

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The majority of women experience natural menopause at their age between late 40s and early 50s globally.12 Although population-based data are limited, premature menopause is known to occur in approximately 1%–8.6% and early menopause occurs in 4.9%–9.4% of women.345 Earlier menopause is an irreversible event and has lifelong consequences, including an increased risk of neurological impairment, glaucoma, cardiovascular disease, osteoporosis, mental disorders, and general mortality.6789 Hormone therapy alleviates some of the adverse effects.1011 Thus, if possible, prediction and prevention through the modification of risk factors would be crucial for improving women's health.
The etiology of earlier menopause remains elusive. Although several genes identified play roles particularly in the development of premature menopause,1213 they cannot explain majority of cases.14 Environmental and behavioral factors, such as obesity, ethnicity (African–American or Hispanic ancestry), early onset of smoking, higher parity, and lower socioeconomic status, are also associated with early menopause.1516 Early menarche is associated with earlier menopause in several studies,1718 which was not replicated in others.1920 Likewise, nulliparity was associated with higher risk of early menopause in European cohort,521 but not in a study of Japanese women.22 Socioeconomic factors that were found to be associated with early menopause in European women,232425 but not significant in Northern India population.26 This heterogeneity in the effect of biologic and social factors on age at menopause across ethnicities, cultural context, or data source may contribute to general incidence of premature or early menopause.27
Globally, age at natural menopause is increasing across populations.28 Considering that reported risk factors for earlier menopause, such as smoking in women, nulliparity, obesity, and early menarche, are increasing, this change might have exerted pressure toward increase in premature or early menopause, rather than decrease, which seemingly conflicts with observed trends of delays in menopause.29 In addition, environmental studies suggested that exposures to endocrine disruptors are constantly increasing, which might deplete ovarian reserve and fasten natural menopause.30 However, whether the general trend in the delay of menopause is parallel to the reduction of earlier menopause is not clear.
Few studies have depicted the trends of premature or early menopause and possible birth cohort effects controlling for multiple covariates in different ethnic groups. Because prevalence of premature menopause is as low as 1%, large population would be necessary to conduct epidemiologic study. We aimed to explore and compare the trends of premature or early menopause between women in three ethnic groups in the US and Korea using nationally representative population data collected through similar survey methods.
METHODS
Study population
Our study comprised two groups of women groups (women from the US and Korea aged 45 or over). Data of US women was retrieved from eight waves of the National Health and Nutrition Examination Survey (NHANES) conducted from 1999 to 2014. Korean data was obtained from seven waves of the Korea National Health and Nutrition Examination Survey (KNHANES) conducted from 2007 to 2012, which used the same questionnaire on the onset of smoking as the NHANES. Although the general survey method and questionnaires are not completely identical, the survey method and modalities of the KNHANES are similar to those of the NHANES because the survey was developed in reference to the NHANES.
The NHANES is among the series of health-related programs conducted by the Centers for Disease Control and Prevention of the National Center for Health Statistics. Approximately 5,000 people per year participated in the NHANES. It is a collection of demographic, socioeconomic, dietary, and health survey data for a nationally representative sample of the resident civilian non-institutionalized US population.31 As described elsewhere, a four-stage sample design was used in the NHANES.32
The KNHANES is a nation-wide survey in Korea, organized by the Korea Centers for Disease Control. Each wave provides nationally representative data for the Korean population. For stratification, survey population was sampled using “rolling survey sampling,” which is described previously.33 In each wave, a new sample of about 10,000 individuals comprised approximately 200,000 geographically defined primary sampling units (PSUs). Each PSU contained approximately an average of 60 households, and 20 final target households were selected by systematic sampling from each PSU.
During both surveys, participants were interviewed on their socio-demographic characteristics by trained interviewers. Information about age at menarche, level of education, relative quartiles of household income (reference to the household income level of the total population) was obtained from a face-to-face interview. Body mass index (BMI) data was obtained from examination data. We assessed smoking history using self-reporting questionnaires. Because both datasets are publicly available survey datasets which do not contain identifiable private information, this study does not require IRB approval.
Study variables
Based on the NHANES data, the participants were classified as one of the following: all Hispanic (Mexican American and other Hispanics), non-Hispanic white, non-Hispanic black, and other races (including multi-racial). As an indicator for individual economic status, household income that falls below the poverty line ratio was used, which measures the relative household income that considers family size.34 The relative level of household income that falls below the poverty line ratio in each ethnic group was included in the model as quartile scales. Educational attainment status was categorized into three groups: middle school graduation or lower, high school graduation, and college graduation or higher. Based on the NHANES data obtained from 1999 to 2014, smoking history (onset of smoking) was available among the relevant lifestyle factors during the premenopausal period. Because only smoking was associated with the occurrence of menopause,35 women who started smoking before the age of 40 were considered as smokers. Reproductive history included early menarche, primiparity, and age at last menstrual period. Early menarche was defined as menarche before the age of 12. Age at menopause was considered as age at natural menopause for all the women excluding those with a history of hysterectomy or bilateral oophorectomy before menopause.
The KNHANES shared survey questions for age at menarche, number of live births, and age at last menstrual period which are well-known determinants for timing of menopause.3637 For an economic status indicator, the ratio of family income to poverty line was used in the NHANES and relative household income for family size in KNHANES were used because no identical indicator for relative household income were available for both datasets. For both survey data, oral contraceptive use and current alcohol drinking were not included in the covariates because its information at the time of the survey does not represent the past exposure.
Determination of premature and early menopause
The menopause state was assessed by asking “What is the reason not having a period these days?” The information on age at menopause was obtained only from participants who have answered “naturally menopaused”. We defined natural menopause as menopausal state which is not the consequence of medical treatment, hysterectomy or bilateral oophorectomy. Those who did not experience menopause at the time of survey were considered to have neither premature nor early menopause. We excluded women who had any history of hysterectomy or bilateral oophorectomy and reported menopause induced by medical treatment before 40. Women without menstrual history who were born before 1920 or after 1969 or with unclear cause of menopause were also excluded from the final analysis. Due to the limited number of populations (5.7%) and unknown composition of nationality, US ethnic group classified ‘others’ were excluded from the final analysis. The ‘others’ ethnic group included peoples from the Far East, Southeast Asia, or the Indian subcontinent were among the Asians.32 Following previous studies, we defined premature menopause as having final menstruation before the age of 40 years. Early menopause is defined as being menopaused at the age of 40-45 years.538
Statistical analysis
We compared mean and proportions calculated with weighted values considering sampling design to explore homogeneities among three ethnic groups and Korean. Correlation structures among the key covariates, such as menarcheal age, number of deliveries, BMI, level of education, and household income, were assessed using R (ver. 3.5.0; R Foundation for Statistical Computing, Vienna, Austria). We used weighted results for all of the analyses stratified by four ethnic groups: all US Hispanic, US non-Hispanic white, US non-Hispanic black (from NHANES), and Koreans (from KNHANES). We defined birth cohort based on the reported year of birth. We explored linear trend of birth cohort-specific prevalence of premature and early menopause using logistic linear regression analysis. We calculated adjusted odds ratios (ORs) and 95% confidence intervals for each of birth cohort. When calculating ORs for early menopause, reference group excluded premature menopause cases. We adopted sampling weight-based survey analytics using SAS 9.4 software (SAS Institute, Cary, NC, USA).
RESULTS
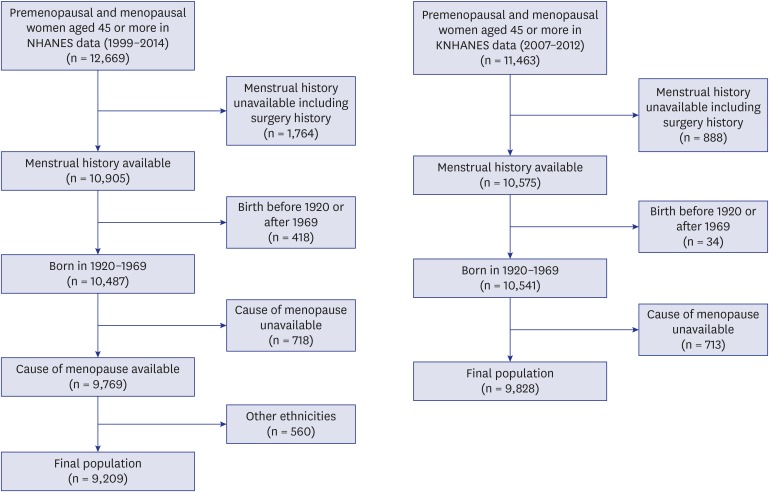
Among 12,669 women aged 45 or over at the time of the survey in the NHANES data, 9,209 (72.7%) US women met the inclusion criteria and were included in the study. In the KNHANES, among 11,463 women aged 45 or over at the time of the survey, 9,828 (85.7%) women were included in the analysis (Fig. 1).
Fig. 1
Exclusion of study population of US (NHANES, 1999–2014) and Korean women (KNHANES, 2007–2012).
NHANES = National Health and Nutrition Examination Survey, KNHANES = Korea National Health and Nutrition Examination Survey.
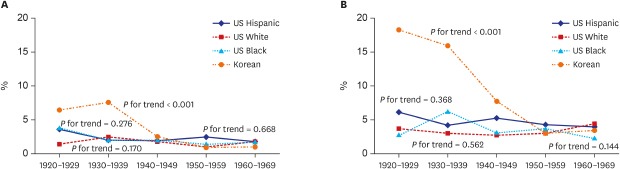
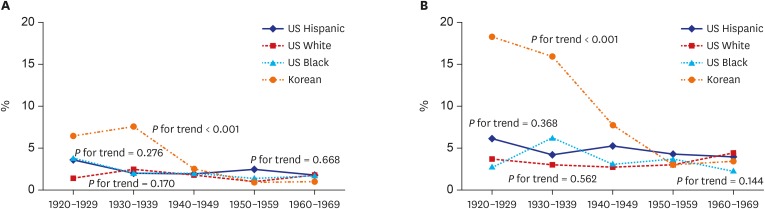
In pooled data, prevalence of premature menopause was 1.7% in US, 2.8% in Korean women. Early menopause occurred in 3.4% and 7.2% of US and Korean, respectively. Premature and early menopause in Korean women peaked among those born in 1920s and consistently decreased in younger generations (P < 0.001 for premature and early menopause) (Fig. 2). In the US women, there was no secular change in all three ethnic groups for both premature and early menopause.
Fig. 2
Trend of cohort-specific prevalence of premature and early menopause in the three ethnic groups in US and Korean women. (A) Premature menopause (< 40 years), (B) Early menopause (40–44 years).
Median age at the time of survey ranged from 57.3 to 61.0 years. Median age of at natural menopause was 47.3–49.4 years (Table 1). US non-Hispanic white women had the lowest prevalence of premature (1.7%) and early (3.2%) menopause, and Koreans had the highest (2.8% of premature and 7.2% of early menopause). Prevalence of premature and early menopause was not different among the three ethnic groups of the US. Korean women had higher premature (< 0.001) and early (< 0.001) menopause rate. A higher proportion of US women (27.7%–43.8%) started smoking before 40 compared than Korean (5.6%). The weighted mean age at menarche was higher in Korean women (15.2 years) than that of US women (12.7–12.9 years). The majority of non-Hispanic white (59.5%) and black (47.3%) women had college education. On the other hand, more than half of the US Hispanic and Korean women had middle school or lower education. Mean number of deliveries ranged from 2.6 to 3.8. There was weak and moderate correlation between each pair of covariates, including menarcheal age, number of deliveries, BMI, level of education, and household income (Supplementary Fig. 1). Among non-Hispanic black women, those born in 1950s showed lower risk for premature menopause. Birth cohort effect was evident in Korean women showing decreasing risk for premature menopause for those born in 1940 or later (Table 2). For early menopause, none of the birth cohorts showed higher risk in the three US ethnic groups. Korean women born in 1940s and later showed consistently lower risk for early menopause.
Table 1
Demographic characteristics of study population of US (NHANES, 1999–2014) and Korean women (KNHANES, 2007–2012)
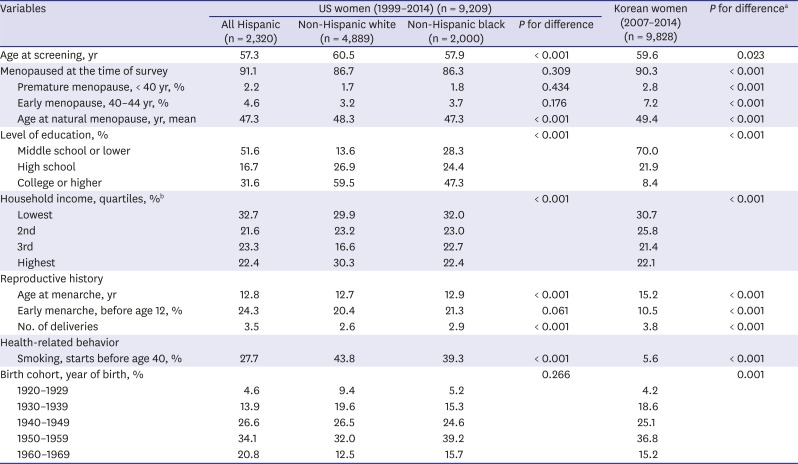
All means and frequencies are calculated using weighted values considering survey sampling.
NHANES = National Health and Nutrition Examination Survey, KNHANES = Korea National Health and Nutrition Examination Survey.
aP values are calculated for difference between the four ethnic groups; bSame household income quartiles were applied for all three US ethnic populations. Household income quartiles for entire Korean population were applied for Korean women.
Table 2
Adjusted OR for premature (< 40 years) and early (40–44 years) menopause in the three ethnic groups in US (NHANES, 1999–2014) and Korean women (KNHANES, 2007–2012)
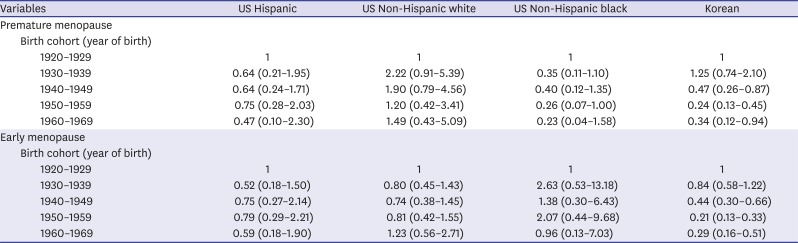
Values are presented as OR (95% CI). Analyses were performed using weighted values (‘proc surveylogistic’ command). ORs are from multivariable models adjusted for body mass index, early menarche, nulliparity, education, household income and smoking started before 40 years old. In the analysis of early menopause, women who had experienced premature menopause were excluded.
OR = odds ratio, NHANES = National Health and Nutrition Examination Survey, KNHANES = Korea National Health and Nutrition Examination Survey, CI = confidence interval.
DISCUSSION
The present study explored temporal trend and risk factors for premature and early menopause among women in the US and Korea using population-based data which is based on the same questionnaires. Particularly, when controlling for BMI, number of deliveries, education, household income, smoking and birth cohort, association of year of birth with premature and early menopause was not identical across three ethnic groups and Korean. This finding suggests that birth cohort effect can be different across ethnicities and national context. Premature or early menopause did not decrease in the three US ethnic groups. We observed downward trend only in Korean women. Specifically, premature menopause decreased in US black women born in 1950s and Korean women born in 1940s and later. To the best of our knowledge, this is the first study exploring premature and early menopause using combined dataset from NHANES and KNHANES.
Our finding shows similar prevalence of premature and early menopause across three ethnic groups and birth cohorts in the US women. However, ethnic difference in prevalence have been reported both for premature and early menopause. In the US population, African American (1.4%) and Hispanic (1.4%) women showed highest and Asian (0.1%–0.5%) women had lowest risk for premature menopause.3 Recent observational study of UK, Scandinavia, Australia and Japan women showed generally higher risk in UK population (1.0%–3.6%) compared to the others.5 For early menopause, the prevalence was between 4.9% and 9.4% in the same study population.5 Although the size of population is small, 22.9% of Nigerian women experience menopause before age of 45 years.39 This similar prevalence of premature and early menopause among different ethnic groups within the US population would be due to potential effect of early childhood on menopausal timing.20 Similar environment in early stage of life would have affected the more similar menopausal timing within the country. In a clinical study of single medical center, women whose birthplace is outside of US had higher incidence of premature menopause.40
Given the increasing trend of age at natural menopause, we can expect the numbers of women who experience premature or early menopause to decrease over time accordingly. However, downward pattern of premature and early menopause was evident only in Korean women. According to a previous multi-ethnic study, both the incidence of premature and early menopause in Korean women born before 1940s is even higher than in Japanese born during the similar period.3 Korean women born in 1920s and 1930s would have been malnourished and socially deprived during their adolescence or young adulthood because of the Korean War occurred in the early 1950s. Epidemiological studies have indicated that caloric restriction or malnutrition during childhood is linked with earlier age at natural menopause.414243 Weight gain in early childhood, however, was associated with later menopause.44 Downward trend of premature and early menopause prevalence in younger generation may reflect improved nutritional status and better environment.
As a cross-sectional study using a combined national data, we have several limitations. First, covariates such as BMI and household income were assessed at the time of survey and might have led misclassification. However, the effect of this bias would be minimized because BMI classification is likely to remain consistent through middle and older age groups.45 Second, several predictors for earlier menopause were unavailable in our study. Information of family history of premature menopause (US and Korean), history of unilateral oophorectomy (Korean), history of oral contraceptives use (Korean) and environmental exposure to heavy metals at the time of menopause were missing and alcohol dose at the time of menopause was incomplete (US). According to a survey conducted in 2015–2017, most common contraceptive methods used were found to be female sterilization (18.6%), oral contraceptive pill (12.6%), and long-acting reversible contraceptives (LARCs) (10.3%) all of which are potentially associated with timing of menopause.46474849 Duration and type of contraception is known to be associated with timing of menopause but they are also affected by menopausal status.50 Given that the composition of oral contraceptives was similar between 2008 and 2014,51 we believe the effect of oral contraceptive use on the trend of premature or early menopause would have been minimal. Lastly, cultural or lifestyle differences between the US and Korean women could have interfered comparability. For example, a study reported a stronger association of dietary carbohydrate with metabolic syndrome in Korean than in American which was due to higher consumption of carbohydrate.52 Likewise, dietary or nutritional difference between Western and Asian cultures could have affected on the associations in this study. Considering the cultural and ethnical diversity within the US women, we believe that the impact of dissimilarities would have been minimal in our analyses.
In conclusion, despite the generally increasing mean age of menopause of the US and Korea, we found downward trend of premature and early menopause only in Korean women. The understanding of the ethnic-specific difference in the trend may attribute to more effective prevention and management of premature and early menopause.
 XML Download
XML Download