

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Gastroesophageal reflux disease (GERD) is a global problem, with a high prevalence.1 The association between GERD and lung disease has been discussed for a long time.234 The primary pathophysiology of GERD is acid reflux and micro-aspirations caused by the reflux of gastric contents to the esophagus, trachea, bronchus, and both lungs.5 This can cause lung injuries, pulmonary inflammation, fibrosis, or esophagobronchial-cardiac reflexes.67891011 GERD is a crucial comorbidity of asthma, chronic obstructive pulmonary disease (COPD), bronchiectasis, and idiopathic pulmonary fibrosis (IPF).1213141516
GERD can aggravate respiratory symptoms or exacerbate respiratory disease symptoms.1718192021 However, it is unclear whether GERD affects lung function in individuals with normal lung function. If it does, the association may give an important clue to understanding the pathophysiology of lung function decline in patients with respiratory diseases.
We sought to determine the long-term effects of erosive reflux esophagitis on lung function in patients with normal lung function. We hypothesized that declines in lung function were accelerated by erosive reflux esophagitis. We investigated the longitudinal lung function changes in a population of individuals with normal lung function.
METHODS
Study design and population
This study was a retrospective cohort study based on the Gene-environment Interaction and Phenotype (GENIE) cohort, which included patients who visited the Seoul National University Hospital Healthcare System Gangnam Center between February 2014 and October 2016. The participants who visited this healthcare center were self-visitors for routine health check-ups. This study was performed in Seoul, metropolitan city in Korea, and all the participants were Asians.
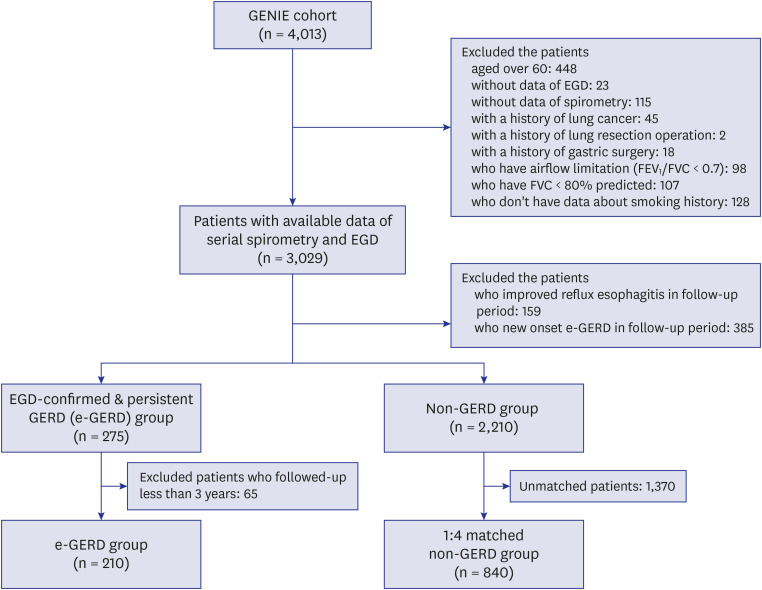
Patients were recruited between 2014 and 2016; however, their medical data from 2005 to 2019 were collected for analysis. Adults aged 30–60 who underwent at least two esophagogastroduodenoscopies (EGD) simultaneously with spirometry were included. Because we only included patients with normal lung function, we excluded those with restrictive lung function (forced vital capacity [FVC] < 80%) or airflow limitations (initial forced expiratory volume in 1 second [FEV1]/FVC < 70). We also excluded patients who had a history of lung cancer, lung resection, or gastric surgery. Since erosive reflux esophagitis can improve within weeks of initiating medical treatment and we wanted to elucidate the long-term and persistent effects of reflux esophagitis on lung function, only patients with more than two EGD results were enrolled. We excluded patients with improved or newly diagnosed reflux esophagitis during the follow-up periods. Also, subjects followed-up for fewer than three years were excluded. Patients without data on smoking status were excluded (Fig. 1).
Definitions and measurements
When persistent reflux esophagitis was found during a follow-up EGD, we regarded the case as a patient with endoscopically confirmed erosive reflux esophagitis. The erosive reflux esophagitis group was defined as patients with evidence of persistent, erosive reflux esophagitis across two or more EGD studies. We only enrolled patients with the same erosive grade of erosive reflux esophagitis in multiple EGD records or patients with aggravated erosive reflux esophagitis in followed-up EGD records. We excluded patients who had improved reflux esophagitis followed up EGD or showed new onset erosive reflux esophagitis in followed-up EGD in either patient's group or control group.
The non-GERD group was defined as patients who had never shown erosive reflux esophagitis in EGD during the follow-up period. Matched controls were randomly selected from the non-GERD group based on sex, age, and the first spirometry year by propensity matching (Fig. 1).
The severity of erosive reflux esophagitis was divided into four groups (A, B, C, and D) with the criteria of Los Angeles (LA) classification, which correlates well with acid reflux tests.2223 The LA grade was determined by the initial EGD grade.
Spirometry data included FEV1, FVC, and FEV1/FVC, which were measured in pre-bronchodilator status. The resultant values are presented as absolute (L) and predicted values (% predicted) estimated according to Korean normal predictive values of spirometry.24 The spirometry was performed following the recommendations of the American Thoracic Society guidelines.2526 The initial date of spirometry was when the erosive reflux esophagitis was diagnosed or ruled out in the study population. We reviewed patients' demographics (age, sex, body mass index [BMI], smoking status), spirometric data, comorbidities (including malignancy), and surgical history.
The primary outcome was the annual estimated pulmonary function change, and all outcome measures were based on serial spirometry data. Another outcome was the proportion of patients who developed COPD. When the FEV1/FVC was less than 0.7 during the follow-up period, we considered that an obstructive pulmonary disease had developed.
Statistical analysis
Student's t-test was used to analyze continuous variables, and the Pearson χ2 test or Fisher's exact test was used for analyzing categorical variables in describing the baseline characteristics of the study population. The mean change in lung function was defined as the annual change between the last and the first spirometry results. We compared mean changes in FVC, FEV1, and FEV1/FVC from serial spirometry between patients with and without erosive reflux esophagitis. A longitudinal linear mixed-effect model with random intercept and the random slope was applied to assess adjusted annual spirometric changes. Age, sex, BMI, and smoking history were adjusted to analyze the annual spirometric change. We carried out a sensitivity analysis of adjusted annual spirometric changes in the erosive reflux esophagitis group by LA classification. Kaplan–Meier estimation with log-rank test and Cox proportional hazards regression models were used to analyze the development of COPD. A P < 0.05 indicated a statistically significant difference. All the analyses were conducted in STATA software (version 13.1; Stata Corp., College Station, TX, USA).
RESULTS
Characteristics of study participants
Among the 4,013 participants in the GENIE cohort, 3,029 met all inclusion/exclusion criteria and had available data for both serial spirometry and EGD. Patients who had insufficient medical data (n = 266), restrictive lung volumes (n = 107), airway limitation (n = 98), lung cancer (n = 45), history of gastric surgery (n = 18), history of lung resection surgery (n = 2), and patients older than 60 years (n = 448) were excluded. Among the 3,029 patients, 544 patients who had inconsistent GERD disease status were excluded.
Among the patients who met the erosive reflux esophagitis criteria, 65 had fewer than three years follow-up and were therefore excluded. A total of 210 patients with erosive reflux esophagitis were eligible for analysis. We later selected 840 controls who were matched to patients with erosive reflux esophagitis 4:1 (Fig. 1).
The baseline characteristics of the study population by erosive reflux esophagitis status are described in Table 1. The participants' mean age was 49.5 years. Males predominated (91%), and the mean FEV1 was 3.5 L (106.4%). Patients with erosive reflux esophagitis had a significantly higher mean BMI and were more likely to smoke compared to the control group. The mean follow-up period was six years, with the GERD group having a slightly shorter follow-up period than the non-GERD group (5.6 vs. 6.3 years, P < 0.001). In most patients, spirometry was performed at 1- or 2-year intervals during the follow-up period. In the erosive reflux esophagitis group, most of the patients had low severity (LA class A, 79%), and there were no patients in class D (Table 1).
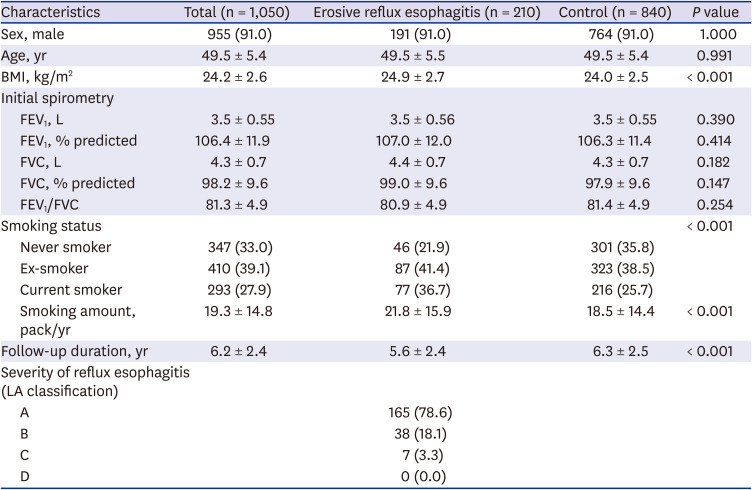
Table 1
Baseline characteristics of study population
Data were described as number (%) for numeric variables and mean ± standard deviation for continuous variables.
BMI = body mass index, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, LA classification = Los Angeles classification.
![]()
Impact of erosive reflux esophagitis on annual spirometric changes
Table 2 shows the absolute mean annual change of spirometric data. In the erosive reflux esophagitis group, the absolute mean annual decreases of FEV1 and FVC were 62.0 and 72.0 mL. The same values were 60.9 mL (FEV1) and 65.4 mL (FVC) for the control group. There were no significant between-group differences in the annual absolute and age-matched percentage change of spirometric parameters.

Table 2
Mean annual spirometric changes in erosive reflux esophagitis and control group
![]()
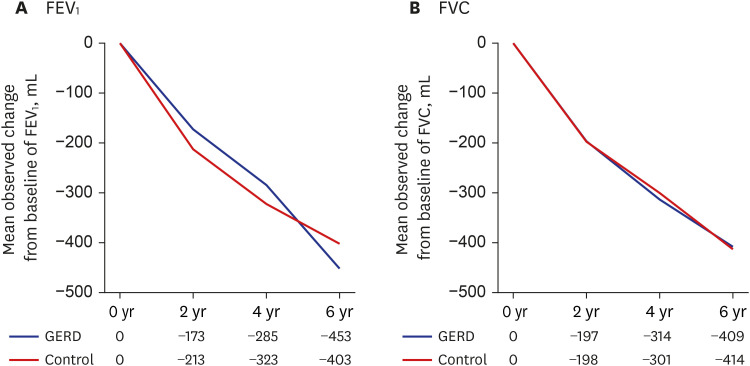
When we look at declining trends within the sequential spirometric data during each two-year interval, there were no significant between-group differences in the changes observed for FEV1 and FVC (Fig. 2). Erosive reflux esophagitis did not appear to contribute to lung function decline in these patients.
After adjusted age, sex, BMI, and smoking status, in patients with erosive reflux esophagitis, the estimated annual decline in FEV1 was 51.8 mL (95% confidence interval [CI], 43.7–59.8) while it was 46.8 mL (95% CI, 43.0–50.6) in the control group. Age, sex, BMI, and smoking status were adjusted, but there was no significant difference between the groups (P = 0.270). The estimated annual decline in FVC showed no difference between the two groups. (55.8 mL/yr for the erosive esophagitis group vs. 50.5 mL/yr for the control group, P = 0.350) (Table 3).

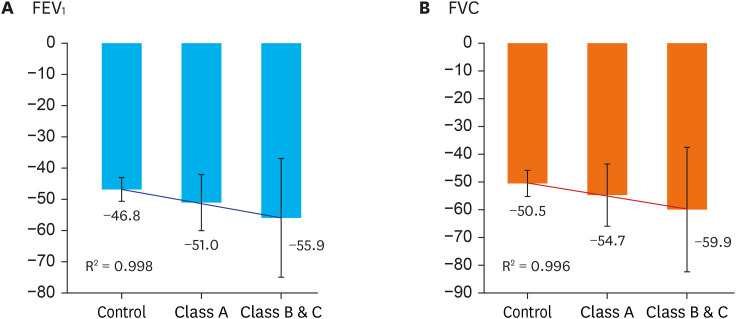
Fig. 3 and Supplementary Table 1 present data on age, sex, BMI, and smoking status adjusted estimated annual lung function change by LA classification. Patients with erosive reflux esophagitis did not have significantly different values for FEV1 change or FVC change compared to controls (−51.0 vs. −46.8 mL/yr, P = 0.731 or −50.5 vs. −54.7 mL/yr, P = 0.497, respectively). Patients with advanced grades of esophagitis (LA classification B or C) did not show any significant differences in adjusted annual FEV1 change or FVC change compared to controls (−55.9 vs. −46.8 mL/yr, P = 0.731 and −59.9 vs. −54.7 mL/yr, P = 0.497). The trend in annual decline with LA classification was linear for FEV1 and FVC, but not statistically significant (R2 = 0.998 and R2 = 0.996, respectively) (Fig. 3). Additionally, changes in FEV1 and FVC between the severity classes were not statistically significant (Supplementary Table 1).
COPD development
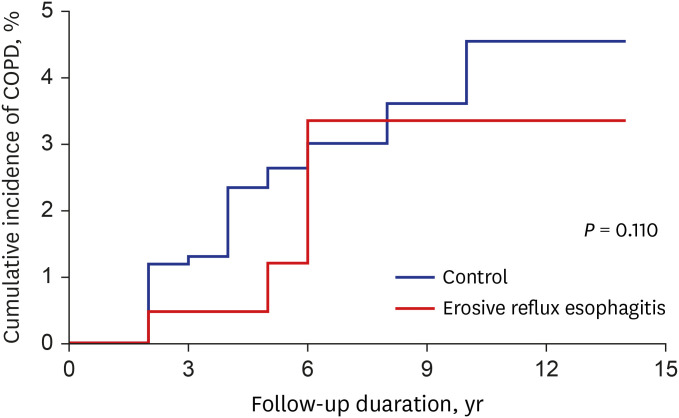
In the follow-up period, there were no significant between-group differences between the erosive reflux esophagitis group and controls for the development of COPD (2.4% vs. 2.8%, P = 0.760) (Supplementary Table 2) and estimated cumulative COPD incidence using the Kaplan–Meier curve (P = 0.524) (Fig. 4). Even after adjusting for age, sex, and BMI, there was no significant between-group difference in COPD development. Very few participants demonstrated restrictive pulmonary disease (FVC < 80% predicted) during the follow-up period (only one case in the erosive reflux esophagitis group and four cases in the control group).
DISCUSSION
This study was a longitudinal study of lung function changes in erosive reflux esophagitis patients compared with non-GERD control patients. In the change in FEV1, FVC measured by spirometry, there were no significant differences in lung function decline between erosive reflux esophagitis and non-GERD control group. In the analysis, according to the severity of erosive reflux esophagitis, there were no significant differences in lung function change compared to the control group. The estimated COPD diagnosis in the followed-up period analyzed by Kaplan–Meier estimates and the log-rank test showed no significant difference between the erosive reflux esophagitis and control groups.
One previous study of patients with asthma showed no significant difference in lung function change between the GERD and control groups.20 One cross-sectional study of GERD and control groups, only diffusing capacity was decreased in the GERD group. There were no significant between-group differences in FEV1 and FVC.27 A recent study of patients with COPD showed no significant longitudinal lung function changes in patients with GERD compared to controls. However, there was a high portion of rapid FEV1 declining patients in GERD patients compared to non-GERD patients.28 As was the case for the previous study, we found no significant changes in annual lung function between patients with and without erosive reflux esophagitis.
This was the first study to evaluate longitudinal spirometric changes in adults with normal lung function who had been endoscopically diagnosed as erosive reflux esophagitis. Moreover, GERD severity was evaluated using LA classification, so that changes in lung function could be analyzed according to GERD severity.
As we hypothesized that GERD might be a precipitating factor for developing chronic respiratory disease accompanying the spirometric changes, our target population was restricted to healthy adults with normal pulmonary function. Also, we limited patients' initial age to 60 years old to avoid the potentially confounding effects of age-related changes in lung function. We also carefully reviewed each patient's smoking history and made appropriate adjustments prior to analyzing lung function change.
This study had some strengths. First, we used strict criteria for erosive reflux esophagitis. Only patients with GERD and multiple EGDS—and without a history of gastric surgery—were included. Second, our control cohort was relatively large and each patient had repeated EGD and spirometric tests. We also matched the erosive reflux esophagitis and control groups using propensity matching. This showed only a few significant differences in baseline characteristics (Table 1). Finally, no study had a longer follow-up duration than ours in terms of EGD findings and spirometry. However, the median follow-up period was 5–6 years, and more time may be needed to detect lung function changes due to reflux.
Our study also had some limitations that warrant consideration. All spirometric examinations were performed in a pre-bronchodilator setting that was not specifically designed to diagnose obstructive lung diseases. Furthermore, non-erosive reflux disease (NERD) patients defined as a subcategory of GERD characterized by reflux-related symptoms in the absence of esophageal mucosal erosions or breaks at endoscopy29 were not diagnosed as GERD in this study. Still, some patients with NERD could have accidentally been included in the non-GERD group. Considering this, our results may not accurately reflect the general symptomatic population of patients with GERD. However, we believe that our results are reasonably representative of patients with erosive reflux esophagitis.
Most patients with erosive reflux esophagitis were LA class A. Very few patients exhibited severe erosive reflux esophagitis; therefore, our statistical power is insufficient for the detection of patients with severe erosive esophagitis population. Patients with more severe disease tended to demonstrate more rapid annual declines in mean FEV1 and FVC than those with milder disease, although the difference did not rise to the level of statistical significance (Fig. 3). Future studies should examine lung function changes in patients with severe reflux esophagitis.
In conclusion, among patients with initially normal lung function, erosive reflux esophagitis did not influence declines in lung function compared to non-GERD controls. The cumulative incidence of COPD was not significantly different between patients with and without erosive reflux esophagitis.
 XML Download
XML Download