

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Frozen shoulder (FS) is a disabling and painful disorder that affects the shoulder joint. It involves stiffness and pain that develops gradually.1 Even though the precise pathogenesis of FS is unclear, thickening of coracohumeral ligament (CHL) is considered as one of the key morphological changes.123 CHL thickening has been shown to restrict external rotation of the shoulder, and limited internal rotation of the shoulder is believed to be associated with posterior capsular tightness.345 Prompt diagnosis of FS followed by treatment with physical therapy or intra-articular corticosteroid injection shortens the duration of the joint stiffness and pain, thereby significantly reducing patient morbidity.678 The diagnosis of FS includes shoulder pain, shoulder joint stiffness for more than four weeks, and absence of other shoulder abnormalities.8910 However, the symptoms are variable and the clinical diagnosis is difficult in the early phases of FS.6 If the diagnosis is unclear due to atypical clinical symptoms, imaging techniques can be a key in FS diagnosis. The CHL plays an important role in the function of the rotator interval.111213 In a biomechanical study, the tension of the CHL played a major role in the range of motion (ROM) and stability of the glenohumeral joint.14 Shoulder Magnetic resonance imaging (S-MRI) revealed the pathological condition of the CHL and other associated pathological evaluation in the shoulder joint.2 Previous research assessed the CHL using a simple and ambiguous measurement at approximately “halfway” or “middle” of the CHL.3 However, CHL is composed of sparse and irregular fibers enriched with type 3 collagen, which results in flexibility.12 Thus, measurement error depends on the cutting angle, and measurement point. Therefore, we devised an unambiguous morphological parameter, called the coracohumeral cross-sectional area (CHLA) for the evaluation of hypertrophy of the whole CHL. In contrast to CHLT, the CHLA is relatively free from measurement errors caused by measurement point as it analyzes the cross-sectional area of the CHL. We hypothesized that the CHLA is a major morphologic parameter in the diagnosis of FS and compared CHLA and CHLT between FS patients and control groups using S-MRI.
METHODS
Study population
The Independent Ethics Committee of the authors' affiliated institutions approved the current retrospective research and waived the requirement for informed patient consent. We reviewed patients who had been diagnosed with FS at our shoulder orthopedic center from December 2015 to July 2018. The inclusion criteria were as follows: 1) insidious onset pain without any anatomic or imaging abnormalities; 2) symptoms lasting for at least 12 weeks to 12 months; 3) routine S-MRI conducted at initial evaluation (joint capsule and synovium thickness > 4 mm)15; 4) restrictive active and passive ROM of the shoulder (forward flexion < 100°, external rotation < 10° degrees, internal rotation < L5 level)16; and 5) limitation of passive ROM shows a capsular pattern (external rotation, abduction and internal rotation). FS was confirmed when the joint capsule and synovium thickness exceeded 4 mm on MRI by two experienced board-certified shoulder image radiologists. There were 20 (38.5%) men and 32 (61.5%) women with an average age of 57.06 ± 7.29 years (range, 41 to 74 years). To compare the CHLA and CHLT between FS patients and people without FS, we included individuals in the control group who showed similar clinical symptoms as FS, such as inclusion criteria, during December 2018 to July 2019 and showed normal findings after scanning S-MRI for differential diagnosis. The control subjects included 51 individuals (18 men and 33 women) with an average age of 56.47 ± 5.47 years (range, 43 to 65 years). Exclusion criteria were: 1) previous shoulder trauma; 2) previous shoulder surgery; 3) past history of cervical spine disease; 4) calcium deposits on shoulder X-ray; 5) laboratory test positive for rheumatoid factor and anti-cyclic citrullinated peptide antibodies suggesting rheumatoid arthritis; and 6) rotator cuff tears on S-MRI. Fifty-two patients with a clinical diagnosis of FS were recruited.
MRI protocol
MRI was performed with 3.0-T S-MRI system (Magnetom Skyra; Siemens Medical Solutions, Erlangen, Germany) and 3T scanner (Ingenia; Philips Healthcare, Amsterdam, Netherlands). For all S-MRI examinations, we obtained images in the oblique sagittal T2-weighted turbo-spin-echo (TSE) images with < 3.0 mm slice thickness, 2,156-ms/80-ms repetition time/echo time, 160 × 160-mm field of view, 308 × 301 matrix, and 0.9-mm intersection gap.
Image analysis
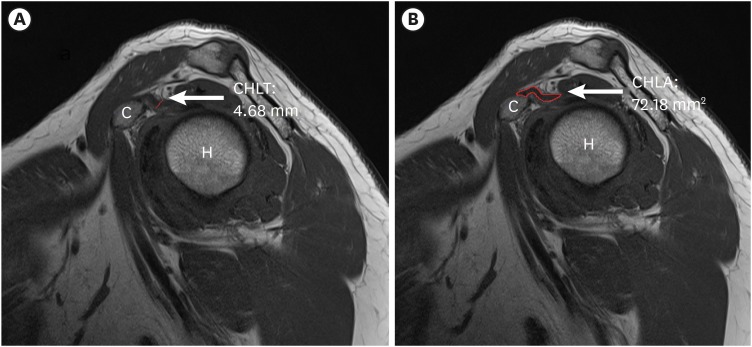
CHLT and CHLA measurements were performed by the one pain specialist, who was blinded to the diagnosis of FS. As in previous studies,217 oblique sagittal T2-weighted TSE S-MR images were acquired at the thickest visualization of CHL. We measured the CHLT and CHLA on S-MRI using a picture archiving and communications system (INFINITT; Medical solutions, Seoul, Korea) (Fig. 1). The CHLA was measured as the whole area of the CHL including the most hypertrophied part of the MR images on the oblique sagittal plane. The CHLT was measured at the thickest point of the CHL.
Statistical analysis
Baseline characteristics of the FS and control groups were compared using unpaired t-tests. All values were presented as mean standard deviation. The validity of the CHLA and CHLT for diagnosis of FS was calculated by using a receiver operating characteristic curve quantified by the area under the curve (AUC, 0.5; non-informative around 1; perfectly complete test),18 sensitivity, specificity and overall accuracy. P value < 0.05 was considered to indicate a statistically significant difference. IBM SPSS version 22 for Windows (IBM Corporation, Armonk, NY, USA) was used for the all statistical analysis.
RESULTS
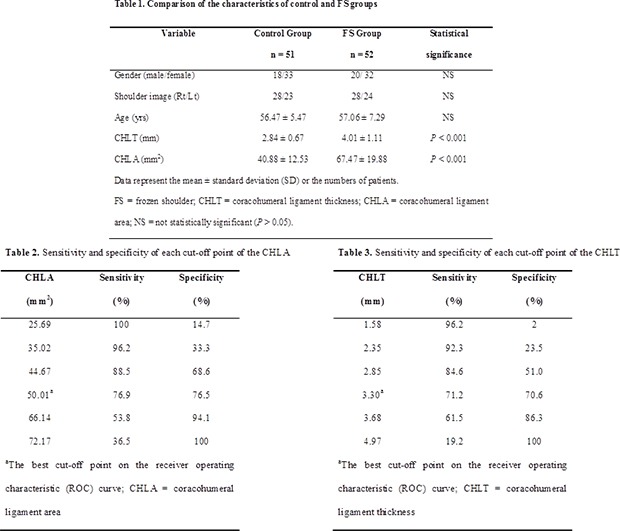
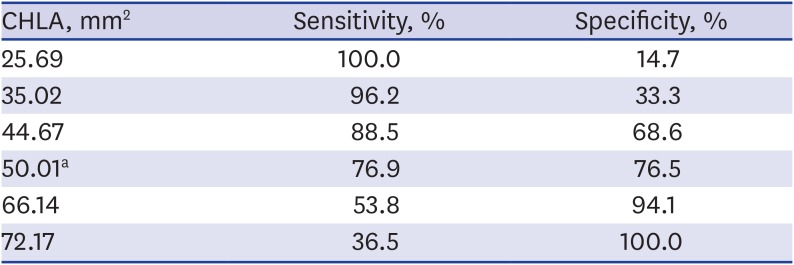
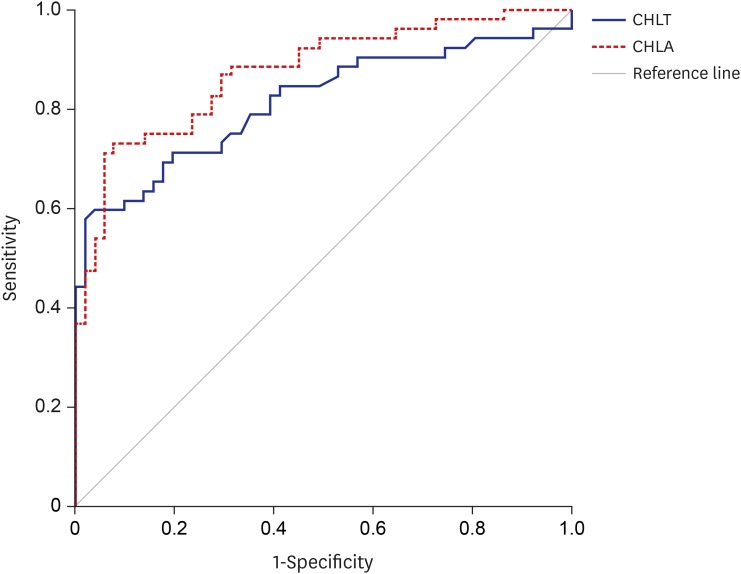
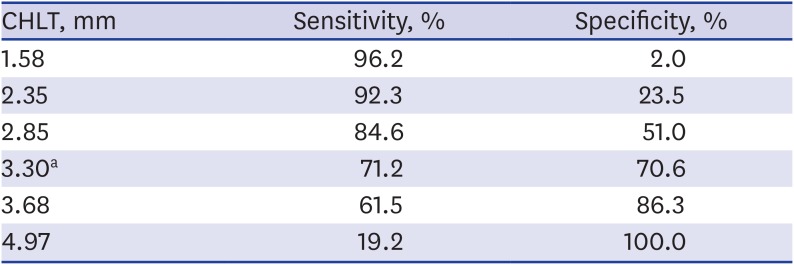
The average CHLA was 40.88 ± 12.53 mm2 in the control group and 67.47 ± 19.88 mm2 in the FS group. The mean CHLT was 2.84 ± 0.67 mm in the control group and 4.01 ± 1.11 mm in the FS group. FS patients had significantly higher CHLA (P < 0.01) and CHLT (P < 0.01) than the control group (Table 1). The receiver operator characteristic analysis showed that the most suitable cut-off score of the CHLA was 50.01 mm2, with 76.9% sensitivity, 76.5% specificity (Table 2), and AUC of 0.87 (95% confidence interval [CI], 0.81–0.94) (Fig. 2). The most suitable cut-off value of the CHLT was 3.30 mm, with 71.2% sensitivity, 70.6% specificity (Table 3), and AUC of 0.81 (95% CI, 0.73–0.90) (Fig. 2). Comparison between the two AUCs showed no statistically significant difference (P = 0.105).
Table 1
Comparison of the characteristics of control and FS groups

Table 2
Sensitivity and specificity of each cut-off point of the CHLA
| CHLA, mm2 | Sensitivity, % | Specificity, % |
|---|---|---|
| 25.69 | 100.0 | 14.7 |
| 35.02 | 96.2 | 33.3 |
| 44.67 | 88.5 | 68.6 |
| 50.01a | 76.9 | 76.5 |
| 66.14 | 53.8 | 94.1 |
| 72.17 | 36.5 | 100.0 |
Fig. 2
ROC curve of CHLT and CHLA for confirmation of FS. The best-cut-off-point of CHLA was 50.01 mm2 vs. 3.30 mm of CHLT, with sensitivity 76.9% vs. 71.2%, specificity 76.5% vs. 70.6%.
ROC = receiver operating characteristic, CHLT = coracohumeral ligament thickness, CHLA = coracohumeral ligament area, FS = frozen shoulder.
DISCUSSION
The diagnosis of FS is limited by the lack of objective standards of comparative testing, but is essentially clinical.19 Therefore, an MRI is not necessary to diagnose all FS patients. However, it may be necessary to exclude other causes that may be confused with the FS, such as rotator cuff tear, tendinitis, osteoarthritis, subacromial impingement, and occult fracture.202122 The CHL is thickened and shortened in FS, and a thickened CHL is considered as one of the major FS morphology, and the key ligament for ROM recovery.23232425262728 Kanazawa et al.25 demonstrated that CHL thickening is significantly correlated with ROM restrictions in external rotation, forward flexion, and hand position behind the back. DePalma29 noted for the first time that the CHL often shorten on the FS, limiting the external rotation of the affected side. In histological studies, Leffert30 emphasized CHL hypertrophy, one of the pathogenesis of FSs. Ozaki et al.31 demonstrated fibrosis and hyalinization of connective tissue at rotator intervals including CHL were shown in chronic FS patients. The evidence that CHL is a major factor of FS is also closely observed in the surgical release of CHL. Ozaki et al.31 presented a study of open surgical release of contracted CHL and rotator interval. This procedure restored motion of the shoulder and decreased pain in all patients. Neer et al.4 reported that sectioning of tight CHL in five fresh cadavers increased an average of 32 degrees on external rotation (range, 30–40 degrees). Tetro et al.32 showed that the arthroscopic release of a normal CHL gained external rotation by 35° in adduction. Also, Yukata et al.27 presented that after ultrasound (US)-guided CHL release, the average gain in external rotation was 29°. Subsequently, several S-MRI studies have shown that the CHL is one of the major diagnostic findings in FSs.333435 Li et al.2 reported that S-MRI is a satisfactory modality for CHL depiction, and a thickened CHL is highly suggestive of FS. They found that the CHL thickness (= 3.08 mm) in the control group was significantly smaller than the thickness (= 3.99 mm) in patients with FS. Our results also demonstrated that the CHLT in those without FS was 2.84 mm, and was 4.01 mm in FS. Homsi et al.3 reported that the mean thickness of CHL using US was 3.0 mm in FS groups, compared with 1.34 mm in asymptomatic shoulders. However, US in FS has several limitations such as poor visualization. The CHL is visualized on all planes, and identified in the middle portion of the rotator cuff interval. However, as the sagittal images enable the analysis of CHL based on S-MRI, the thickest portion of the CHL was measured on sagittal, T2-weighted, and TSE oblique images in our study. Previous research focused only on the CHLT.13 However, Arai et al.12 reported that the CHL is composed of sparse and irregular fibers and an abundance of type 3 collagen, for flexibility. Yang et al.36 demonstrated that the CHL is irregular trapezoidal structures located in rotator interval and its origin is similar to that of the coracoid process, but the insertion sites vary, including supraspinatus, subscapularis tendon, or rotator interval. Neer et al.4 Showed similar results for the origin and insertion sites of CHL. Toprak et al.37 presented a study comparing thickness and cross-sectional area for evaluation of patella tendons with different origin and insertion shapes. Their results allow them to use thickness/area ratios to determine risk predictions for tendinosis. They mentioned a nonhomogeneous structure, patellar tendon, so the researcher should be able to see it as a three-dimensional structure instead of just measuring the thickness of the tendon. Therefore, the CHL becomes curvilinear and irregular in shape, and the measurement error depends on the cutting angle and the measurement point of the single slice image. In contrast to CHLT, CHLA based on the cross-sectional area of CHL can be considered to have at least a few measurement errors due to cutting angle or measurement point of CHL. Several measurements should be made to find the thickest ligament thickness in a single cut image when based on thickness, but the area should be based only on the maximum contour, which can save the rater's effort. Bang et al.38 also reported that for the same reason, the area of ligament is better than thickness in diagnosing adhesive capsulitis. We hypothesized that the oblique sagittal area of the CHLA may predict FS. We also found that the CHLA is comparable to the CHLT as a morphological parameter of FS. In the current study, we found that the CHLA showed 76.9% sensitivity, 76.5% specificity, and AUC of 0.87 (95% CI, 0.81–0.94) to confirm FS. The CHLT showed 71.2% sensitivity, 70.6% specificity, and AUC of 0.81 (95% CI, 0.73–0.90). However, comparison between the two AUCs showed no statistically significant difference (difference between areas = 0.0601; 95% CI, −0.0127–0.133; P = 0.105). These findings suggest that the CHLA has statistically equivalent power to CHLT.
We acknowledge several limitations in our present study. These data excluded symptom onset time, and clinical correlation between treatment and follow-up. Because FSs have the onset of insidious symptoms, it is difficult to assess the exact onset. Second, CHL has been shown to involve both intra- and extra-articular structures with superficial and deep limbs. This may result in measurement errors within or between raters. Because this bias may exist in our study where one evaluator measured CHLA only once, it is important to design a study to reduce this risk in future studies. However, according to previous studies, the typical error between examiners was below 2% for all the measured cross sectional areas.39 Also, cross sectional area measured by MRI showed no statistical difference from intraoperative findings.40 Thus, although we could not demonstrate the reliability of this study, we still believe it is valuable by presenting the confirmatory MRI finding of FS. Third, in order to have adequate statistical power, it is necessary to increase the number of samples in a future study. Fourth, the morphological parameters on MRI may be associated with age, gender, height, weight, hand dominance, diabetes mellitus, previous steroid injection, and stage of adhesive capsulitis,41424344454647 which were not considered in our study. In particular, the thickness and area of CHL may vary depending on the stage of FS. The glenohumeral ligament becomes thinner after thickening to stage 2,17 and CHL is also likely to follow this trend. In this study, the inclusion criteria were set at 3 months to 12 months, but other results may be presented if we proceeded with patients corresponding to stage 1, 3 or 4. These should also be considered in later studies to eliminate bias arising from demographic characteristics. Fifth, this study is retrospective, and the correlation between CHLA, CHLT and ROM has not been investigated. Further studies that correlate these factors will help clinicians understand the symptoms of joint disease.
Nevertheless, this study is considered meaningful as the first report to introduce CHLA with good accuracy.
In conclusion, the significantly positive correlation between the CHLA, CHLT and FS was found. We also demonstrate that the CHLA has statistically equivalent power to CHLT. Thus, for diagnosis of FS, the treating physician can refer to CHLA as well as CHLT.
 XML Download
XML Download