

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
More than 120 hand/upper extremity transplant procedures have been performed worldwide following the first successful hand transplantation performed by the U.S. Louisville team in 1991.1 This is considered as ‘crossover therapy’ from the realm of experimental to the mainstream as a standard of care for the treatment of amputation23 or as a “controlled standard” for the appropriately selected cases of amputation.4 Recently published data demonstrate improvements in function and quality of life, delivering highly encouraging short- and intermediate-term outcomes.56789101112
In Korea, however, there was no vascularized composite tissue allotransplantation (VCA) until 2017. Although brain death was formally recognized in Korea in 2000 for organ donation, no hand/arm harvesting was possible because the Korea Organ Transplantation Act (KOTA) had then only allowed eleven internal organs plus bone marrow, eyeballs, and other internal organs or tissue prescribed by Presidential Decree, to be recovered and transplanted for functional recovery, in effect making it illegal to harvest hand/arm from a potentially matched brain-dead patient. Due to this status, Korean National Health Insurance is precluded, making the costs prohibitively high to patients.
There was also cultural and academic resistance. Prejudice against having the remains of the deceased dismembered acts as a substantial hindrance for hand/arm donation. Korean people's strong desire to have the carnal body intact even after death makes harvesting a hand that much more complicated and required concerted and multifaceted efforts.13 A missing arm/hand is difficult to conceal during the funeral viewing. Academia was also somewhat hesitant to push forward with VCA in Korea, mainly because of the unfamiliarity with the topic and the aforementioned cultural attitudes.
Despite these problematic obstacles, W Hospital in Korea successfully performed the nation's very first hand transplantation laying the groundwork for the VCA program in Korea. The purpose of this paper is to report on how our team at W Hospital overcame these unfavorable financial, social, and legislative environments to make VCA possible in Korea. We would like to share our protocol and functional outcomes of successful hand transplantation in our first three years. The authors hope that surgically capable physicians in other countries facing similar issues would perhaps be inspired and guided by our experience.
Go to : 
METHODS
Legal approach
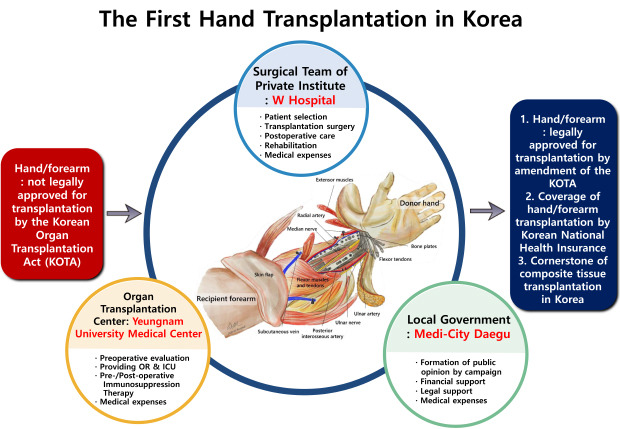
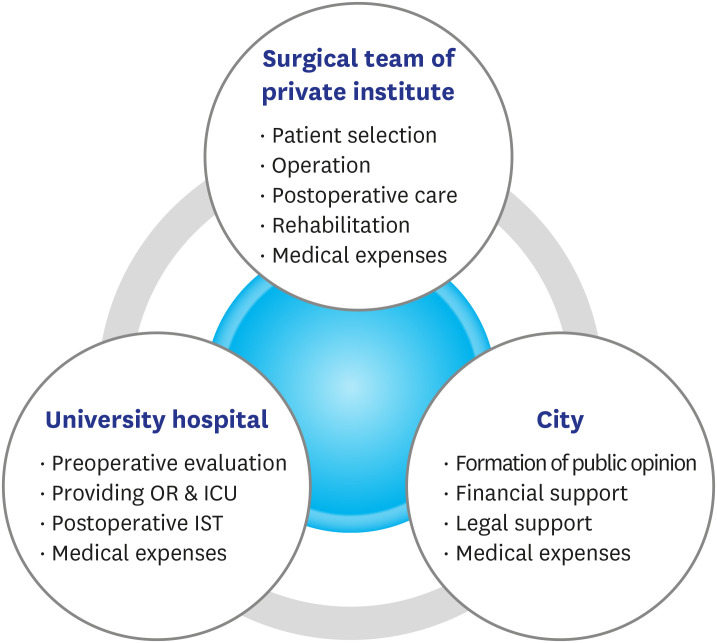
To change the legislative status of VCA, multiple meetings were held with local congress members to initiate a formal congressional proposal to amend the KOTA to include hand/arm transplantation. No meaningful progress was made, however. The authors then applied for hand VCA to be registered as a ‘New Health Technology’ to the Ministry of Health and Welfare (MOHW) in 2010 and received approval at the federal level.14 On Feb 28, 2016, VCA was chosen as the “Representative Innovative Medical Technology of the City of Daegu, Korea” which resulted in the signing of a memorandum of understanding (MOU) to share legal and financial responsibility for the operation (Fig. 1). Another MOU was signed with Yeungnam University Medical Center (YUMC), Daegu, Korea, which provided an operation room, intensive care unit, and postoperative management of immunosuppression for the W Hospital team to perform the actual operation.
Financial affairs
An MOU was signed with Daegu, Korea, essentially securing funds to cover all medical expenses and public awareness campaigns. Another MOU was signed with the YUMC that agreed to cover all hospitalization costs for the main operation. W Hospital was responsible for all of the remaining expenses, including medical instruments and supplies, operation fees, postoperative rehabilitation, immunosuppression drugs, secondary biopsy, additional operations and admission, and follow-ups at the university hospital.
Request for active support from academic colleagues
To gain full support from academic colleagues, in 2001, the authors published the nation's first article on VCA entitled, ‘Concept and current trends of composite tissue allotransplantation’ in the Journal of the Korean Society of Reconstructive Hand Surgery15 and made over twenty presentations and lectures on the topic at multiple university hospitals throughout Korea. At the time, however the Korean Society for Transplantation was not keenly interested in VCA and it was not until 2014 that the Society finally invited the first author to lecture on VCA at the annual congressional meeting's special frontier session. This meeting was very beneficial in that it offered an in-depth preview of VCA to all organ transplantation coordinators nationwide. In November 2015, the author presented on “How to overcome legal problems related to the first hand transplantation in Korea” at the 6th Korea Healthcare Congress in Seoul organized by the Korean Health Association.
Improving public perception and awareness
A city-funded TV public campaign was initiated to attenuate the negative perception of hand/arm donation and to create a favorable public opinion towards hand transplantation. The online website (http://www.arm-transplantation.com) provided necessary information on hand transplantation, successful cases in other countries, and registered donations and recipients. Several public hearings on hand transplantation and briefing sessions for patients and their families were held at Daegu City Hall and YUMC.
The hand transplantation operation
Before the set operation day, W Hospital and YUMC transplantation team had three full practice runs. The surgical team of ten board-certified hand specialists of W Hospital performed the nation's first hand transplantation in Korea on February 2, 2017, with support from the departments of plastic surgery, anesthesiology, psychiatry, pathology, and the organ transplantation center of YUMC.
We transplanted the left distal forearm from a managed brain-dead 48-year-old man to a 35-year-old left-handed man who had suffered a traumatic amputation of the distal radioulnar joint 18 months prior (Fig. 2A and B). Under general anesthesia, the skin of the stump of the recipient's left wrist was incised in a crisscross pattern on the stump. All the flexor and extensor tendons, nerves, and vascular structures were freed for joining with those of the donor hand. All anatomic structures were dissected, identified, and tagged with pre-naming rubbers (Fig. 3A). In the next operation room, the left upper arm of the donor was disarticulated at the elbow under tourniquet control before the procurement of internal organs. It took only 15 minutes. After removing excess skin and bone, all arteries, nerves, and tendons to be repaired were identified (Fig. 3B). The transplantation procedure was almost the same as replantation for the amputation of the forearm. The total operation time was 10 hours 10 minutes.
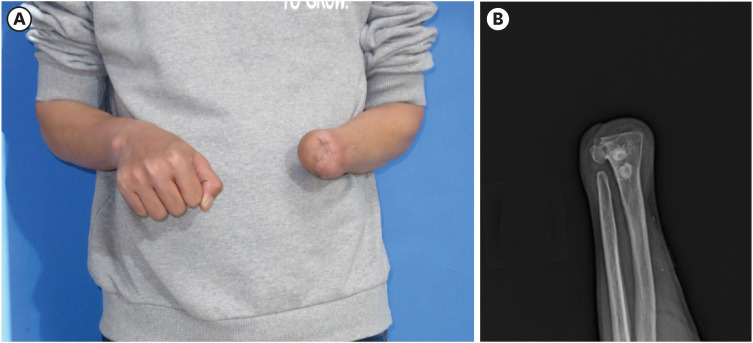 | Fig. 2Recipient of the hand transplantation. (A) A preoperative view of the recipient with a traumatic amputation of the left hand, which took place 18 months prior. (B) The preoperative radiograph shows amputation at the distal radiocarpal joint. The figures are published under agreement of the patient.
|

Ethics statement
The present study was reviewed and approved by the Institutional Review Board (IRB) of Yeungnam University College of Medicine (approval No. 20019-02-042). Informed consent was submitted by the patient when he was enrolled.
Go to :
RESULTS
Legal/legislative results
Application for VCA as the ‘New Health Technology’ was finally approved by the MOHW. This declaration of approval to perform the operation, however, did not resolve the VCA illegality issue because the KOTA had not yet changed at the legislative level to include arm/hand as a possible procurable organ. Even with this approval and favorable support from the government offices, no further legislative actions were forthcoming, and many years of inactivity ensued. On April 21, 2017, two months after the operation, this issue was formally taken up by National Committee for Regulation Reformation under the auspices of the Prime Minister's Office. In conjunction with the National Bioethics Committee, the MOWH arbitrated and gave its full support for VCA operation and declared the “hand and arm” as legal composite tissue appropriate for organ transplantation. This final recommendation continued up to the Presidential Cabinet meeting, which finally endorsed the amendment to KOTA. On May 1, 2018, the legislative amendment bill was sent down for congressional debate and was eventually revised to include the hand/arm.16 Implementation began in August 2018 and hand/arm transplantation is now treated as any other organ transplantation in Korea.
Medical expenses and health insurance coverage
Total medical expenses by the end of October 2018 after the operation were estimated at around USD 91,964, assuming an operation cost of approximately $26,000. This included two readmissions for acute rejection management and monthly outpatient clinic costs and rehabilitation for the 20 months following initial discharge. Routine blood tests and maintenance immunosuppressive medication amounted to $1,206 a month. As per the MOU signed by the city of Daegu, W Hospital, and YUMC, all costs related to this VCA operation were shared by the parties involved. Daegu city provided seed money of $70,000 for the first operation. This covered preoperative examination, promotional expenses including a TV campaign and newspaper articles, an international symposium for VCA, and the opening of an online website.
Immediately after the operation, the W Hospital team, in close collaboration with the Korean Society for Surgery of the Hand (KSSH), the Korean Society for Microsurgery, the Korean Society of Plastic and Reconstructive Surgeons, and the Korean Orthopedic Association, strongly advocated for health insurance coverage by the Health Insurance Review and Assessment Service (HIRA) to reduce the out-of-pocket expense for the patient. The KSSH submitted a request for resource-based relative value scale (RBRVS) for arm transplant surgery. After more than one and a half years of negotiations and controversies, HIRA finally approved national insurance for hand transplantation. It declared the total surgical fee as $9,505 (based on 2020 scale). This figure represents only the surgical fee, which consists of $1,200 for arm/hand procurement, and $8,305 for the transplantation itself. The patient's own out-of-pocket expense is 20% of the total cost, which comes out to around $1,900. Preoperative evaluation, anesthesia fee, and other inpatient fees, outpatient costs, immunosuppression medication, and rehabilitation fees are all billed separately. With the insurance coverage, the patient's cost for monthly maintenance of immunosuppressive medication decreased to $117.
Functional outcomes
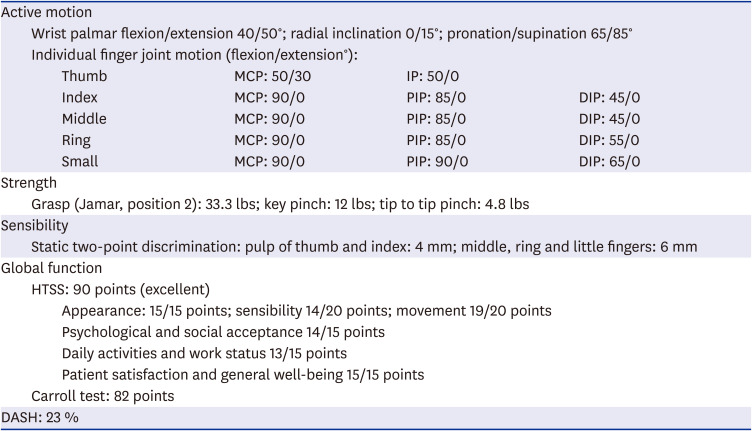
The initial postoperative course was uneventful, and no surgical complications were observed. There were two episodes of acute rejection and an atypical rejection, which were completely resolved with steroid pulse therapy, rituximab, and plasmapheresis. The appearance of the transplanted hand was well-matched with the contralateral one in size and color (Fig. 4A and B). Psychologically, postoperative post-traumatic stress disorder score17 is 7, 46 before the operation (below 20 is normal). The depression score of Beck Depression Inventory18 has improved 13 points from 43, which means mild depression. Postoperative radiography confirmed solid bone union of both radius and ulna by three months (Fig. 5). High-resolution ultrasonography shows patency of the both ulnar and anterior interosseous artery without any intraluminal narrowing (Fig. 6). Functional brain magnetic resonance imaging (MRI, 1.5-T Philips Gyroscan Intera scanner; Philips, Eindhoven, Netherlands) results showed improved effectiveness of the right corticospinal tract by disappearing additional cortical activations on the left primary sensorimotor cortex (Fig. 7). Functional outcome at 36 months after operation showed satisfactory motor and sensory function (Table 1).
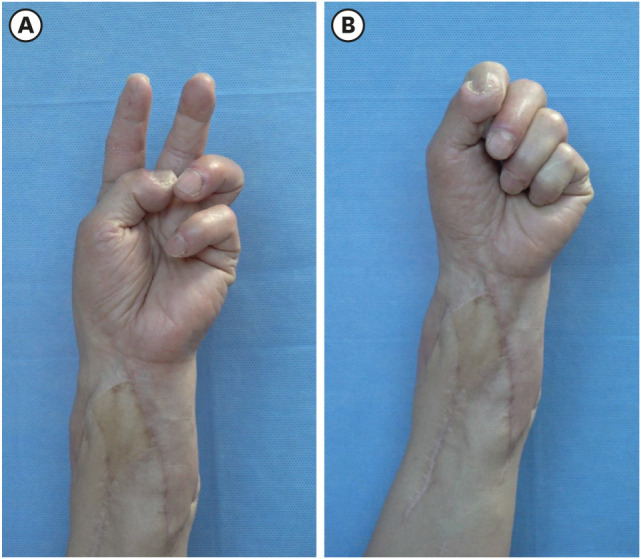 | Fig. 4Postoperative view at 36-months post-transplantation. (A) V-sign of the hand shows independent digital motion of flexion and extension. (B) Grasping of the hand.
|
 | Fig. 5The postoperative radiograph shows good alignment with the complete union of the radius and ulna.
|
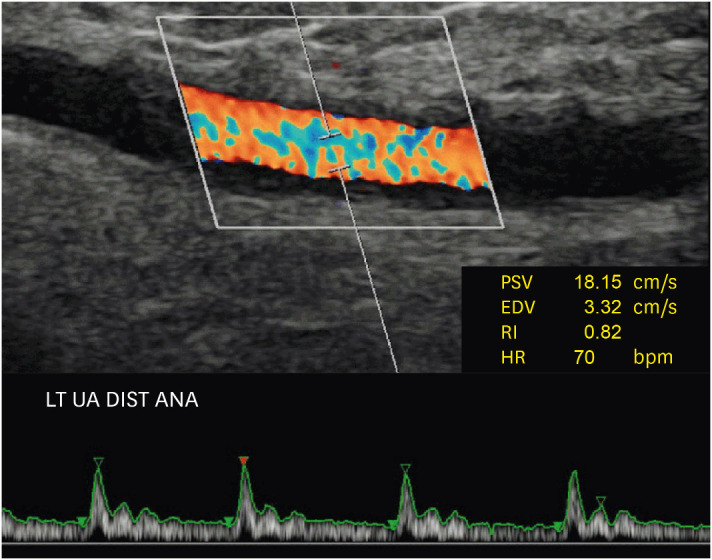 | Fig. 6High-resolution Doppler scan of repaired ulnar artery (Samsung RS 85 unit; Medison Healthcare, Seoul, Korea). There are no signs of intimal thickening or arterial narrowing. The RI of the ulnar artery is 0.82.PSV = peak systolic velocity, EDV = end-diastolic velocity, RI = resistance index, HR = heart rate, LT = left, UA = ulnar artery, DIST = distal, ANA = anastomosis.
|
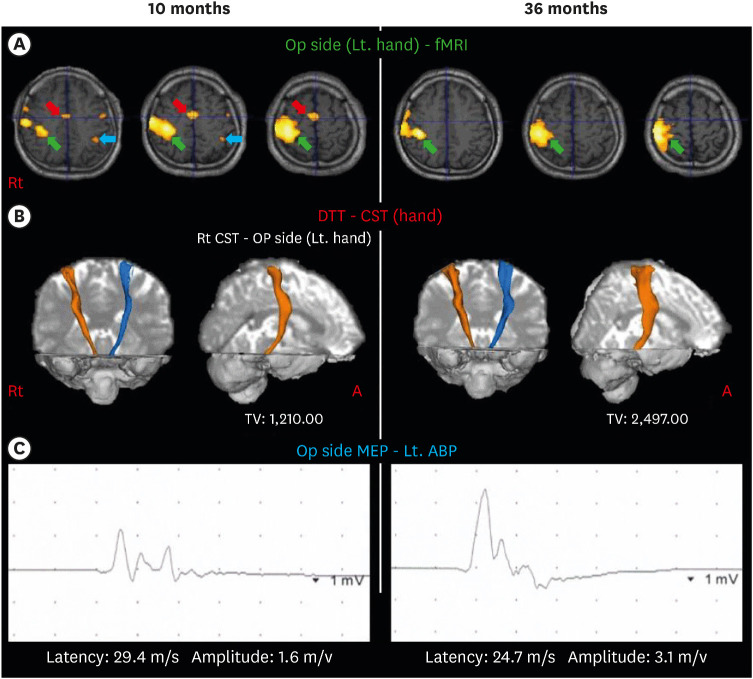 | Fig. 7Postoperative neurologic assessment with functional brain MRI and electromyography. (A) The right primary sensorimotor cortices (green arrow) are activated during the left hand movements on 10- and 36-month functional brain MRI results. Activations of the right primary sensorimotor cortex (sky-blue arrow) and the supplementary motor area (red arrow) on 10-month fMRI have disappeared at 36 months. (B) On 10- and 36-month DTTs, the integrities of the CSTs are well-preserved in both hemispheres. The tract volume of the right CST has increased to 2,497 on 36-month DTT compared with 1,210 at 10-month. (C) On 36-month transcranial magnetic stimulation results, the latency of motor-evoked potential decreased from 29.4 m/s to 24.7 m/s, and the amplitude increased from 1.6 mV to 3.1 mV compared with 10-month.Op = operation, Lt = left, fMRI = functional magnetic resonance imaging, DTT = diffusion tensor tractography, Rt = right, CST = corticospinal tract, A = anterior, TV = tract volume, ABP = abductor pollicis brevis muscle, MEP = motor-evoked potentials, MRI = magnetic resonance imaging.
|
Table 1
Objective assessment of functional outcomes after hand transplantation at a 36-month follow-up
MCP = metacarpophalangeal, IP = interphalangeal, PIP = proximal interphalangeal, DIP = distal interphalangeal, lbs = pounds, HTSS = Hand Transplant Score System, DASH = disabilities of the arm, shoulder and hand.
![]()
Go to :
DISCUSSION
Hand or arm transplantation is not a life-saving procedure and therefore does not warrant the cost or consequences of life-long immunosuppression, which can include increased infections, malignancies, renal failure, diabetes, and death.19 Because of severe complications of immunosuppression, an ethical debate has accompanied its evolution.20 However, the patient survival rate for 107 cases in 72 patients of unilateral or bilateral hand transplantation in isolation is 98.5% since 1999. The long-term graft survival rate is 83.1% per patient or 88.3% per limb.21 The majority of transplant recipients did show progressive improvement upon physical examination and objective functional tests over time. Based on these results, for carefully selected individuals, hand transplantation may be considered standard treatment and alternative to traditional prosthetics despite the risk to recipients with immunosuppression and ethical criticism.22 The loss of body image has a disastrous psychological effect on many amputees,2324 which is underestimated by most of surgeons.
Legal barriers to hand transplantation have long been the most burdensome issue for the authors to deal with in Korea. Several government officers have informally said, “Law follows reality. Conduct a successful VCA operation, and the law will change accordingly.” A case in point happened in October 2011 when a 6-year-old girl with life-threatening intractable chronic intestinal pseudo-obstruction underwent multi-visceral transplantation in Korea.25 Dramatically, the patient survived after transplantation of all seven internal organs, including the liver, pancreas, small intestine, stomach, duodenum, large intestine, and spleen. At the time of surgery, the last four organs were not legally approved for transplantation by the MOHW. Two months later, much inflamed public opinion and demands and protests from the Korean Medical Association resulted in the historical amendment of the Enforcement Ordinance of the KOTA. With continued successes in other multi-visceral transplantations that resulted in changes in the KOTA, W Hospital transplant team mustered up the courage to attempt the Nation's first hand VCA surgery, despite the unresolved legal issue that left all involved surgeons/physicians vulnerable to subsequent legal litigations mostly if the outcome of the attempted surgery was anything but excellent. Even though ten hand and microsurgery specialists with ten to twenty or more years of replantation experience performed the surgery, taking on the operative risks and possible repercussions of a legal breach was quite burdensome. For this precise reason, we should have performed successful hand transplantation in unilateral distal forearm amputation. The authors recognize that some groups, based on ethical debates about the justification for arm transplantation, adopt an agreement authorizing transplant exclusively for bilateral traumatic mid or distal forearm amputation with stumps in good condition in a motivated patient devoid of psychological problems.2226272829
Under the revised KOTA, it permits transplantation of the hands, arms, feet, and legs as a composite tissue composed of bones, skin, muscles, nerves, and blood vessels, irrespective of amputation level or bilaterality. But it still does not include the face, larynx, uterus, penis, and abdominal walls. In the United States, VCA transplantations were performed under the IRB of each institute until 2014. The Organ Procurement and Transplant Network (OPTN) in the United States officially designated VCA as organs in 2014.30 The OPTN has allocated and collected data on VCA transplants separately from all other organs, which are managed in the OPTN computer system. In Taiwanese transplantation law, it already had hands/arms and legs as official organs for transplantation in 2003; they already performed three cases of hand and arm transplantation in 2014 and 2017. On the contrary, in Japan, it does not allow hand/arms transplantation legally. Active experimental research on composite tissue transplantation in the early 2000s is no longer underway. In Korea, regarding face or larynx transplantation for desperate demands by the patients, a few universities have held subsequent experiments and academic meetings.313233343536 However, despite years of efforts due to the safety concerns and ethical problems of the operation, no progress has been made since the medical institution has yet to receive the approval of new health technology, which is the minimal legal step to protect doctors and medical institutions. Continued interest and close cooperation among related transplantation societies, the MOHW, and the Regulatory Reform Committee under the Prime Minister's Office should precede. There must be a change in the public's perception of organ donation of covered human organs for composite tissue allotransplantation. With legal problems unresolved, the new surgery will not go so far as to risk the legal responsibility of individual doctors and the severe damage of the institute, which ones belong in violation of the current law.
Successful procurement of the donated upper extremity was a huge barrier. Twice we failed to procure the arm because of a last-minute withdrawal of consent by the donor's family. Both times the recipient and all surgeons from W Hospital were on standby at the university hospital with a customized prosthesis prepared to be fitted at the donor site. These last-minute reversals of consent show well the profound prejudice regarding the donation of visible organs in Korea. Because organ donation is considered post-mortem mutilation, it is perceived as a great disrespect to the reverend patriarchs deeply rooted in Oriental Confucian society. According to the international registry of organ donation and transplantation, the distribution of deceased donors and living donors demonstrates a significantly different trend between Korea and the United States. In Korea, living organ donors (82.6%) greatly exceed deceased ones (17.4%). In contrast, in the United States, deceased donors (62.4%) exceed living organ donors (37.6%) in 2012.37 This implies that in Korea, donors are likely to give organs to their family members and relatives when they are alive, but not willing to donate organs to others after death. The donation of organs to family members reflects traditional values in which family relationships are considered to be more critical than social ties.
Regarding the 'covered human organ' donation for VCA,38 a public survey for VCA in the United States shows surprisingly favorable attitudes. Most respondents were willing to donate hands/forearms (67.4%) and legs (66.8%), and almost half (48.0%) were willing to donate the face.39 The annual number of people donating organs after death is about seventy thousand in Korea,40 and regretfully, this decreases yearly. Although we have no official data or statistical research on donations for VCA in Korea, it can seemingly never be accepted by the Korean people. Greater VCA public education campaigns need to be developed and implemented.
In November 2018, the MOHW officially announced it would begin covering hand transplants with Korean National Health Insurance. Irrespective of the amputation level of the forearm and upper arm, the operation fee is the same. In bilateral transplantation, the operation fee is twice. Compared with other internal organ transplantations, however, the operation fee for hand transplantation ($9,505) was lower than requested, lower than heart transplantation ($16,332), and single lung transplantation ($12,962), but higher than kidney transplantation ($4,047). Although they have calculated somewhat based on RBRVS, the assigned number of RBRVS seems to be politically influenced and reflects the opinions of the vital organ transplantation committees and groups.
In our case, the left upper arm of the donor was disarticulated at the elbow under tourniquet control before the procurement of internal organs. It took only 15 minutes. Hand and forearm should be harvested before solid organs to prevent impaired hand perfusion and prolong ischemia time.2241 This approach is of limited influence on solid organ procurement as the surgical procedure, in general, takes less than 30 minutes.42 It is typically done under tourniquet, which stays on the donor arm until the procurement. Before the operation, good coordination with the thoracic organ or abdominal team is mandatory. To shorten the operation time and increase the efficiency of the operation, at least two to three experienced hand specialists need to join in two teams, each in the recipient and donor site. And, the chief surgeon, who oversees it, needs to control the entire surgical process.
According to the 2017 survey conducted by the Korea Institute for Health and Social Affairs, the number of patients amputated above the elbow was 9,050 and 11,636 above the wrist.43 Unlike recipients for internal organ transplantation threatened with life; amputation patients do not actively put their names on the waiting list due to concerns over the side effects of immunosuppressant and functional outcomes and the burden of initial examination expenses. Resolved legal and financial obstacles will now grant many amputee patients the hope of overcoming their disability.
In conclusion, the nation's first hand VCA transplantation was successfully carried out with intermediate follow up showing excellent functional and quality of life status, paving the way for activation of the VCA program in Korea. VCA is no longer illegal in Korea and is fully covered by Korean National Health Insurance. The authors hope that the nation's first case of VCA will serve as the starting point for more comprehensive clinical applications of VCA in Korea. Additional educational and public awareness programs are necessary for the general public and potential donors. The surgical academic community also needs to become more familiar with VCA. The authors hope that this experience in Korea will offer some guidance to physicians in other countries facing similar legislative and social issues.
Go to :
 XML Download
XML Download