

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endocrine disrupting chemicals (EDCs) are substances that influence the hormonal and homeostatic systems. They exert numerous effects on various receptors, enzymatic pathways involved in steroid biosynthesis and/or metabolism, and other mechanisms that are involved in the functioning of endocrine and reproductive systems.1
Bisphenol A (BPA) has estrogenic properties, and mainly used in the form of epoxy resins as coatings on the inside of food and beverage cans, and it is basic raw material of polycarbonate plastic. The major human exposure route to BPA is diet, including ingestion of contaminated food and water.2 After oral administration, BPA undergoes a first-pass metabolism in the gastrointestinal tract and liver and metabolizes to bisphenol A monoglucuronide (BPAG) and bisphenol A sulfate (BPAS). Both BPAG and BPAS are excreted in urine within 5–7 hours after oral administration.34 Human exposure to BPA has been confirmed based on the presence of BPA in various tissues including ovarian follicular fluid and has been linked to alterations in reproductive effects in animal models.5 In terms of infertility, there exist epidemiological studies demonstrating higher serum BPA levels in infertile women compared with fertile women.67 One epidemiological study showed a negative correlation between urinary BPA exposure and antral follicle counts in women undergoing in vitro fertilization (IVF) treatments.8
Phthalates also have estrogenic and anti-estrogenic properties on a living organism910 and mainly used as a plasticizer to increase the flexibility, transparency, durability, and longevity of plastics. Phthalate is absorbed through inhalation or oral and skin exposure.111213 Phthalate has a short biological half-life (less than 24 hours)14 and has been detected in various body fluids including blood, urine, breast milk, and follicular fluid.1516 Phthalates have been documented to cause female reproductive toxicity.17 An animal study revealed altered serum estradiol levels, advanced or delayed onset of puberty, increased ovarian and uterine weights and deficits in growing follicles and corpora lutea subsequent to exposure to phthalates.18 The majority of studies evaluating the effects of phthalates on ovarian function has focused on DEHP and MEHP, alteration in ovarian steroidogenesis and production of the gonadotropins by gonadotropes.19
The aim of the present study was to demonstrate the harmful effect of EDC exposure associated with the changes in ovarian reserve and the risk of gynecologic disease in reproductive-aged women.
Go to : 
METHODS
Study design and population
A total of 307 married women aged between 30 to 49 years volunteered for the study from September 2014 to November 2014 at Ewha Womans University Mokdong Hospital in Seoul of Korea. To minimize environmental differences, we restricted the study to women living in the three western districts of Seoul: Gangseo-gu, Mapo-gu, and Yangcheon-gu. The women volunteered following a notice on the bulletin board at the Ewha Womans University Medical Center, a support center for healthy families, a community health center, a community service center, and a community blog for mothers. Questionnaires were provided to all the participants and the answer sheets were collected. The questionnaire was categorized based on six subjects, including 1) personal data including socioeconomic status, 2) general daily life habits including alcohol intake, smoking and exercise, 3) medical history, 4) gynecologic history including previous gynecologic operation history, 5) environmental survey, and 6) dietary survey. Anthropometric measurements, including measurement of height, weight, and abdominal circumference were performed. Also, body mass index (BMI) was calculated. Laboratory tests with urine and blood samples were performed after midnight fasting for at least 8 hours. Infertility was defined as subjects who checked “yes” on the questionnaire about infertility treatment history and diagnosed with female infertility or unexplained infertility.
Pelvic ultrasonography
All the included subjects underwent pelvic ultrasound examinations by the 7-MHz transvaginal transducer (Volusion I, GE Medical Systems, Milwaukee, WI, USA) to detect uterine myoma, adenomyosis, endometrial polyp, and ovarian endometrioma. All the ultrasounds were performed by three experts, during the early follicular phase within 5 to 10 days of the menstrual cycle. Each ovary was scanned in the longitudinal cross-section from the inner to outer margins in order to count the total number of follicles which measured between 2 and 9 mm in diameter. The ovarian volume (OV) was calculated using the formula for a prolate ellipsoid (0.523 × length × width × thickness).20 Patients with history of ovarian surgery were excluded from this study.
Anti-Müllerian hormone (AMH) measurements
Blood samples were obtained by venipuncture and the venous blood samples were taken after overnight fasting for at least 8 hours, during the patient's follicular phase of menstrual cycle. In the case of women with amenorrhea, blood was sampled considering the ovarian morphology investigated by ultrasound. The serum AMH level was measured using enzyme-linked immunosorbent assay (ELISA) kit (AMH Gen II ELISA; Beckman Coulter Inc., Brea, CZ, USA) according to the manufacturer's instructions. It has a sensitivity of 0.57 pmol/L and reported intra- and interassay coefficients of variation of less than 5.6%, according to the products' inserts.
Urine sample collection and BPA/phthalate measurements
A single (spot) urine sample was collected for BPA and phthalate level measurement using a BPA-free polypropylene container. Mono-(2-ethyl-5-hydroxyhexyl) phthalate (MEHHP), mono-(2-ethyl-5-oxohexyl) phthalate (MEOHP) and mono-N-butyl phthalate (MnBP) were measured as phthalate metabolites. Clean-catch midstream urine samples were evaluated by high-performance liquid chromatography with tandem mass spectrometric (HPLC-MS/MS). The lower limit of detection (LOD) for BPA, MEHHP, MEOHP, and MnBP was 0.112 ug/L, 0.239 ug/L, 0.218 ug/L, and 0.329 ug/L (urine), respectively. As urinary levels of BPA and phthalate metabolites in single-spot samples can vary depending on urine output, we co-measured urine creatinine levels to correct for urine BPA and phthalate metabolites levels.21
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics Version 20 (Statistical Package for Social Science Japan, Inc., Tokyo, Japan). Quantitative variables are given as mean ± standard deviation. The age-matched AMH quartile percentile was based on normal levels in 1,298 Korean women with regular menstruation22 and subjects were divided into two groups to evaluate the effects of EDCs on AMH, and differences between the two groups were determined by Student's t-test. The DOR group was defined as AMH less than 25%. The Pearson correlation coefficient was used to analyze the correlation between AMH levels and each EDC levels. Linear regression analysis was used to evaluate the correlation between EDCs and antral follicle count (AFC) and OV. Logistic regression analysis was used to evaluate the contribution of each EDC exposure to myoma, adenomyosis, endometrial polyp, ovarian endometrioma, and infertility. Subjects were divided based on EDC level, as ≥ 90 percentile and < 90 percentile. The EDC high exposure group was defined as ≥ 90 percentile. P values of < 0.05 were considered to be statistically significant.
Ethics statement
The study protocol was approved by the Institutional Review Board of Ewha Womans University MokDong Hospital (No. 2014-06-014). All the participants provided written informed consent.
Go to :
RESULTS
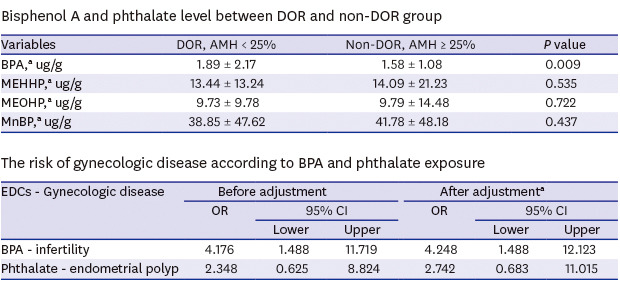
The mean age of the subjects was 36.8 ± 4.4 years and the mean BMI was 22.4 ± 3.1 kg/m2. Subjects were divided into two groups, based on AMH percentile according to age-specific serum AMH level, as the DOR group < 25 percentile and non-DOR group ≥ 25 percentile and the number of subjects in each group was 93 (30.3%) and 214 (69.7%), respectively (Table 1). The mean level of individual EDC was evaluated. In the DOR group, mean BPA level was 1.89 ± 2.17 ug/g, mean MEHHP level was 13.44 ± 13.24 ug/g, mean MEOHP level was 9.73 ± 9.78 ug/g, and mean MnBP level was 38.85 ± 47.62 ug/g. In non-DOR group, mean BPA level was 1.58 ± 1.08 ug/g, mean MEHHP level was 14.09 ± 21.23 ug/g, mean MEOHP level was 9.79 ± 14.48 ug/g, and mean MnBP level was 41.78 ± 48.18 ug/g. Accordingly, mean BPA level was noted to be significantly higher in the DOR group (Table 2).
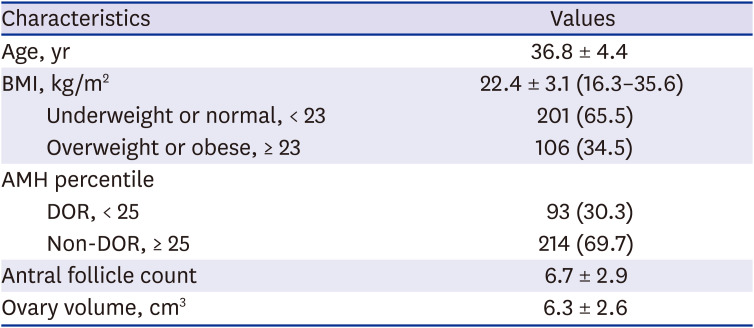

Table 1
Baseline characteristics of study subjects (n = 307)
Data are expressed as mean ± standard deviation or number (%).
BMI = body mass index, AMH = anti-Müllerian hormone.
![]()
Table 2
Bisphenol A and phthalate level between DOR and non-DOR group
DOR = diminished ovarian reserve, AMH = anti-Müllerian hormone, BPA = bisphenol A, MEHHP = mno-(2-ethyl-5-hydroxyhexyl) phthalate, MEOHP = mono-(2-ethyl-5-oxohexyl) phthalate, MnBP = mono-N-butyl phthalate.
P ≤ 0.05 were considered statistically significant.
aBPA and phthalate (ug/g creatinine) are corrected by urine creatinine.
![]()
As AMH is known to have a negative correlation with BMI, we adjusted AMH level with BMI and divided the patients into four groups. As per the grouping based on age, the number of subjects aged between 30–34 years (group 1) was 108, aged between 35–39 years (group 2) was 128, aged between 40–44 years (group 3) was 45, and aged between 45–49 years (group 4) was 26. As a result of Pearson correlation coefficient, the measured BPA was observed to be correlated negatively with BMI-adjusted serum AMH level in group 3 (Table 3).
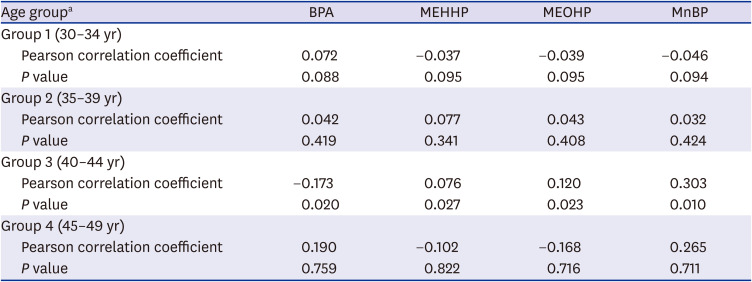
Table 3
Adjusted associations of age group between anti-Müllerian hormone and bisphenol A and phthalate level
BPA = bisphenol A, MEHHP = mono-(2-ethyl-5-hydroxyhexyl) phthalate, MEOHP = mono-(2-ethyl-5-oxohexyl) phthalate, MnBP = mono-N-butyl phthalate.
P ≤ 0.05 were considered statistically significant.
aBMI-adjusted.
![]()
Multivariable linear regression analysis showed no significant correlation between EDCs and AFCs or OV, after adjustment for age and BMI (Table 4).
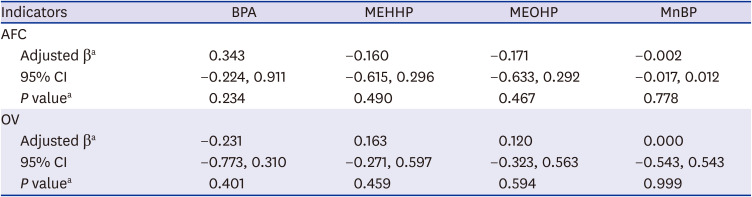
Table 4
The association of BPA and phthalate level with AFC or OV
BPA = bisphenol A, MEHHP = mono-(2-ethyl-5-hydroxyhexyl) phthalate, MEOHP = mono-(2-ethyl-5-oxohexyl) phthalate, MnBP = mono-N-butyl phthalate, AFC = antral follice count, OV = ovarian volume.
P ≤ 0.05 were considered statistically significant.
aMultivariate linear regression adjusting for age and body mass index.
![]()
Logistic regression analysis suggested an increase in infertility in BPA level ≥ 90 percentile group and the odds ratio (4.248) was statistically significant after adjustment for age, birth control pills, the age of menarche, parity, and waist circumference. The phthalate level ≥ 90 percentile group was associated with endometrial polyp after adjustment (odds ratio, 2.742). However, exposure to these EDCs revealed no significant associations with myoma, adenomyosis or ovarian endometrioma (Tables 5 and 6).
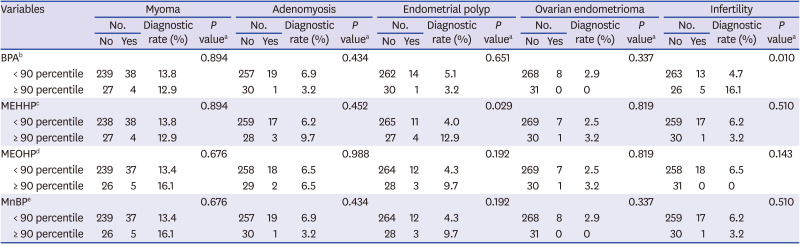

Table 5
The association of BPA and phthalate level with myoma, adenomyosis, endometrial polyp, ovarian endometrioma or infertility
BPA = bisphenol A, MEHHP = mono-(2-ethyl-5-hydroxyhexyl) phthalate, MEOHP = mono-(2-ethyl-5-oxohexyl) phthalate, MnBP = mono-N-butyl phthalate.
Bisphenol A and phthalate (ug/g creatinine) are corrected by urine creatinine.
aP ≤ 0.05 were considered statistically significant by chi-square; bBPA 90th concentration: 3.008 (ug/g crea.); cMEHHP 90th concentration: 24.126 (ug/g crea.); dMEOHP 90th concentration: 17.973 (ug/g crea.); eMnBP 90th concentration: 73.076 (ug/g crea.).
![]()
Table 6
The risk of gynecologic disease according to BPA and phthalate exposure
BPA 90th concentration: 3.008 (ug/g crea.); Phthalate 90th concentration: 73.076 (ug/g crea.).
BPA = bisphenol A, EDCs = endocrine disrupting chemicals, OR = odds ration, CI = confidence interval.
aAdjusted for age, birth control pills, age of menarche, parity and waist circumference.
![]()
In addition, to evaluate interactions between EDCs, the Pearson correlation coefficient was used and BPA level demonstrated significant correlation with all the measured phthalate metabolites (Table 7).
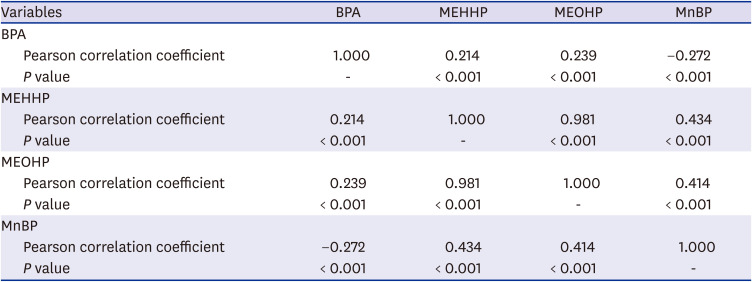
Table 7
Interactions between BPA and phthalate
BPA = bisphenol A, MEHHP = mono-(2-ethyl-5-hydroxyhexyl) phthalate, MEOHP = mono-(2-ethyl-5-oxohexyl) phthalate, MnBP = mono-N-butyl phthalate.
P ≤ 0.05 were considered statistically significant.
![]()
Go to :
DISCUSSION
The present study was designed to evaluate the associations between EDCs and ovarian reserve and the risk of development of health issues in Korean reproductive women. Although the effect of EDCs on human health remains ambiguous, several studies have demonstrated that some EDCs have adverse effects on reproductive health. Recent human studies indicate that BPA exposure in adults may be associated with infertility in the form of reduced ovarian response and IVF success, and negative effects on embryo quality and implantation failure.232425 BPA is likely to alter oviduct morphology and gene expression, affect implantation, and uterine morphology and function.2627 It is further hypothesized that BPA may affect estrous cyclicity and the expression of major determinants in the hypothalamic-pituitary axis, including kisspeptin and GnRH. Importantly, BPA has been regarded as an ovarian toxicant likely to act through multiple pathways including apoptosis, oxidative stress and folliculogenesis.28
Many studies have investigated the relationship between EDC exposure and ovarian reserve. Irene reported a negative correlation between urinary BPA concentrations and AFCs in women undergoing infertility treatment.8 Zhou et al.29 demonstrated that increased urinary BPA level was associated with significant decrease in AFC, and BPA was negatively associated with AMH and day-3 FSH, but neither of them demonstrated statistical significance. Messerlian et al.30 demonstrated that phthalate metabolites may adversely impact the size of the growing antral follicle pool, and showed a negative correlation with phthalate metabolites concentration and AFCs in women seeking infertility care. Our study demonstrated that women aged between 40–44 years had a significant negative correlation with AMH, and this might be due to the possibility of acceleration of normal ovarian aging by BPA exposure.
Furthermore, the studies on phthalate and estrogen-dependent diseases, including leiomyoma, adenomyosis and endometriosis report that women with higher MnBP or MEHHP exposure had an increased odds ratio for endometriosis or leiomyoma.31 Some studies have reported a higher exposure level of DEHP in Indian women with endometriosis.32 Our result showed increased MEHHP level in women with endometrial polyp; however, no significant correlation was observed with myoma or ovarian endometrioma. As etiology of these estrogen-dependent diseases is not completely known, and based on the possibility of demographic characteristics functioning as the potential risk factors, further studies are necessitated to clarify the presence of possible associations.
There are certain limitations of our study. First, our sample size was relatively small and it is possible that the smaller number did not provide adequate power to attain meaningful statistical significance. Secondly, exposures to EDCs are chronic; however, BPA and phthalate have relatively short half-lives which makes health risks assessment associated with EDCs a difficult task. Thirdly, evaluating the toxicity of a chemical is very difficult because humans are exposed to a mixture of different chemicals simultaneously. However, evaluation of toxicity of the mixture rather than single compounds is needed.33
On the other hand, we conducted a study with volunteers and not with the patients of an infertility clinic. This makes the study subjects represent a general population; however, we could not stringently confirm their medical history not to be included in our study.
EDCs are emerging as a great concern for human health. However, only a few studies have investigated the effects of EDC on Korean reproductive women. Despite the presence of evidence on the adverse effects of EDCs on various systems, larger studies with an aim to investigate potential interaction between EDC exposure and the etiology of gynecologic diseases are warranted.
In conclusion, BPA exposure might be associated with DOR and infertility. Meanwhile, the endometrial polyp is increased in women with high phthalate exposure. Therefore, the risk of exposures to EDCs for reproduction should be a matter of concern in reproductive-aged women.
Go to :
 XML Download
XML Download