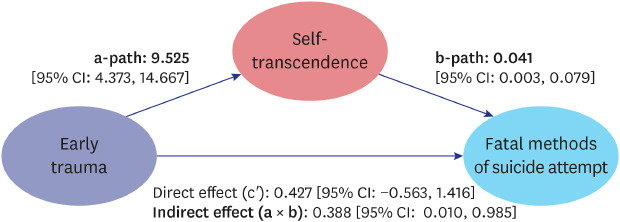
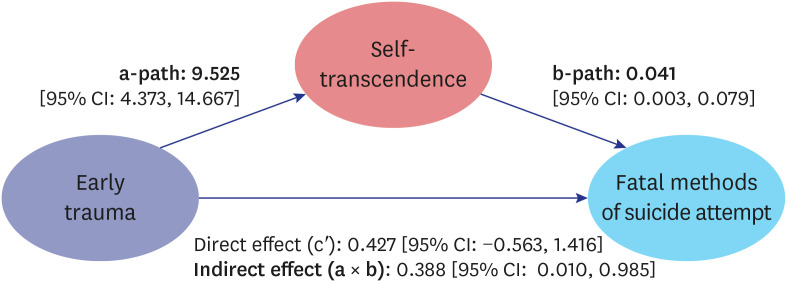
In the relationship between early trauma and fatal methods of suicide attempt, the mediating effect of self-transcendence adjusted for age, sex, and presence of a psychiatric history was as follows: The direct effect was not significant with 95% CI = 0.427 (−0.563, 1.416), while the indirect effect was significant with 95% CI = 0.388 (0.010, 0.985), thereby confirming that self-transcendence mediates the relationship between early trauma and fatal methods of suicide attempt (Fig. 1). Mediation analysis was performed again, with each of the three subscales of self-transcendence as a mediator. As a result, only subscale 2: transpersonal identification showed a significant indirect effect; the direct effect was 95% CI = 0.237 (−0.789, 1.263), and the indirect effect was 95% CI = 0.600 (0.188, 1.411).
Go to :
DISCUSSION
This study found that among those with experience of suicide attempt, the scores on the TCI scale for self-transcendence were higher both in the group with a history of early trauma and in the group with a history of suicide attempts using fatal methods. In addition, the mediation analysis showed that self-transcendence mediates the relationship between early trauma and fatal methods of suicide attempt.
In this study, unlike previous studies, only self-transcendence was found to be higher in participants with early trauma. We suggest that the psychiatric disorder might have affected this difference as a confounder in previous studies performed in the general population. Early trauma is associated with a variety of psychiatric disorders, including mood disorders. These disorders usually exhibit features such as high novelty seeking, harm avoidance, and self-transcendence, and low persistence, self-directedness, and cooperativeness.545556 It is possible that the TCI changes seen in early trauma in previous studies were actually the features of psychiatric disorders. However, our study included only suicide attempters, among whom there was no difference in the presence of a psychiatric history in the groups with and without early trauma. In addition, we adjusted presence of a psychiatric history as a covariate in the analysis. Therefore, self-transcendence, which showed a statistically significant difference—even after the TCI difference associated with psychiatric disorder caused by early trauma was offset—may be a personality trait more directly related to early trauma itself than the other traits.
In general, self-transcendence is a personality trait associated with experiencing spiritual thoughts, expanding the boundaries of an individual to perceive oneself as a part of the universe, and diminishing self-centered and selfish motives.5758 It is defined as expanding one's boundaries intrapersonally (toward greater awareness of one's philosophy, values, and dreams), interpersonally (to relate to others' and one's environment), and transpersonally (to connect with dimensions beyond the typically discernible world).59 Healthy self-transcendent people are known to adapt better when faced with inevitable pain or death. They are patient, full of imagination, and easily influenced by art, but usually have low self-esteem and poor rationality and scientific objectivity.60
In his seven-dimensional model of personality, Cloninger defined self-transcendence in relation to the experience of self's spiritual aspect, and suggested self-forgetful, transpersonal identification, and spiritual acceptance as its subcategories.61 Self-forgetful people tend to forget themselves when they are deeply immersed in love or work, which is also a hallmark of high levels of meditation. Those who score high on transpersonal identification feel a strong bond to nature and the universe. Those with high spiritual acceptance trust transcendental phenomena and regain vitality and security through them.60
In healthy individuals, self-transcendence has positive qualities such as creativity and altruism. However, it is known that self-transcendence also stands for vulnerability to psychosis and schizotypy when the subject scores low in other personality areas such as self-directedness and cooperativeness.57 The participants in our study have a history of suicidal attempts and their prevalence of psychiatric pathology is greater than that of the general population, so the high self-transcendence seen in this study may be associated with unhealthy defense mechanisms, such as paranormal beliefs and dissociation.626364
For children experiencing trauma, a withdrawal into fantasy may be a powerful defense mechanism to cope with emotional difficulties that is associated with a high self-transcendence, suggesting a spiritual and transcendental defense mechanism.65666768 In addition, previous studies have reported associations between PTSD and self-transcendence. Individuals with traumatic experiences tend to distort perceptions of themselves and the environment, and PTSD symptoms develop as they use inefficient defense mechanisms that might be reflected in self-transcendence.69 Also, if a person had such an experience in childhood, these defense mechanisms may appear as a lasting personality trait.
Among the TCI findings suggestive of the risk of suicide-related behavior in previous studies, only high self-transcendence was associated with fatal methods of suicide attempt in our study. Most previous studies including those mentioned earlier that assessed the association of TCI and the risk of suicide-related behaviors, were studies of patients with mood disorders, such as major depressive disorder.242526272870 In these studies, TCI scores might have varied depending on the severity of the affective symptoms of the participants. In the case of harm avoidance, for example, it is reported to be higher in depression and reduced after treatment with an antidepressant.71 In a study of patients with remitted depression, self-transcendence and persistence but not harm avoidance were higher in the suicide attempt group than the control.70 Temperament is inherited and is usually thought to last a lifetime, but it can also be a marker reflecting the severity of depression, as with high harm avoidance, low self-directedness and cooperativeness.72 Since severe depression is a risk factor for suicide-related behavior,737475 the previously reported association between suicide-related behaviors and harm avoidance, self-directedness, and cooperativeness may be attributed to the confounding effect. Self-transcendence may be the TCI dimension that strongly suggests the risk of suicide after the effect of psychiatric symptoms, including mood episodes, is excluded.
More specifically, self-transcendence subscale 2: transpersonal identification, in particular, was commonly increased in both the early trauma group and the fatal group in the ANCOVA, and appeared to mediate the relationship between early trauma and fatal methods of suicide attempt. Transpersonal identification indicates a sense of unity with objects outside the individual self,21 and was shown to have a significant correlation with psychopathology in previous studies.76 This subscale reflects solidarity with others in healthy people, but is also related to self-harm behavior aimed at self-punishment because it reflects unselfish self-sacrifice.29 This further reinforces the earlier assumption that self-transcendence increases the risk of fatal suicide attempts by suggesting an unhealthy defense against stress.
Meanwhile, this study reported that males and those without a psychiatric history have a greater risk of fatal methods of suicide attempt. It is well known that men use more fatal methods of suicide attempts than women,77 but reports on the effects of a psychiatric history on the risk of suicide attempts are divided. In a previous study conducted in China, risky methods were often chosen in the psychiatric disorder group,78 but our previous study in Korea reported results consistent with the current study.79 It is thought that psychiatric patients have easy access to drugs, and less fatal self-harm may be repeated by those with personality disorder.8081
More crucially, all participants in our study were evaluated as having psychiatric disorders on the K-MINI. Regarding the high specificity of K-MINI diagnosis (0.91 for major depressive disorder, 1.0 for current manic episode),45 it is possible that the fatal group did not receive sufficient psychiatric diagnosis and treatment. According to the Survey of Mental Disorders in Korea, only 22.2% of the psychiatric patients used mental health services and 16.6% received medical treatment from a psychiatrist.82 This failure to receive treatment is due to stigma about psychiatric treatment or a lack of awareness of treatment and service institutions.83 This survey also found that 68.7% of suicide attempters experienced mental disorders. It is also possible that the participants in our study were afraid of stigma and did not disclose their own psychiatric history. Therefore, it is necessary to pay close attention to the risk of suicide even in people without a psychiatric history, while promoting a policy to eliminate stigma against psychiatric treatment and improve access to mental health services.
This study is the first to analyze early trauma and the method of suicide attempts in Koreans, and it has representativeness by recruiting participants from hospitals and communities in a variety of regions in Korea to minimize selection bias. However, our research also has some limitations. First, as this is a cross-sectional study, reverse causation between early trauma, self-transcendence, and fatal methods of suicide attempt was not excluded. Suicidal attempts in a fatal method are life-threatening and can also act as a traumatic experience. Considering the relationship between early trauma and self-transcendence, suicide attempts may also have increased self-transcendence in the same way as early trauma. In addition, since this study consisted of two cohorts, a community cohort and a hospital cohort, the results might have been different had the composition ratio of the two cohorts changed. Lastly, child trauma cannot be free of recall bias because it was evaluated based on the respondents' retrospection. However, the memory of childhood trauma is relatively stable and generally appears in the direction of underestimation rather than overestimation, with rare false-positivity.848586 Therefore, the recall bias would not be large, and the possibility of reaching an incorrect conclusion through recall bias would not be high in the current study. If a separate scale to evaluate the validity of the response, such as the Minimization/Denial scale of the CTQ,87 were to be administered, the effect of reporting bias could be assessed more objectively.
In conclusion, this study has shown that both early trauma and use of fatal methods of suicide attempt are related to self-transcendence. We also showed the relationship between early trauma and fatal methods of suicide attempt to be mediated by self-transcendence. These findings suggest that self-transcendence may be associated with unhealthy defenses against external stress and suicide-related behavior for self-punishment, as well as that self-transcendence may serve as a marker for greater suicide risk. More comprehensive and prospective research on early trauma and self-transcendence is expected.
Go to :
 XML Download
XML Download