

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) is a rapidly spreading disease with various symptom profiles. The outbreak has created unprecedented threats and difficulties for societies and healthcare systems worldwide.123 The outbreak started in December 2019 in Wuhan, China, where the first cases of pneumonia of unknown origin were reported. Subsequently, the pathogen was identified as a coronavirus and named COVID-19.4 Since then, the virus has spread to most of the world, with cases reported on every continent except Antarctica.5 The World Health Organization (WHO) declared COVID-19 as a pandemic on March 11, 2020.45 COVID-19 has infected 64,603,428 people, resulting in 1,500,614 deaths worldwide as of December 4, 2020.6 Korea recorded its first COVID-19 case on January 20, 2020, and by December 4, 2020, Korea had 36,915 confirmed cases and 540 deaths, with a mortality rate approaching 1.5%.7
The current COVID-19 pandemic is a major challenge to national health systems. COVID-19 has caused significant disruptions to established care paths, including those for acute conditions such as neurosurgical emergencies.8 Little was known about managing neurosurgical diseases during the initial phase of the COVID-19 global crisis. Intensive changes have been necessary for neurosurgical practice.9 The greatest challenge faced by neurosurgeons is emergency surgery on patients with neurosurgical emergencies.
Screening for COVID-19 is crucial, and hastily performed surgery without excluding COVID-19 increases the risk of COVID-19 contamination in the hospital, which exposes patients and doctors to grave danger.10 However, COVID-19 screening is time-consuming, which delays surgery and may result in catastrophic neurological complications. Therefore, maintaining a balance between adequate screening and timely surgery is essential for the management of neurosurgical emergencies. Here, we aimed to propose a clinical pathway for emergency brain surgery during the COVID-19 pandemic and quantify its effect on the clinical outcomes of patients.
METHODS
Subjects
A total of 114 patients were admitted through the emergency room (ER) and underwent a neurosurgical operation between February 1, 2020 and June 30, 2020, and a total of 104 patients were admitted through the ER and underwent a neurosurgical operation in the previous year between February 1, 2019 and June 30, 2019. In the COVID-19 group, 57 patients were excluded (20 patients with a spinal emergency, 31 patients who visited the ER with non-emergency neurosurgical problems and underwent elective surgery after hospitalization, and 6 patients with an exceptionally long hospital stay with non-neurosurgical reasons). Most of the spinal emergency patients were due to acute pain and received elective surgery after admission. Also, outcome measures were not consistent with the brain emergencies so these cases were excluded from the study. Long-term hospitalization cases due to refusal to discharge, due to issues related medical insurance or financial issues were excluded because these cases could have a significant impact on comparing the difference in length of hospital stay before and after COVID-19 in emergency brain surgery patients. In addition, 25 patients who did not undergo a COVID-19 reverse transcription-polymerase chain reaction (RT-PCR) test during the early COVID-19 period were excluded. In the pre-COVID-19 group, 39 patients were excluded (12 patients with spine neurosurgical emergencies, 21 patients with non-emergency neurosurgical problems, and 6 patients with an inappropriate length of stay). Finally, 32 patients in the COVID-19 group and 65 patients in the pre-COVID-19 group were included in the study.
Baseline and outcome assessment
We performed a retrospective review of consecutive patients undergoing emergency neurosurgical operations who were admitted to our hospital in Korea, 5 months after the COVID-19 outbreak. The data were extracted from electronic medical records in an institutional database using a standardized data collection form. The baseline demographics of the patients including age, sex, and brain emergency type were collected. The severity of the presenting state measured by the Korean Triage and Acuity Scale (KTAS), vital signs, Glasgow Coma Scale (GCS) at ER arrival, and initial surgical procedures were recorded, and the time interval from ER arrival to severity classification, time interval from ER arrival to admission, and time interval from ER arrival to skin incision were reviewed. The time of admission was defined as the time the patient started to transfer from the ER to the operating room, intensive care unit (ICU) or ward. Additionally, patient outcomes including the 30-day mortality, complications during hospital stay (neurological [e.g., re-bleeding, brain edema, infarction, hydrocephalus], pulmonary [e.g., pneumonia, pulmonary thromboembolism, atelectasis], and non-pulmonary infectious [e.g., sepsis, urinary tract infection, procedure site infection]), Glasgow Outcome Scale (GOS) after 1 month, modified Rankin Scale (mRS) after 1 month, length of hospital stay, requirement of ICU care, and requirement of mechanical ventilation were recorded from the database. We compared these factors between the COVID-19 group and the pre-COVID-19 group. A subgroup comparison within the COVID-19 group was performed to investigate how characteristics and outcomes differed between the group undergoing immediate surgery and the group undergoing semi-elective surgery. Semi-elective surgery was defined as a surgery that must be performed as soon as possible but is unsuitable to be performed immediately due to an unconfirmed COVID-19 status.
COVID 19 screening and quarantine
According to the COVID-19 guideline and protocol published by the Central Disaster Management Headquarters of Korea Centers for Disease Control & Prevention and the Central Disease Control Headquarters of the Ministry of Health and Welfare, cases are defined based on the patient's epidemiological history and clinical symptoms.7
If a family member or domestic partner living in the same facility had COVID-19 clinical symptoms, if there was contact with a family member, domestic partner, friend, or acquaintance who entered the country from abroad within 14 days, or if there was a history of visiting an institution or place where a confirmed case was detected, this was noted in the epidemiological history, and the patient was recommended for active examination even if there were no clinical symptoms. These patients were defined as Patient Under Investigation (PUI). In addition, those with COVID-19 clinical symptoms such as fever (37.5°C or higher), cough, difficulty in breathing, chills, muscle pain, headache, sore throat, loss of smell and taste, or pneumonia were included for investigation and also defined as PUI.
Those who developed COVID-19 clinical symptoms within 1 day after contact with confirmed patients were classified as suspected cases. Confirmed cases were defined as cases in which infection was confirmed by a positive RT-PCR result regardless of clinical symptoms.
Inpatient wards were divided into the isolation ward and general ward. Isolation wards consisted of single-person isolation rooms and six-person isolation rooms according to the level of protection. The single-person isolation room was primarily for patients with a high suspicion of COVID-19 infection. The six-person isolation room was mainly for patients with a low risk of COVID-19 infection; however, the possibility could not be completely ruled out, and observation was required until a negative RT-PCR result was obtained.
Clinical pathway for emergency brain surgery during the COVID-19 pandemic
Since the start of the COVID-19 outbreak, our hospital designed a standardized clinical pathway to assess COVID-19 pre-operatively, and it was used from February 2020. The neurosurgery department has modified this clinical pathway according to the characteristics of patients who need emergency brain surgery. The detailed clinical pathway is shown in Fig. 1.
Fig. 1
Clinical pathway for emergency brain surgery during the COVID-19 pandemic.
In the case of COVID-19 RT-PCR result (+) in a patient who underwent emergency surgery, the patient was reported to local public health authorities and transferred to a 1-person room in an isolated ward. In the case of COVID-19 RT-PCR result (+) in a patient requiring semi-elective surgery, the patient was reported to local public health authorities. The location of containment and time of neurosurgical treatment were decided according to the severity and risk.
COVID-19 = coronavirus disease 2019, RT-PCR = reverse transcription-polymerase chain reaction, PPE = personal protective equipment, ICU = intensive care unit.
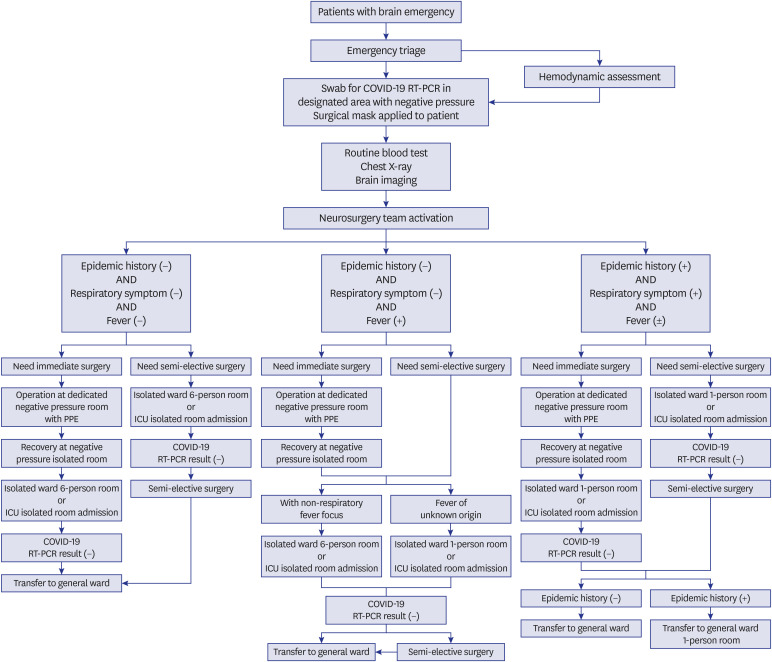
When patients were first presented to the ER with a brain emergency, a brief screening for COVID-19 was performed immediately at the registration office. The patients were triaged according to their epidemiological history and clinical manifestations. If they had unstable vital signs, stabilization was performed as a priority in an isolated negative pressure ER. A surgical mask was immediately worn on the patient as soon as the patient arrived, and if oxygen was to be supplied through a nasal cannula, a surgical mask was worn over the device. Then, a swab for COVID-19 RT-PCR was performed in the quarantine office outside the ER to minimize the risk of droplet spread.
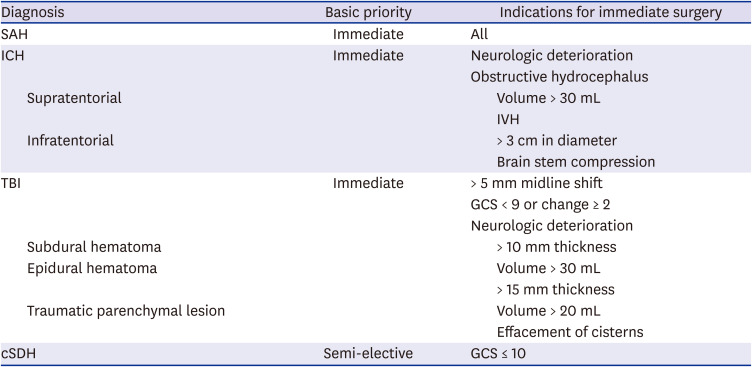
Pre-operative laboratory tests were performed after COVID-19 screening. Routine preoperative tests include blood typing and cross-matching, blood counts, electrolytes, kidney function tests, liver function tests, glucose measures, coagulation tests, cardiac integrity markers, inflammatory markers, viral infectivity screening, urinalysis, pregnancy tests, arterial blood gas analysis, 12-lead electrocardiogram, and chest radiography. Then, brain imaging was performed. As soon as brain imaging results were ready, the neurosurgery team was called and requested for consultation. The neurological emergency was evaluated by neurosurgeons, and the necessity of immediate surgery and feasibility of semi-selective surgery were determined. The decision of emergency brain surgery was individualized according to the patient's neurological condition, the size and location of the bleed, the age, and the health status, but basically, the indications for the immediate surgery were determined based on the criteria presented in Table 1.
Table 1
Indications for immediate surgery in brain emergencies
Immediate surgery was performed without confirmation of the COVID-19 RT-PCR result in the negative pressure operating room. The operation was considered as an aerosol-generating procedure, and all patient interactions were conducted with enhanced droplet precautions and personal protective equipment (PPE).11 The surgical team replaced the surgical mask with an N95 or Korea Filter (KF) 94/99 respirator, wore visors or goggles to protect the eyes and wore a gown, gloves, shoe covers, and a hair cover before draping the patient according to the surgical procedure. For patients who needed immediate surgery with an epidemic history or respiratory symptoms regardless of fever, all personnel in the operating room wore level D PPE (coveralls, safety boots, goggles, double gloves, N95 or KF94/99 respirator) during surgery (Fig. 2).
Fig. 2
Preparation for emergency brain surgery in PUI or suspected cases.
(A) Level D PPE (coveralls, safety boots, goggles, double gloves, N95 or KF94/99 respirator) (B) Preparation of the operating room.
PUI = patients under investigation, PPE = personal protective equipment, KF = Korea filter.

The patient's transfer route was set to the shortest possible distance as a pre-planned route and was moved by the same transport personnel. The operating room was dedicated and was set as close to the entrance of the theater block. The operating room door was set from automatic to manual and closed. It was stated in front of the door that an operation was underway for a patient whose possibility of COVID-19 could not be excluded. The operating room personnel entered the operating room on time to minimize exposure, and the relevant personnel adhered to the principle of not leaving the operating room during the procedure. To minimize the operation time as much as possible, the operation was performed with an experienced neurosurgeon and minimal assistants. During craniotomy and drilling, more rigorous irrigation was performed than usual, so that the aerosol did not disperse, and efforts were made to minimize the anterior skull base procedures that could open the air sinuses. After surgery, the PPE was removed and disposed of in a dedicated doffing area outside the operating room, and the relevant area was disinfected as soon as possible.
Ward admission was conducted using a dedicated elevator, and the patient was hospitalized in an independent ward in another building. After confirming the result of COVID-19 RT-PCR, transfer to a general ward was decided. RT-PCR tests were performed three times a day, and results for COVID-19 could be obtained within 5 hours. Semi-elective surgery was performed after admission to an isolation room and when the COVID-19 RT-PCR result was obtained.
If a patient was confirmed as having COVID-19 RT-PCR result (+) after emergency surgery, the patient was reported to local public health authorities and transferred to a 1-person room in an isolated ward. If a patient requiring semi-elective surgery was confirmed as having COVID-19 RT-PCR result (+), the patient was reported to local public health authorities. The location of containment and time of neurosurgical treatment were decided according to the severity and risk (Fig. 1).
Statistical analysis
IBM SPSS Statistics for Windows (version 23; IBM Corp., Armonk, NY, USA) and GraphPad Prism (version 8; Graph Pad Software Inc., San Diego, CA, USA) were used for all statistical analyses. For categorical variables, data are expressed as frequencies and percentages. The χ2 test or Fisher's exact test was used to analyze categorical variables using contingency tables. For continuous variables, data are expressed as the mean ± standard error. When continuous variables were normally distributed, the mean differences between the groups were analyzed using Student's t-test. For non-normally-distributed variables, Mann-Whitney U test was used. P values < 0.05 were considered statistically significant.
RESULTS
Comparison between the pre-COVID-19 period and COVID-19 period
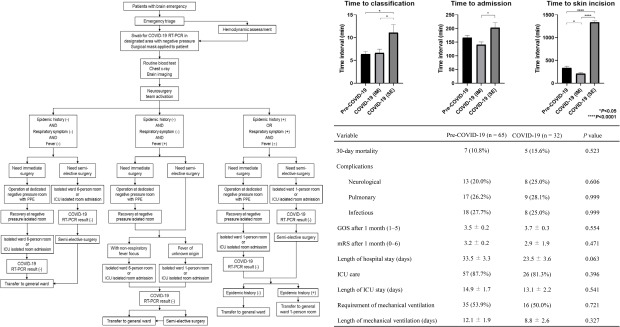
There was a difference in age between the two groups (P = 0.036); however, there were no significant differences in sex and diagnosis. There were no significant differences in the severity indicators and initial surgical procedure. In the comparison of the time intervals of emergency processes, there were no significant differences in the time interval from ER arrival to severity classification and time interval from ER arrival to admission. However, the time interval from ER arrival to skin incision was significantly increased in the COVID-19 group (P = 0.027) (Table 2).
Table 2
Comparison of the baseline characteristics, severity indicators, and time intervals between the pre-COVID-19 group and COVID-19 group
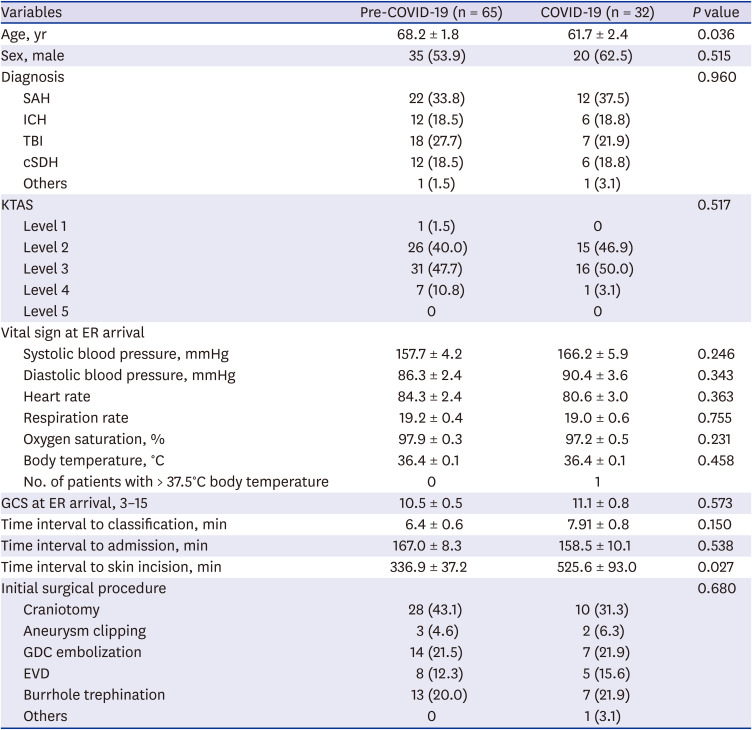
Data are presented as the mean ± standard error or number (%).
COVID-19 = coronavirus disease 2019, SAH = subarachnoid hemorrhage, ICH = intracerebral hemorrhage, TBI = traumatic brain injury, cSDH = chronic subdural hematoma, KTAS = Korean Triage and Acuity Scale, ER = emergency room, GCS = Glasgow Coma Scale, GDC = Guglielmi detachable coil, EVD = external ventricular drainage.
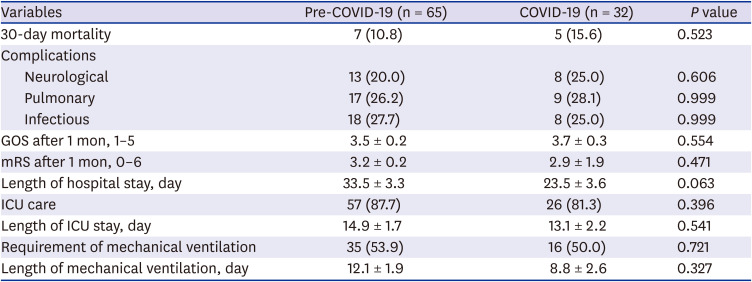
There were no significant differences in the outcomes between the two groups, including the 30-day mortality, complications, GOS after 1 month, mRS after 1 month, length of hospital stay, requirement of ICU care, length of ICU stay, requirement of mechanical ventilation, and length of mechanical ventilation (Table 3).
Table 3
Comparison of the outcomes between the pre-COVID-19 group and COVID-19 group
Comparison between the immediate surgery group and semi-elective surgery group in the COVID-19 period
In the comparison of the severity indicators and time intervals between the two groups, significant differences were observed in all items such as the diagnosis (P = 0.016), time interval from ER arrival to severity classification (P = 0.038), time interval from ER arrival to admission (P = 0.002), and time interval from ER arrival to skin incision (P < 0.001) (Table 4).
Table 4
Comparison of the severity indicators and time intervals between the COVID-19 subgroups
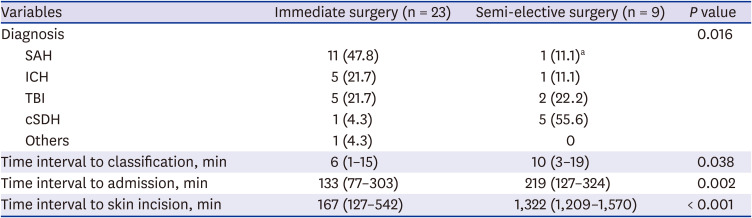
Subgroup data, analyzed with the non-parametric method, are presented as the median (range) or number (%).
COVID-19 = coronavirus disease 2019, SAH = subarachnoid hemorrhage, ICH = intracerebral hemorrhage, TBI = traumatic brain injury, cSDH = chronic subdural hematoma.
aSemi-elective external ventricular drainage was performed for hydrocephalus in a case with subarachnoid hemorrhage of unknown origin.
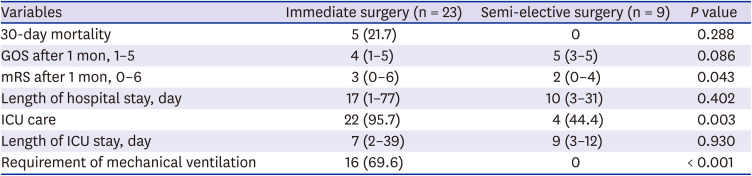
In the comparison of the outcomes, there were no significant differences in the 30-day mortality, GOS after 1 month, length of hospital stay, and length of ICU stay. However, there were significant differences in the mRS after 1 month (P = 0.043), requirement of ICU care (P = 0.003), and requirement of mechanical ventilation (P < 0.001) (Table 5).
Table 5
Comparison of the outcomes between the COVID-19 subgroups
Comparison of the time intervals of emergency processes among the pre-COVID-19 group and COVID-19 subgroups
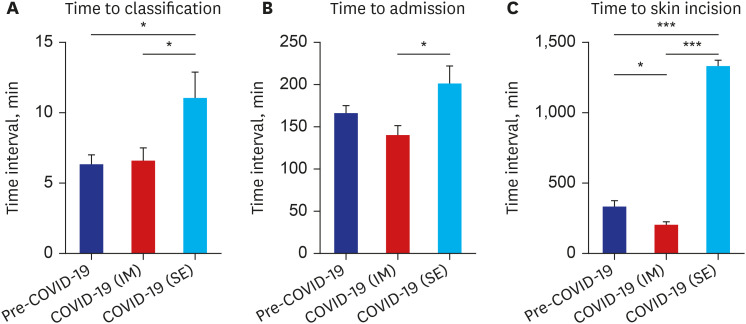
In the comparison of the time intervals of emergency processes among the three groups, significant differences were observed. The time interval from ER arrival to severity classification was significantly longer in the semi-elective surgery group during the COVID-19 period compared with the pre-COVID-19 group (P = 0.017) and immediate surgery group during the COVID-19 period (P = 0.035) (Fig. 3A). The time interval from ER arrival to admission was significantly longer in the semi-elective surgery group compared with the immediate surgery group during the COVID-19 period (P = 0.038) (Fig. 3B). The time interval from ER arrival to skin incision was significantly longer in the semi-elective surgery group during the COVID-19 period compared with the pre-COVID-19 group (P < 0.001) and immediate surgery group during the COVID-19 period (P < 0.001). In comparison with the pre-COVID-19 group, the immediate surgery group during the COVID-19 period rather showed a shorter time interval from ER arrival to skin incision (P = 0.040) (Fig. 3C).
Fig. 3
Comparison of the time intervals of emergency processes among the pre-COVID-19 group and COVID-19 subgroups.
(A) The time interval from ER arrival to severity classification was significantly longer in the semi-elective surgery group during the COVID-19 period compared with the pre-COVID-19 group (P = 0.017) and immediate surgery group during the COVID-19 period (P = 0.035). (B) The time interval from ER arrival to admission was significantly longer in the semi-elective surgery group compared with the immediate surgery group during the COVID-19 period (P = 0.038). (C) The time interval from ER arrival to skin incision was significantly longer in the semi-elective surgery group during the COVID-19 period compared with the pre-COVID-19 group (P < 0.001) and immediate surgery group during the COVID-19 period (P < 0.001). In comparison with the pre-COVID-19 group, the immediate surgery group during the COVID-19 period rather showed a shorter time interval from ER arrival to skin incision (P = 0.040).
COVID-19 = coronavirus disease 2019, COVID-19 (IM) = immediate surgery group during COVID-19 period, COVID-19 (SE) = semi-elective surgery group during COVID-19 period, ER = emergency room.
*P < 0.05; ***P < 0.001.
DISCUSSION
The spread of COVID-19 has infected more than 62,000,000 people in more than 200 countries by the end of November 2020, meeting the pandemic criteria defined by the WHO.612 Although most of the literature on COVID-19 is focused on the disease itself, there are some studies on the management of urgent non-COVID-19 conditions during the pandemic.13 From a neurosurgical perspective, COVID-19 requires that neurosurgeons balance the surgical needs of patients suffering from “urgent” diseases with the prevention of a possible infection outbreak.
COVID-19 is characterized by rapid transmission and long incubation periods, thus requiring rigorous screening.14 We proposed a clinical pathway for COVID-19 screening in patients who need emergency brain surgery. This clinical pathway aims to retain isolation measures and to minimize the likelihood of transmission of the virus in the hospital as much as possible.
The results of our study showed that the overall time interval from ER arrival to skin incision was significantly increased in the COVID-19 group; however, there were no effects on the clinical outcomes. The increase in the start time of surgery due to COVID-19 was significant; however, there was no delay in the time to skin incision among those requiring immediate surgery. The time interval to surgery initiation was longer in the COVID-19 group due to the increased time interval in the semi-elective surgery group. Screening processes such as the triage and nasopharyngeal swab did not significantly increase the time interval to classification and admission. As the semi-elective group consisted of patients with low severity, clinical outcomes were favorable even if surgery was performed late after COVID-19 confirmation.
We used common criteria that most neurosurgeons use to plan for emergency surgery and individualized the criteria on a case-by-case basis to make surgical decisions.1516 Subarachnoid hemorrhage was treated immediately by clipping or coiling. In the case of intracerebral hemorrhage or traumatic brain injury, decisions were made based on the neurological status, size and location of the bleed, age, and state of health of the patient. For chronic subdural hematoma, surgery was performed after the COVID-19 RT-PCR result was obtained, if GCS was not less than 10 (Table 1). Clinical outcomes were acceptable when using this method to classify indication for the semi-selective surgery group and perform surgery after COVID-19 confirmation, as shown in Table 5.
Most of the studies about emergency surgery during the COVID-19 pandemic focused on the operating room setting and PPE of medical workers rather than the screening and clinical pathway. Nevertheless, in the field of orthopedic surgery and traumatology, some studies reported hospital reorganization and clinical pathways for the treatment of traumatic and orthopedic patients during the COVID-19 period.171819 A study on vertebral fracture and spinal compression patients proposed a new protocol during the COVID-19 pandemic. According to the study, the time interval between admission and surgery and the length of hospital stay were reduced after the COVID-19 pandemic.20 This result can be said to reflect the intention of early surgery, early mobilization, and early discharge by lowering the threshold for surgical management rather than the 'watch and wait' strategy.20
In the field of neurosurgery, a review of the modified guidance algorithm that optimizes subarachnoid hemorrhage care and workflow during the COVID-19 pandemic has been reported.21 However, it seems that no studies have proposed a comprehensive clinical pathway for brain emergencies and established the validity of the protocol by comparing the clinical outcomes before and after the COVID-19 period.
There are several limitations in our study. First, this study was not a randomized prospective study but a retrospectively designed study. Therefore, there may be limitations due to the retrospective nature of the study. In addition, as this study was performed in a single tertiary medical center, there was a relatively small number of subjects. Due to this limitation, we were unable to statistically demonstrate that the clinical outcomes among patients who underwent semi-elective surgery during the pre-COVID-19 period and the COVID-19 period did not differ. However, this study aimed to promptly provide information to those who lack the relevant clinical experience in this pandemic. Therefore, even with a small number of subjects, the results of this study may provide a clinical basis for healthcare in a future situation similar to the current pandemic.
In summary, our study presented a clinical protocol to screen for and reduce the risk of nosocomial infections and to perform timely surgery. Considering the ongoing COVID-19 outbreak, our experience would be of value to neurosurgical emergency management in the present pandemic and future crises.
 XML Download
XML Download