

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since being originally devised by Noon1 in 1900, the efficacy of allergen immunotherapy (AIT) has been clearly demonstrated, particularly for the treatment of respiratory allergy, allergic rhinitis, and asthma.2 In randomized controlled studies, AIT has proven effective in controlling symptoms and reducing the requirement for medication, as well as in preventing progression to new allergen sensitization and development of asthma.34 More recent observational studies have also confirmed the effectiveness of AIT,56 causing it to emerge as a potent and specialized strategy employed by allergists to treat respiratory allergic diseases.
Yet, physicians and patients face several obstacles in AIT treatment. Although it is a safe and efficacious tool, its treatment adherence is reportedly low. In fact, some studies have reported the proportion of patients completing three years of treatment, to be as low as 30%.7 The inconvenience associated with frequent hospital visits during the initial build-up phase required for conventional immunotherapy (CIT) is one of the factors that deters patients from initiating AIT. Recently intralymphatic immunotherapy, requiring markedly fewer injections, was introduced in an effort to reduce the associated inconvenience to patients.8 Thus, physicians must address the key factors responsible for the low adherence to optimize an immunotherapy strategy befitting the patients' need.910
Rush immunotherapy (RIT), involving a rapid increase in concentration and allergen extract doses, was introduced to reduce frequent hospital visits and the required duration for the build-up phase.11 However, RIT is associated with a higher risk of adverse events compared to CIT as a result of rapidly intensifying treatment protocol.12 Considering this safety concern, aqueous allergen extracts have not been routinely adopted into RIT, as the rapid absorption of allergen could lead to an increased risk of systemic reaction. However, the characteristics and clinical applications of aqueous allergen extracts differ from those of modified allergen extracts, making them more suitable for use in AIT for polysensitized patients. Nonetheless, since the safety concerns associated with AIT have not been adequately addressed, particularly in comparison to that of RIT with modified allergens, and CIT with aqueous allergens, this study aimed to investigate the safety and utility of RIT with aqueous allergen extracts.
Go to : 
METHODS
Study population
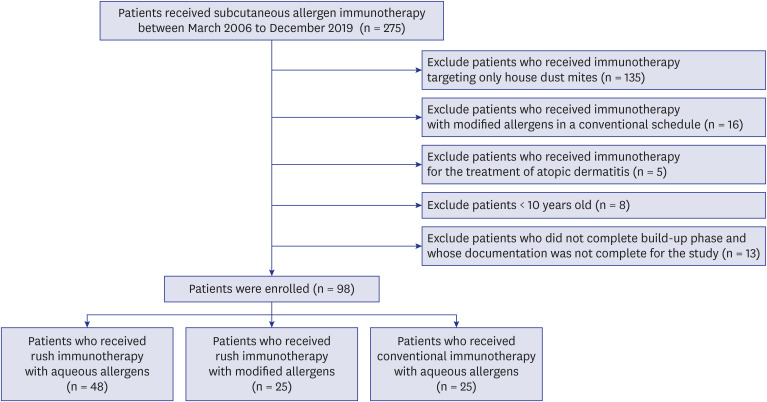
A medical chart review was conducted to retrospectively collect patient data at a single tertiary center, Wonju Severance Christian Hospital in Korea. Subcutaneous immunotherapy was administered to study subjects between March 2006 and December 2019 for the treatment of respiratory allergies, allergic rhinitis with or without bronchial asthma. Degree of asthma control before initiating AIT was classified into well controlled, partly controlled, and uncontrolled according to the GINA guidelines.13 Their atopic status was determined through skin prick test and serum specific immunoglobulin E (IgE) testing using the immunoCAP system (ThermoFisher Scientific, Uppsala, Sweden). A wheal size ≥ 3 mm or specific IgE ≥ 0.35 kU/L caused by the allergen was indicative of a positive result. Among positive allergens, the type of allergen extracts mixed for use in AIT was ultimately selected by the physician, considering allergen cross-reactivity and clinical relevance. Among the patients who received subcutaneous immunotherapy during the study period, those who received immunotherapy with modified allergens as per the conventional schedule, those who received immunotherapy for the treatment of atopic dermatitis, those younger than 10 years old, and those who did not complete the build-up phase or whose documentation in the medical chart was incomplete, were excluded (Fig. 1). In addition, patients who received AIT targeting only house dust mites (HDMs) were excluded, given the AIT pattern for clinical practice. While AIT for only HDM is often prescribed with modified allergen extracts, AIT for allergens other than HDM, or for multiple allergens, has been administered with modified or aqueous extracts.
AIT
The commercially available allergen products used in this study were aluminum hydroxide adsorbed Novo-Helisen® depot extract (Allergopharma, Reinbeck, Germany) and Hollister-Stier® (Jubilant HollisterStier, Spokane, WA, USA) aqueous extract. Both products comprised four bottles of different strength. Novo-Helisen® depot extract consisted of strength 1, strength 2, strength 3, and strength 4; while Hollister-Stier® aqueous extract was diluted at concentrations of 1:1,000, 1:100, 1:10, and 1:1 (undiluted). Depot extract was formulated according to manufacturer instructions at the physician's request. Meanwhile, aqueous extract was diluted by the physician in the clinical setting, in accordance with manufacturer instructions taking into account the recommended effective dose.11 Study subjects were classified into three groups according to the type of commercial allergen products and immunotherapy schedules: those receiving RIT with aluminum hydroxide adsorbed Novo-Helisen® depot extract (depot-RIT); RIT with Hollister-Stier® aqueous extract (aqueous-RIT); and CIT with Hollister-Stier® aqueous extract (aqueous-CIT). Depot-RIT was prescribed between March 2006 and December 2014, while aqueous-RIT and aqueous-CIT were not administered to the patients in our hospital until January 2015.
Mixed allergen extracts were administered with gradually increasing concentrations and doses during the initial build-up phase. The same dose and concentration of allergen was injected every four weeks during the subsequent maintenance phase. AIT schedules were classified based on the initial build-up phase through either CIT or RIT. Mixed allergens were injected subcutaneously once per week during the build-up phase in CIT. In contrast, during RIT, patients were hospitalized for 4 to 5 days and were injected at shorter intervals with rapidly increasing concentrations and doses of allergen extracts. In aqueous-RIT, 0.1 mL, 0.3 mL, and 0.6 mL of aqueous extract containing 1:1,000, 1:100, and 1:10 diluted allergens, respectively were administered at 2-hour intervals. The undiluted (1:1) solution was administered at a starting dose of 0.05 mL, followed by increments of 0.05 mL or 0.10 mL at each step. After discharge, the patients visited the hospital every 1 or 2 weeks until the maintenance dose was reached (Table 1). In depot-RIT, the four extract dilutions were administered in 0.1 mL, 0.2 mL, 0.4 mL, and 0.8 mL doses at 2-hour intervals. The maximum maintenance dose was 0.3 mL for aqueous extract and 1 mL for depot extract. Leukotriene receptor antagonist and second-generation antihistamine were prescribed to all patients before immunotherapy as a pretreatment, as well as during the build-up phase, regardless of the immunotherapy schedule. If a systemic reaction was observed, chlorpheniramine and dexamethasone were administered, after which the subsequent scheduled injection was delayed until the systemic symptoms abated. In the event of severe systemic reaction, including anaphylaxis, RIT was discontinued and subsequent build-up phase injections were restarted with an equal or lowered dose at the outpatient department (OPD). During the maintenance phase, 1:1 undiluted solution was administered, and the dose for which was determined considering the sensitivity of the patient and their systemic reaction during the build-up phase. Patients sensitized to seasonal allergens were initiated with AIT excluding allergens for the corresponding season.
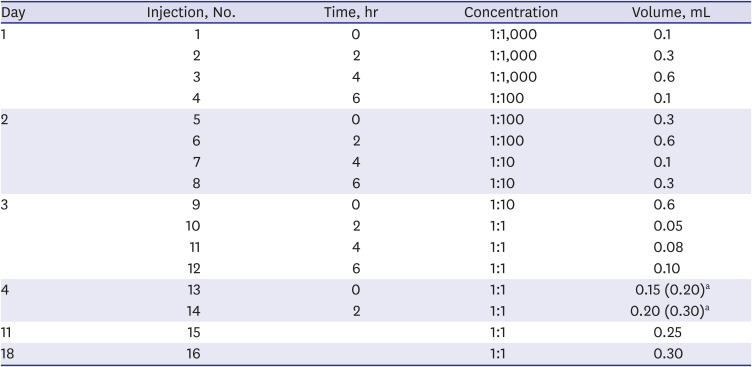
Table 1
Protocol for rush immunotherapy with aqueous allergen extracts
aIf patients were well tolerable without systemic reaction, 0.20 mL and 0.30 mL were administered instead of 0.15 mL and 0.20 mL.
![]()
Study outcomes
Safety was assessed using a previously described grading system.14 Grade 1 was defined as localized reaction at injection site; grade 2 as a cutaneous reaction such as urticaria at locations other than the injection site; grade 3 as generalized pruritus, urticarial, angioedema, rhinitis, itchy throat, or cough; grade 4 as occurrence of wheezing, shortness of breath, or lung function decline in peak expiratory flow or pulmonary function test; grade 5 as laryngeal edema or severe asthma not responding to an inhaled bronchodilator, or anaphylaxis including hypotension or loss of consciousness, abdominal cramping, or diarrhea; and grade 6 as cardiopulmonary arrest. Systemic reaction was adjudged based on subjective symptoms reported by patients as well as physical or objective examination performed by physicians at each visit. Localized reactions restricted to injection sites (grade 1) were not recorded. Reaction of grade 2 or greater was regarded as a systemic reaction. Severe systemic reaction was defined as grade 5 or greater during the build-up phase.
During the skin prick test, the longest wheal diameter and its perpendicular diameter were measured and recorded. Cumulative wheal size obtained for the test was a summation of the longest wheal diameter caused by all allergens included as AIT allergen extracts.
Utility was analyzed based on the reduced number of visits to the OPD, as well as the time interval required to achieve maintenance phase with RIT compared to CIT. All data regarding safety and utility variables were limited to the build-up phase.
Statistical analysis
Baseline clinical characteristics for the study subjects were described as the mean value ± standard deviation for continuous variables and as the number of patients plus percentage they occupied within each group for categorical variables. Continuous variables among three groups were compared using the Kruskal–Wallis test, and Mann Whitney U test was used to compare the data between two groups as the data were not normally distributed and the n value was too low to allow for parametric analysis. χ2 test was used for the comparison of categorical variables. Binary logistic regression was used to identify variables associated with systemic reaction. All statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). A P value < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board of Wonju Severance Christian Hospital (CR320061). Informed consent was waived due to the retrospective nature of the study.
Go to :
RESULTS
Demographics of the study subjects
A total of 98 patients (25 in depot-RIT, 48 in aqueous-RIT, and 25 in aqueous-CIT) were enrolled in the study. The completion rate of the protocol was 100% (25/25) in depot-RIT, 96% (48/50) in aqueous-RIT, and 92.6% (25/27) in aqueous-CIT. The mean patient age was 27.2 ± 13.4 years (11–52 years) in depot-RIT, 26.0 ± 14.1 years (range: 10–66 years) in aqueous-RIT, and 32.2 ± 15.3 years (10–63 years) in aqueous-CIT (P = 0.231). More than half of the patients had both allergic rhinitis and bronchial asthma: 64.0% in depot-RIT, 64.6% in aqueous-RIT, and 76.0% in aqueous-CIT (P = 0.564). All but 2 patients had well or partly controlled asthma before initiating AIT. Proportion of polysensitization was defined as sensitization to two or more types of allergen families (HDMs, tree pollens, grass pollens, weed pollens, or animal dander) and was 88.0% in depot-RIT, 93.8% in aqueous-RIT, and 84.0% in aqueous-CIT (P = 0.402). The most frequently sensitized allergens were HDMs and tree pollens, while the allergen sensitized to the fewest patients was grass pollen. Sensitization to cat and dog dander was 16.0% in depot-RIT, which was significantly less than the 60.4% of aqueous-RIT and 60.0% of aqueous-CIT (P = 0.001). Total duration of immunotherapy, including the build-up phase and maintenance phase, was 47.3 ± 23.0 months in depot-RIT, 25.1 ± 13.2 months in aqueous-RIT, and 24.2 ± 16.9 months in aqueous-CIT (P < 0.001), with the depot-RIT treatment duration being significantly longer than that associated with aqueous-RIT (P < 0.001). Meanwhile, differences were not observed between aqueous-RIT and aqueous-CIT (P = 0.650). The mean maintenance dose after build-up phase was 0.98 ± 0.07 mL in depot-RIT, 0.25 ± 0.07 mL in aqueous-RIT, and 0.26 ± 0.08 mL in aqueous-CIT. No difference was observed in the maintenance dose between aqueous-RIT and aqueous-CIT (P = 0.819). Patient characteristics are shown in more detail in Table 2.
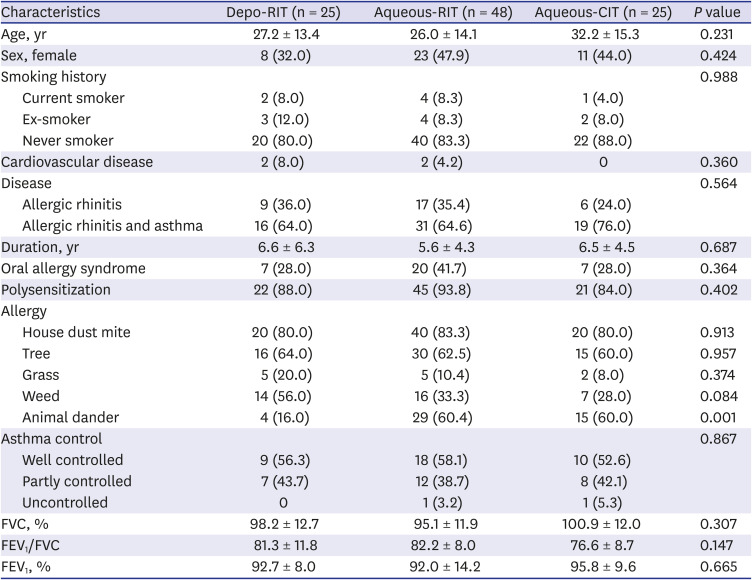
Table 2
Baseline patient characteristics
Values are presented as mean ± standard deviation or number (%).
RIT = rush immunotherapy, CIT = conventional immunotherapy, FVC = forced vital capacity, FEV1 = forced expiratory volume in the first second.
![]()
Combined allergen components for immunotherapy
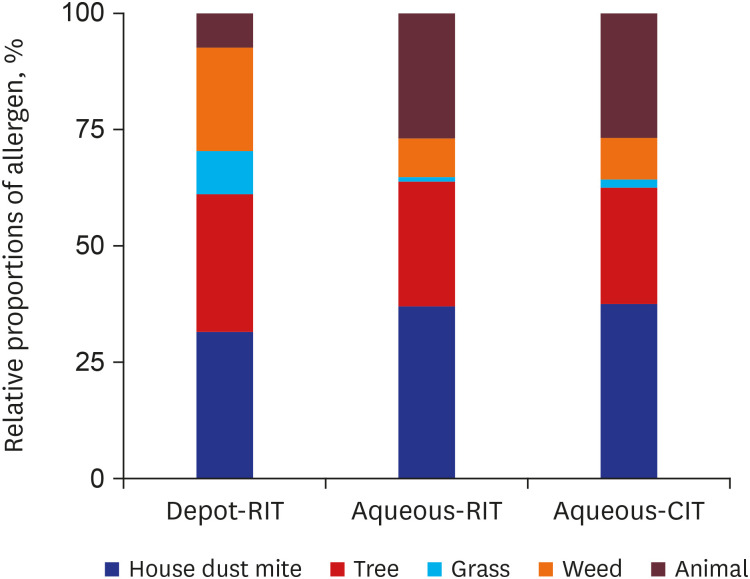
The mean numbers of allergens mixed in AIT was 3.1 ± 1.1 in depot-RIT, 3.7 ± 1.0 in aqueous-RIT, and 3.5 ± 1.2 in aqueous-CIT (P = 0.089). The most frequently mixed allergens were HDMs and tree pollens, similar to that observed for sensitization patterns: 68.0% and 64.0%, respectively in depot-RIT, 83.3% and 58.3%, respectively, in aqueous-RIT, and 80.0% and 56.0%, respectively, in aqueous-CIT. Grass and weed pollen were administered more in depot-RIT than in aqueous-RIT and aqueous-CIT: 20.0%, 2.1%, and 4.0%, respectively, P = 0.015 (grass); 48.0%, 18.8% and 20.0%, respectively, P = 0.019 (weed). However, animal dander was included in 16.0% of depot-RIT mixtures, which was significantly lower than that in aqueous-RIT (60.4%) and aqueous-CIT (56.0%; P = 0.001). The relative proportions of allergen components combined in the different immunotherapies are depicted in Fig. 2.
The cumulative wheal size observed during the skin prick tests was 35.7 ± 20.2 mm in depot-RIT, 26.6 ± 19.0 mm in aqueous-RIT, and 22.8 ± 16.7 mm in aqueous-CIT (P = 0.016). Total IgE levels were 542.1 ± 549.3 kU/L in depot-RIT, 806.1 ± 1,035.2 kU/L in aqueous-RIT, and 475.4 ± 412.2 kU/L in aqueous-CIT (P = 0.763). Specific IgE levels to Dermatophagoides farinae were 49.5 ± 40.7 kU/L in depot-RIT, 42.0 ± 35.3 kU/L in aqueous-RIT, and 34.2 ± 31.2 kU/L in aqueous-CIT (P = 0.730). Specific IgE to birch were 40.0 ± 41.7 kU/L in depot-RIT, 39.9 ± 39.0 kU/L in aqueous-RIT, and 28.2 ± 33.0 kU/L in aqueous-CIT (P = 0.746). Specific IgE levels to other allergens included in the three groups were comparable (Table 3).
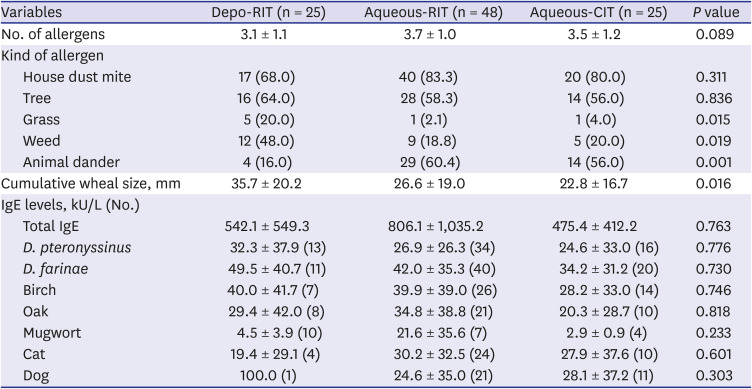
Table 3
Types of mixed allergens and their specific IgE levels in each immunotherapy group
Values are presented as mean ± standard deviation or number (%).
RIT = rush immunotherapy, CIT = conventional immunotherapy, IgE = immunoglobulin E.
![]()
Safety of RIT
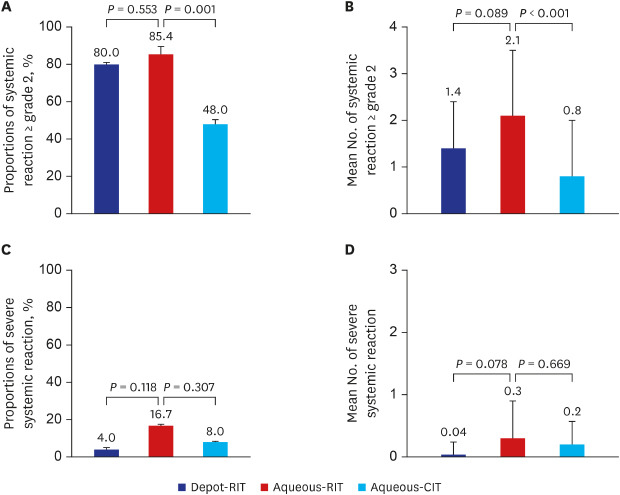
The proportion of patients who had a grade 2 or higher systemic reaction was 20/25 (80.0%) in depot-RIT, 41/48 (85.4%) in aqueous-RIT, and 12/25 (48.0%) in aqueous-CIT (P = 0.002) (Fig. 3A). Moreover, the mean number of grade 2 or higher systemic reaction occurring per patient were 1.4 ± 1.0 in depot-RIT, 2.1 ± 1.6 in aqueous-RIT, and 0.8 ± 1.2 in aqueous-CIT (P < 0.001) (Fig. 3B). Within two group analysis, systemic reaction was more frequent in aqueous-RIT than in aqueous-CIT (proportion of patients with systemic reaction of grade 2 or higher: P = 0.001; mean number of systemic reactions of grade 2 or higher per patient: P < 0.001). Meanwhile, no significance was observed between depot-RIT and aqueous-RIT (proportion of patient with systemic reaction of grade 2 or higher: P = 0.553; mean number of systemic reactions of grade 2 or higher per patient: P = 0.089).
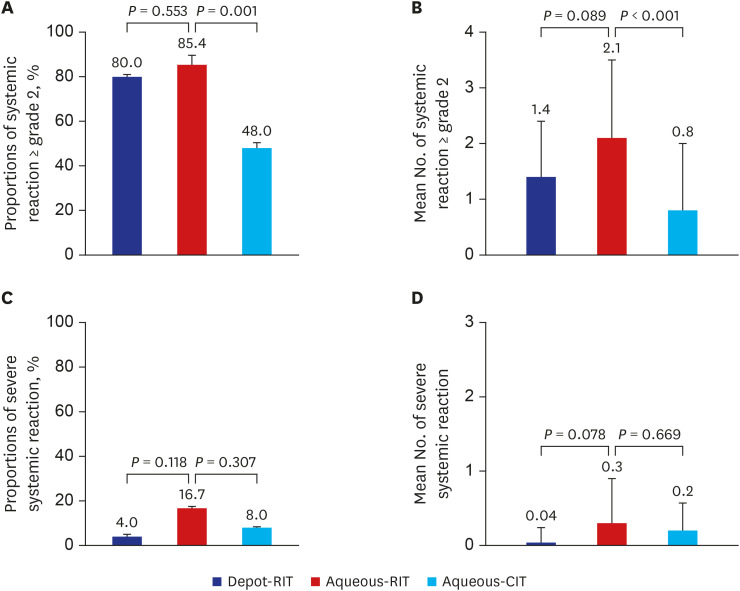 | Fig. 3Safety of immunotherapy. Proportion of patients experiencing systemic reaction of grade 2 or greater (A) and mean number of systemic reaction of grade 2 or higher per patient (B). Proportion of patients experiencing severe systemic reaction (C) and mean number of severe systemic reaction per patient (D).RIT = rush immunotherapy, CIT = conventional immunotherapy.
|
The proportion of patients who had severe systemic reaction was 1/25 (4.0%) in depot-RIT, 8/48 (16.7%) in aqueous-RIT, and 2/25 (8.0%) in aqueous-CIT (P = 0.223) (Fig. 3C). Mean number of severe systemic reaction occurring per patient was 0.04 ± 0.2 in depot-RIT, 0.3 ± 0.6 in aqueous-RIT, and 0.2 ± 0.4 in aqueous-CIT (P = 0.208) (Fig. 3D). Within two group analysis, severe systemic reaction was not statistically different between aqueous-RIT and aqueous-CIT (the proportion of patient with severe systemic reaction: P = 0.307; mean number of severe systemic reactions per patient: P = 0.669) or between depot-RIT and aqueous-RIT (proportion of patient with severe systemic reaction: P = 0.118; mean number of severe systemic reactions per patient: P = 0.078). All severe systemic reactions were anaphylaxis, while grade 6 was not observed in any of the groups.
In aqueous-RIT, 23/41 (56.1%) patients experienced their first systemic reaction of grade 2 or greater with 1:10 diluted allergen, while 14/41 (34.1%) experienced their first systemic reaction with 1:1 undiluted allergen. However, in aqueous-CIT, 3/12 (25.0%) patients experienced their first systemic reaction of grade 2 or greater with 1:10 diluted allergen, while 8/12 (66.7%) had it with 1:1 undiluted allergen. In aqueous-RIT, all but four patients tolerated 1:1 undiluted allergen during hospitalization, although subsequently, all patients reached 1:1 undiluted allergen before maintenance phase.
In aqueous-RIT, patients experiencing systemic reaction of grade 2 or greater had a larger cumulative wheal size compared to those without systemic reaction; however, these results were not statistically significant (28.2 ± 19.8 mm vs. 17.4 ± 10.0 mm, P = 0.533). Univariate analysis revealed that no significant variable was associated with systemic reaction of grade 2 or greater (Table 4).
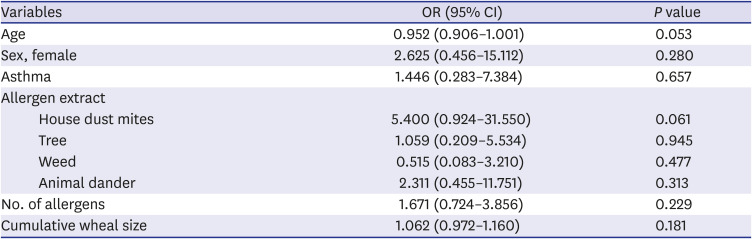
Table 4
Univariate analysis of risk factors for systemic reaction during rush immunotherapy with aqueous allergens
![]()
Utility of RIT
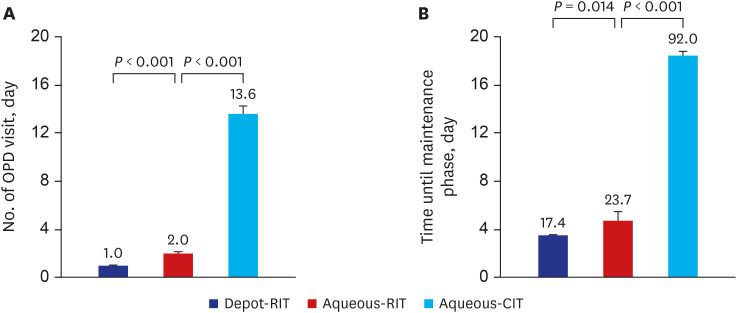
The mean number of injections during the build-up phase was 17.0 ± 0.2 in depot-RIT, 14.0 ± 1.1 in aqueous-RIT, and 14.2 ± 1.3 in aqueous-CIT (P < 0.001). Number of injections in aqueous-RIT was lower compared to those in depot-RIT (P < 0.001). Number of OPD visits during the build-up phase were 1.0 ± 0.2 in depot-RIT, 2.0 ± 1.3 in aqueous-RIT, and 13.6 ± 1.9 in aqueous-CIT (P < 0.001). Fewer OPD visits were recorded for aqueous-RIT compared to aqueous-CIT (P < 0.001) and more compared to depot-RIT (P < 0.001) (Fig. 4A). Interval times until maintenance phase were 17.4 ± 1.8 days in depot-RIT, 23.7 ± 10.9 days in aqueous-RIT, and 92.0 ± 12.5 days in aqueous-CIT (P < 0.001). Interval times in aqueous-RIT were shorter compared to aqueous-CIT (P < 0.001) and longer compared to depot-RIT (P = 0.014) (Fig. 4B). Hospitalization days were 4.4 ± 0.8 days in depot-RIT and 4.2 ± 0.6 in aqueous-RIT (P = 0.177).
Go to :
DISCUSSION
Herein, we sought to compare the outcomes of aqueous allergen-RIT with those of aqueous allergen-CIT and depot-RIT to ascertain the clinical value of aqueous allergen-RIT. As there were no significant differences in rates of systemic reactions, aqueous-RIT was found to have an acceptable safety profile compared to that of depot-RIT. In addition, utility of aqueous allergen-RIT was revealed through reduced frequency of OPD visits and shortened duration for build-up phase in comparison to aqueous allergen-CIT. To our knowledge, this is the first study to report data from four-day RIT protocols with aqueous allergen in patients with polysensitization.
Novo-Helisen® depot is an aluminum-precipitated extract, representing a modified allergen.15 Allergoids account for another type of altered allergen, which are produced by a reaction between allergenic proteins and formaldehyde, or glutaraldehyde, to develop high molecular weight complexes.16 These allergen modifications are expected to reduce allergenicity and rate of absorption at injection site, resulting in decreased systemic reactions. On the other hand, Hollister-Stier® represents aqueous extracts without allergen modification. Extracts that are soluble in water, and thus inclined to rapid absorption at injection sites, have inherent safety concerns, particularly in RIT applications. However, this study showed that multiple allergens in aqueous extracts can be used in RIT without increasing the occurrence of systemic reactions. Hence, useful application of aqueous allergen extracts is expected in RIT, particularly in polysensitized patients.
Significant differences exist in the clinical application of immunotherapy between Europe and the United States.17 For instance, in Europe, allergen extracts are generally prepared and customized by the manufacturer for individual patients. Nearly, all patients are treated with only one clinically relevant modified allergen, such as depot extracts. In contrast, in the United States, allergen extracts are prepared in clinical setting and multiple allergens are generally mixed with the mean number of allergens applied for AIT reported to be eight. Meanwhile, modified allergens are rarely used in the United States. In Korea, three types of allergen products are primarily prescribed. Aluminum hydroxide adsorbed Novo-Helisen® depot and L-tyrosine adsorbed Tyrosine S® (Allergy Therapeutics, Worthing, UK) are representative of European style, while Hollister-Stier® aqueous extracts resemble the American style.18 When treating polysensitized patients, it remains unclear whether multiple allergens, or only one relevant allergen, is most efficacious.19 Nevertheless, a recent study in Korea showed that the mean number of sensitized allergens was 4.5 ± 2.2, and 60.8% of subjects were sensitized to more than three allergens.20 Hence, if multiple allergens are necessary in polysensitized patients, aqueous allergen extracts of the American style would be a suitable treatment option. In addition, the present study showed that this strategy can reduce the amount of time spent by the patient at the hospital by adopting RIT protocol.
Although, RIT is more convenient than CIT, it has a higher probability of inducing a systemic reaction, an observation which is consistent with the present study. In a previous study, the systemic reaction rate in those without premedication was 15% to 100%, and was 3% to 79% in those administered premedication.11 Moreover, a study by Sharkey and Portnoy14 reported a systemic reaction rate of 5/22 (23%), in which the last injection was 1:100 diluted allergen, using a rush protocol. The study by Harvey et al.21 reported 25/65 (38%) patients having a systemic reaction during a 1-day protocol of aqueous allergen-RIT, in which the last dose was 0.05 mL of 1:1 undiluted allergen. Further, 72% of systemic reactions developed with 1:1 undiluted allergen and 28% with 1:10 diluted allergen. In addition, cumulative wheal score in the skin prick test correlated with the systemic reaction. In our study, the occurrence of a systemic reaction of any grade was 85.4% in aqueous-RIT; 56% of which occurred with 1:10 diluted allergen and 34% with 1:1 undiluted allergen. Moreover, cumulative wheal size was not predictive of systemic reaction. The differences observed between the two studies in the rate of systemic reaction and concentration of allergen extracts triggering the systemic reaction might be attributed to differences in the RIT protocols. In our study, prednisone was not included as premedication and a maximum dose of 1:1 undiluted allergen was permitted, if tolerated by the patient. Moreover, a correlation between larger skin test reaction and risk of systemic reaction has not been consistently reported. While DaVeiga et al.22 reported a significant association between larger skin test response and elevated risk of systemic reaction, Rank et al.23 did not find a similar association. Given the results in the present study, risk factors for systemic reactions remain to be determined. A follow-up study to identify patients at greater risk during immunotherapy, and to devise an effective preventive strategy against systemic reaction would be beneficial.24
Several limitations were noted in this study. First, the types of allergens mixed differed between the depot-RIT and aqueous-RIT. In addition, as described before, these treatments had different characteristics in terms of allergen modification and practice patterns. Therefore, direct comparison between depot-RIT and aqueous-RIT in real-world practice is challenging. Other limitations include the retrospective design of the study and small number of subjects enrolled. Although a significant difference in the occurrence of severe systemic reactions was not observed between aqueous-RIT and depot-RIT, aqueous-RIT was found to induce more frequent severe systemic reactions compared to depot-RIT. Therefore, we could not definitely conclude whether the safety of aqueous-RIT was superior based solely on the resulting P value, which may have been caused by the small n value for the study. Accurate analysis of the systemic reaction incidence and its associated risk factors in a prospective study with a larger study population is warranted.
In conclusion, RIT with aqueous allergen extracts can be performed in polysensitized patients with respiratory allergies as it improves patient convenience and is accompanied by an acceptable risk of systemic reaction.
Go to :
 XML Download
XML Download