

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Urinary tract infection (UTI) is typically one of the most common human infections.12 When patients with UTIs visit the hospital through an outpatient clinic or emergency room, only blood or urine cultures can be used to identify bacterial pathogens. However, these cultures require several days to verify the results. The most common UTI bacterial pathogen is Escherichia coli.
3 In most clinical situations, empirical antibiotics to treat E. coli for patients with UTIs are prescribed even before cultures verify the results. Trimethoprim-sulfamethoxazole, previously used empirically for UTI, is currently not recommended because of its high resistance rates.4 Similarly, ciprofloxacin is also not recommended for simple UTIs since the rate of resistance in the United States is reported to be 32.4%.5
The detection rate of upper urinary tract stones is rapidly increasing due to recent advances in technology such as computed tomography, and an increase in health awareness among people leading to regular medical check-ups.6 Obstruction, due to urinary stones, inhibits the normal flow of urine and the resulting stasis compromises the bladder and renal defense mechanisms. Stasis also contributes to the growth of bacteria in the urinary tract and their ability to adhere to urothelial cells.7 Furthermore, UTI accompanied by urinary obstruction is detrimental as it can lead to sepsis.8 However, in order to begin empirical antibiotic therapy before the culture test results, clinicians need to know the regional distribution of the pathogens that cause UTIs and the resistance of those microorganisms to antibiotics. This is especially important when urinary stones are found in febrile patients with UTIs, although no research has been performed to confirm this. The aim of this series was to characterize the local antimicrobial resistance pattern in febrile patients with urinary stones and guide recommendations regarding empiric antibiotic regimens based on these data.
Go to : 
METHODS
Patients and setting
This study was conducted at three institutions in the Republic of Korea. We retrospectively collected medical data of febrile patients between January 2011 and December 2016 who visited outpatient departments or emergency rooms for antibiotic treatment of UTIs with upper urinary tract calculi. Among these patients, those whose medical information identified the following were excluded: urine culture results unidentifiable, another cause of UTI (elevated prostate-specific antigens, ureteral stent indwelling state, a severe neurogenic bladder, history of urologic neoplasm, or anatomical abnormality of the urologic system) identified, and the impact of fever found in other organs (e.g., pneumonia, tonsillitis, cellulitis). We investigated demographic characteristics, underlying diseases, stone-related factors, and results of urine and blood culture examinations and antibiotic sensitivity tests. This study was approved by the institutional review board of each hospital.
Definitions
A febrile condition was defined as the presence of fever (body temperature ≥ 38.0°C).9 UTIs were defined as the presence of ≥ 5 leukocytes per high-power field from a centrifuged specimen. Chronic kidney disease was defined as creatinine clearance < 60 mL/min/1.73 m2.10 A recurrent UTI was defined as three or more UTIs in the preceding 12 months, or two or more UTIs in the preceding 6 months.11 Prior antibiotic treatment was defined as antibiotic usage during the preceding 90 days. A healthcare-associated UTI was defined according to the modified criteria of Friedman et al.,12 as follows: 1) the patient received intravenous therapy, wound care, or specialized nursing care at home during the 30 days prior to the UTI; 2) the patient attended a hemodialysis clinic or received intravenous chemotherapy within 30 days before the infection; 3) the patient had been hospitalized for acute care for 2 or more days in an acute-care hospital in the 90 days preceding the infection; 4) the patient resided in a nursing home or long-term care facility; or 5) the patient received an invasive urinary procedure, urological surgery, or urethral catheterization within the 30 days prior to the UTI.12 For determining quinolone resistance, if either ciprofloxacin or levofloxacin had microorganism resistance, it was considered resistant. To simplify the classification according to the location of stones, the kidney and upper ureter stones were classified as proximal and the mid and lower ureter as distal.
Antibiotic susceptibility testing
Antibiotic susceptibility testing was performed using either the semi-automated VITEK II system (bioMérieux, Hazelwood, MO, USA) or the MicroScan (Dade Behring, West Sacramento, CA, USA) system at each hospital. The antimicrobial susceptibility of pathogens was based on the standards of the Clinical and Laboratory Standards Institute. Isolates showing intermediate antimicrobial susceptibility were considered to be resistant.
Statistical analysis
Statistical analysis was performed using SPSS version 20 (SPSS Inc., Chicago, IL, USA), and all reported P values were two-sided, with P < 0.05 considered statistically significant. Student's t-test was applied to assess the differences in continuous variables among groups. Categorical data were analyzed using χ2 or Fisher's exact tests, as appropriate. Any variable with a P value < 0.05 in the univariate analysis was included in the binary logistic regression as a dependent variable.
Ethics statement
This study's protocol was approved by each Institutional Review Board (IRB) on human research: Dongguk University Ilsan Hospital, Dongguk University College of Medicine (2018-10-028); Ilsanpaik hospital, Inje University College of Medicine (2018-08-001). No informed consent was needed because it was a retrospective study.
Go to :
RESULTS
Table 1 shows the patients' demographic characteristics. The mean age of patients was 61.97 years (standard deviation [SD], 20.38). One hundred and forty-one (69.5%) were female and 62 (30.5%) were male. The mean height of patients was 158.62 cm (SD, 10.34), and the mean weight of patients was 59.09 kg (SD, 12.74). The underlying diseases in the patients were cardiovascular disease (n = 106, 52.2%), diabetes mellitus (n = 72, 35.5%), neurological disease (n = 59, 29.1%), chronic kidney disease (n = 7, 3.4%), solid tumors (n = 15, 7.4%), hematological disease (n = 2, 1.0%), chronic liver disease (n = 8, 3.9%), chronic pulmonary disease (n = 16, 7.9%), and connective tissue disease (n = 3, 1.5%). Patient history included bed-ridden state (n = 46, 22.7%), prior antibiotic treatments within 3 months (n = 60, 29.6%), healthcare-associated UTIs (n = 37, 18.2%), and recurrent UTIs (n = 47, 23.2%). The mean size of the upper urinary tract stones was 12.68 mm (SD, 11.41). One hundred and twenty patients (59.1%) had proximal ureter stones, and 83 patients (40.9%) had distal ureter stones. Single urinary stones occurred in 160 patients (78.8%), and multiple urinary stones occurred in 43 patients (21.2%). Hydronephrosis was found in 176 (86.7%) patients. Of the 120 patients with a proximal ureter stone, 93 (77.5%) had hydronephrosis. All 83 patients with distal ureter stones were identified with hydronephrosis on the ipsilateral side.
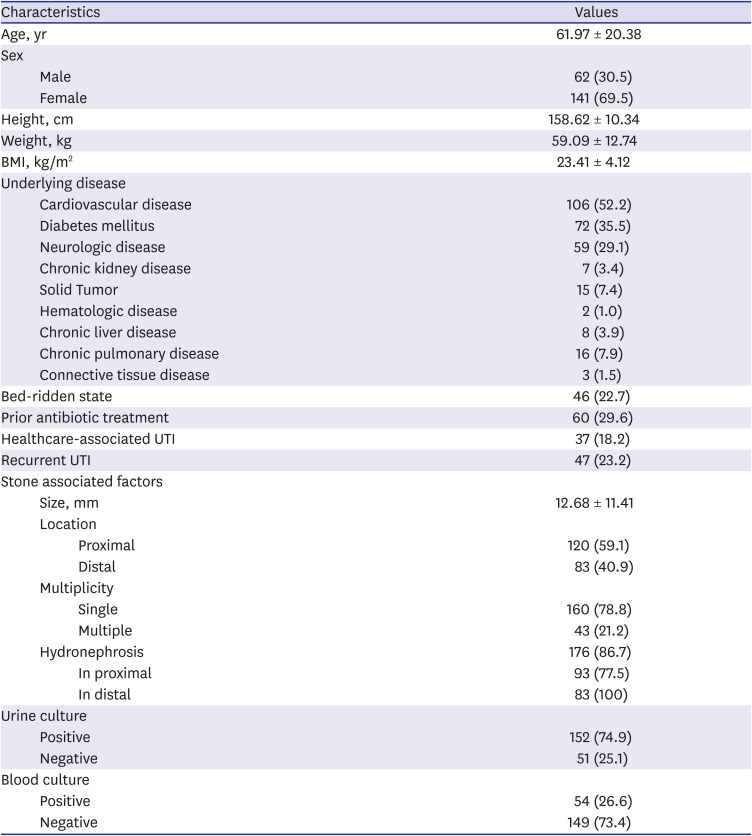
Table 1
Patients' demographic characteristics
Values are presented as mean ± standard deviation or number (%).
BMI = body mass index, UTI = urinary tract infection.
![]()
Bacteria were identified in 152 of the 203 patients (74.9%). The bacterial pathogens are described in Table 2. The most commonly cultured bacteria included E. coli (44.1%), followed by Enterococci spp. (11.8%), Proteus spp. (8.6%), Streptococcus agalactiae (6.6%), Klebsiella spp. (5.3%), Pseudomonas spp. (4.6%), coagulase-negative Staphylococcus (4.0%), Staphylococcus epidermidis (4.0%), Serratia spp. (2.6%), Acinetobacter spp. (0.7%), Enterobacter spp. (0.7%), and mixed infections (7.2%). Cultured bacterial species showed sex-specific differences. The differences in cultures, according to sex, are shown in Fig. 1. In males, the most commonly cultured bacteria were Enterococci spp. (19.5%), followed by E. coli (14.6%), Pseudomonas spp. (14.6%), S. agalactiae (12.2%), Proteus (9.8%), coagulase-negative Staphylococcus (7.3%), S. epidermidis (7.3%), Klebsiella spp. (4.9%), Serratia spp. (2.4%), Acinetobacter (2.4%), and mixed infections (4.9%).
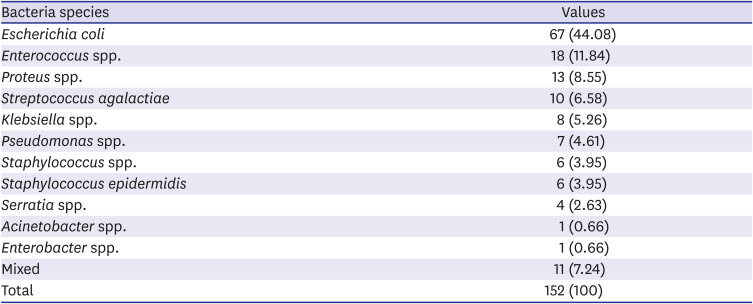
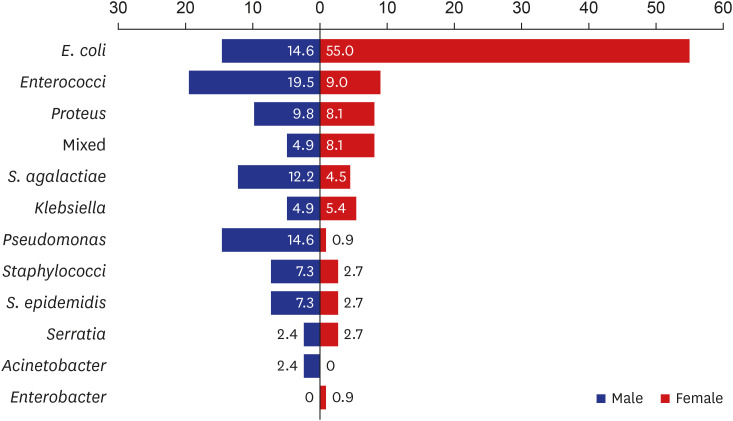
Table 2
Kinds of bacteria and resistance rate in urine culture
![]()
Cardiovascular disease, diabetes mellitus, neurological disease, a bed-ridden state, prior antibiotic treatment within 3 months, healthcare-associated UTIs, and multiple urinary stones were found to be risk factors for quinolone resistance in univariate analysis (P = 0.034, P = 0.009, P = 0.031, P = 0.018, P = 0.021, P = 0.003, P = 0.002, and P = 0.005, respectively). Multivariate analysis revealed that the multiplicity of calculi was an independent predictive factor for quinolone resistance (P = 0.008).
Advanced age, neurological disease, chronic pulmonary disease, healthcare-associated UTIs, recurrent UTIs, and multiple urinary stones were risk factors for cefotaxime resistance in univariate analysis (P = 0.018, P = 0.024, P = 0.008, P = 0.020, P = 0.005, and P = 0.025, respectively). Recurrent infection was a significant predictor of cefotaxime resistance in multivariable analysis (P = 0.041). Table 3 summarizes the factors associated with the resistance to common antibiotics.
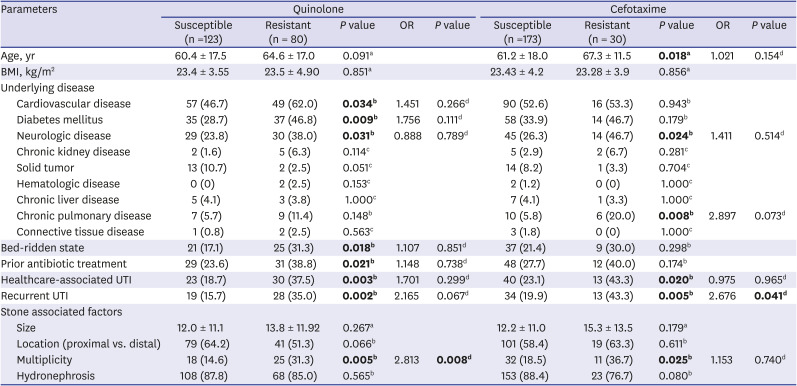
Table 3
Analysis of febrile patients with UTIs regarding ciprofloxacin and cefotaxime resistance (n = 203)
Values are presented as mean ± standard deviation or number (%). P values below 0.05 are shown in bold.
OR = odds ratio, BMI = body mass index, UTI = urinary tract infection.
aUsing Student's t-test; bUsing χ2 test; cUsing Fisher's exact test; dUsing binary logistic regression test.
![]()
Among patients, 19.6% were infected with extended-spectrum beta-lactamase (ESBL)-producing bacteria. Advanced age was a factor associated with an ESBL-positive result in the single variant analysis (P = 0.029); however, it was not a significant factor in multivariate analysis. Table 4 summarizes the factors associated with ESBL-positive patients.
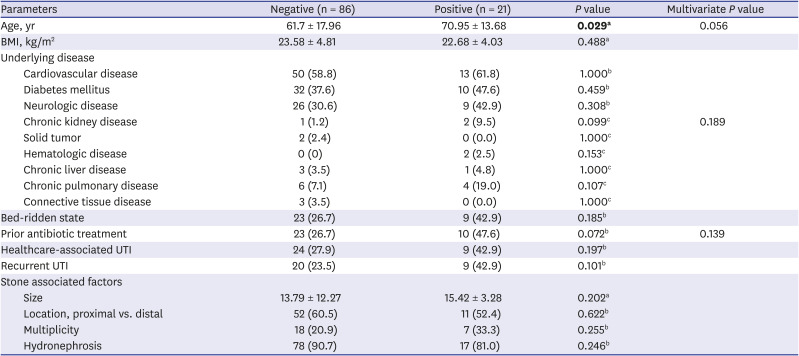
Table 4
Analysis of febrile patients with ESBL and UTIs
Values are presented as mean ± standard deviation or number (%). P values below 0.05 are shown in bold.
ESBL = extended-spectrum beta-lactamase, BMI = body mass index, UTI = urinary tract infection.
aUsing Student's t-test; bUsing χ2 test; cUsing Fisher's exact test; dUsing binary logistic regression test.
![]()
Go to :
DISCUSSION
Clinicians routinely examine febrile UTI patients in emergency rooms or clinics, and many of these patients also have upper urinary tract calculi. This series aimed to characterize the local antimicrobial resistance patterns in febrile patients with upper urinary stones and make recommendations regarding empiric antibiotic regimens. Our purpose was not to classify these patients using different types of UTIs.
Nevertheless, febrile patients with upper urinary tract calculi in this study had some unique epidemiological characteristics different from those with UTIs without calculi. The incidence of urinary tract calculi was affected by numerous factors. In population-based studies, the diagnosis of urinary tract stones increased faster in female than in male,13 although in Asia, the prevalence was still slightly greater in male than in female.14 According to Tae et al.,15 the incidence of urinary tract calculi was similar in Korea. However, there were approximately twice as many females in this study. These incidence differences between male and female were also observed in a study conducted in Japan by Hamasuna et al.,16 who reported that the male to female ratio was 1:2.2 for patients with obstructive pyelonephritis and urolithiasis. Considering reports that approximately more than half of the female experience UTIs during their lifetime, this difference may be acceptable.2
Another characteristic was the type of bacteria isolated. Traditionally, E. coli is the most common causative UTI strain,317 and accounts for 75% to 90% of the non-complex cystitis and nephritis-causing bacteria in female.9 This percentage was reported to be lower in complicated UTIs. In a study on the clinical features of complicated pyelonephritis, Buonaiuto et al.,18 reported that E. coli was cultured in 67% of patients. However, in a study of investigating obstructive uropathy with urinary tract calculi, Hamasuna et al.16 reported that E. coli represented 48.9% of the bacteria cultured. Marien et al.8 reported that E. coli represented 66% of the bacteria cultured. In our study, E. coli was only cultured 44.1% of the time. Differences in sex can explain this decrease in E. coli cultured from the urine in complicated UTIs with obstructive uropathy. While female patients in our study had a very high rate of cultured E. coli, similar to other studies, this was not true for males where E. coli was only cultured 14.6% of the time. Notably, the ratio of Proteus spp. (9.8%) and Pseudomonas spp. (14.6%) in male patients was higher than those in females (8.1% and 0.9%, respectively). These species can create alkaline urine, which can result in the formation of calcium phosphate stones.19 These results suggest that even with similar symptoms and clinical situations, the differences may be sex-related. Our study found it difficult to determine whether calculi were the cause of the infection or the result of the infection, but the existence of urinary tract calculi was an effect of the type of bacteria in febrile patients with UTIs. This difference is also very important since the initial treatment using empirical antibiotics is determined by the most prevalent bacteria cultured from patients with UTIs. Additional studies investigating sex differences are imperative.
Since very few studies have investigated the antibiotic resistance of bacteria in patients with UTIs and urinary stones, an accurate comparison between this study and others is challenging. The resistance rate to quinolone was found to be very high, at 39.41% in this study. A previous study showed that in complicated UTIs, the quinolone resistance ratio was higher than in non-complicated UTIs.20 Another study involving healthcare-related UTIs showed that improper use of antibiotics increased the resistance to quinolones. However, in this study, a bed-ridden state, prior antibiotic treatment, and healthcare-associated UTIs were significant factors in the single variable analyses, but not in the multivariate analyses.21 According to guidelines from the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases, if local resistance prevalence exceeds 20%, it is recommended not to be used in empirical treatment.22 Since it was known that quinolone resistance was high and there was an increase in quinolone-resistant bacteria, the use of quinolone as a primary antibiotic in simple UTIs was not recommended in Korea.4 The cephalosporin family of antibiotics is often used as primary antibiotics to replace quinolone. Even in the three institutions involved in the study, the most common antibiotic used as an initial treatment for febrile UTI patients was the cephalosporin family. In this study, the resistance rate of cefotaxime was 14.78%, with multivariate analysis indicating that the risk factor for this resistance was recurrent UTIs. These findings are in accordance with those reported in previous UTI studies.2324 At the study planning stage, recurrent UTI was also expected to be a cause of ESBL-producing bacteria. However, old age alone was significant in the single-variable analyses, and there was no significant factor identified in the multivariate analyses for ESBL-producing bacteria. If primary antibiotic resistance is suspected, a combination of aminoglycosides may be considered.2526 However, complicated UTIs are often accompanied by decreased renal function; thus, attention should be paid to the side effects of nephrotoxicity. In recent studies, β-lactam/β-lactamase inhibitors have reported non-inferior results in UTI by multidrug-resistant bacteria compared to carbapenem; therefore, β-lactam/β-lactamase inhibitor is one of the empiric treatment options for complicated UTI.2728 Considering the distribution of bacterial strains, a similar effect can be expected in patients with febrile UTI and upper urinary tract calculi.
The present study had a few limitations. First, this retrospective study could not assess certain types of information such as whether antibiotics were used, the types of antibiotics, or antibiotic resistance. Furthermore, if there was a lack of information regarding other causes of UTIs in the medical records, patients with other causes of UTIs besides urinary stones may have been included in the results of this study. Second, all patients did not undergo surgery; therefore, the relationship between infection and urinary tract calculi was unclear as the components of the calculi were not identified. In addition, it was difficult to verify the postoperative urine culture test to determine the relationship between the causative bacterial species and urinary tract calculi. Third, most urine samples were collected through natural urination in emergency rooms or outpatient visits. If the catheter was inserted due to voiding symptoms, the culture results were collected after implantation. Therefore, the possibility of sample contamination cannot be ruled out. Further, it was not possible to verify the uniformity of the culture test, as a central test was not conducted. Finally, patients with secondary visits from other hospitals may have had false-negative results in urine culture as a result of previous treatment with antibiotics. This may have affected the resistance rate outcome.
In conclusion, based on the results of this study, cultured bacterial species showed sex-specific differences. If multiple urinary stones were identified in febrile patients with UTIs, quinolone was not recommended as an empirical antibiotic treatment. Although combination antibiotic therapy is recommended for patients with recurrent UTIs, cefotaxime resistance can occur. In older, febrile patients with UTIs and urinary tract calculi, multi-drug resistant bacteria should be considered when choosing antibiotics for the initial treatment.
Go to :
 XML Download
XML Download