

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Tympanosclerosis is associated with sclerotic changes in the tympanic membrane (TM), middle ear cavity, ossicular chain, or (rarely) mastoid cavity; it is characterized by the deposition of degenerated hyaline and calcification of collagen fibrils in the submucosal layer. Tympanosclerosis limited to the TM is known as myringosclerosis,1 and can be defined as a localized tissue reaction involving hyalinization and calcification of the middle fibrous layer of the TM.2 Myringosclerosis is generally asymptomatic, but may cause conductive or mixed type hearing loss if it affects the movement of the TM, ossicular chain, or windows.3
Myringosclerosis is the most common complication after ventilation tube insertion (VTI),45 which has been used for the treatment of otitis media with effusion (OME).56 The etiology and pathogenesis of this condition have not been fully elucidated; however, VTI, middle ear infection, trauma, genetic tendency, and increased formation of oxygen-derived free radicals have been proposed as risk factors for myringosclerosis.7 Sclerotic changes caused by myringosclerosis could render the TM stiff and inflexible, with fixation of the ossicular chain.8 Therefore, a small myringosclerosis may not affect hearing, while a more extensive plaque may lead to the onset of conductive hearing loss.9 Hearing loss caused by OME itself or myringosclerosis in childhood could result in a detrimental effect on the development of auditory temporal processing, and language development.10
Although VTI is the most common procedure used for the treatment of OME and is presumed to be associated with myringosclerosis, there have only been a few studies of potential risk factors for myringosclerosis after VTI.711 This study was performed to investigate possible risk factors for myringosclerosis formation after VTI and to determine factors affecting the severity of myringosclerosis after VTI.
METHODS
Patients
The study population consisted of 582 patients who underwent VTI for OME between January 2011 and March 2016 at Chungnam National University Hospital (Daejeon, Korea). Unilateral VTI was performed in 364 patients, while bilateral VTI was performed in 218 patients. All patients had undergone monthly follow-up for at least 6 months postoperatively. Patients with craniofacial anomalies, such as cleft lip and palate or Treacher-Collins syndrome, as well as those with insufficient medical records or otoscopic images, were excluded from the study. Patients with myringosclerosis before VTI were also excluded. In patients with bilateral VTI, only the left ear was included in the analysis of risk factors, in order to reduce the potential for bias originating from differences in myringosclerosis formation between ears in each patient.
Data collection
Patient data and clinical information were retrospectively collected through medical records review. Patient data collected included the following variables: age; gender; VT type; duration of effusion; characteristics of effusion; duration of VT placement; frequency of VTI; and incidences of intraoperative bleeding, post-VTI infection, and post-VTI perforation; these data were collected from operation records and otoendoscopic imaging. The point of myringosclerosis development was regarded as the date of initial detection after VTI.
Study protocol
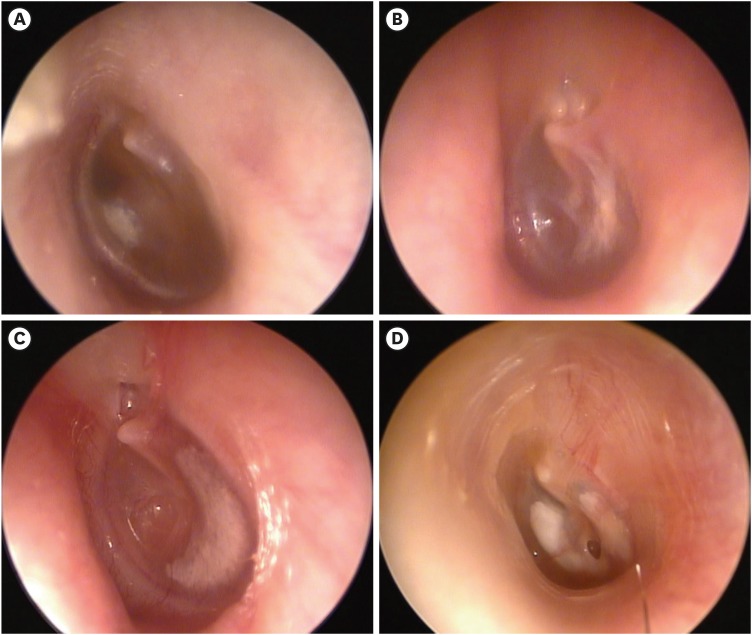
Myringosclerosis was divided into five grades according to severity: grade 0, no myringosclerosis; grade 1, myringosclerosis involving a single quadrant of the TM; grade 2, myringosclerosis involving two quadrants of the TM, regardless of the particular quadrants involved; grade 3, myringosclerosis involving three quadrants of the TM; grade 4, myringosclerosis involving all quadrants of the TM (Fig. 1).
Fig. 1
Classification of grade of myringosclerosis based on the number of involved quadrants in the tympanic membrane. (A) Grade 1: one quadrant. (B) Grade 2: two quadrants. (C) Grade 3: three quadrants. (D) Grade 4: four quadrants.
A small myringotomy was made radially on the anterior-inferior quadrant of the TM. Effusion in the middle ear was aspirated and a VT was placed into the TM. The characteristics of the effusion and presence of intraoperative bleeding were determined intraoperatively. For all patients, silicone VTs (Paparella Type; Medtronic Xomed, Minneapolis, MN, USA) were used; there were two types of VTs: type 1 had an internal diameter of 1.14 mm and type 2 had an internal diameter of 1.52 mm. The duration of effusion was defined as the time from initial detection of middle ear effusion to the time of surgery; duration of VT placement was defined from VTI to the extrusion of the VT from the TM whether the myringosclerosis was formed before or after tube extrusion. If the perforation of the TM continued for more than 3 months after removal of the tube, it was regarded as post-VTI perforation.
Statistical analysis
Statistical analysis was performed using SPSS for Windows, version 22 (SPSS Inc., Chicago, IL, USA). Independent t-tests were used for comparisons of age, frequency of VTI, duration of effusion, and duration of VT placement between the MS+ and MS− groups. The chi-squared test was used for comparisons between the two groups with regard to gender, characteristics of effusion, tube type, post-VTI infection, intraoperative bleeding, and post-VTI perforation. In addition, 1-way analysis of variance was performed to analyze the associations between severity of myringosclerosis and potential risk factors, including the frequency of VTI, duration of OME, and duration of VT placement. Post hoc analysis was performed using Tukey's test to assess potential factors affecting the severity of myringosclerosis development. In all analyses, P < 0.05 was considered to indicate statistical significance.
RESULTS
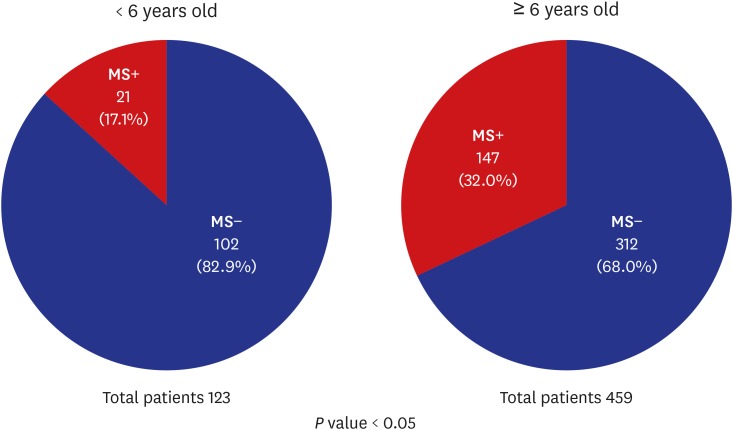
A total of 582 patients underwent VTI (men:women = 308:274). The patients ranged in age from 0 to 88 years, with a mean ± standard deviation (SD) age of 35.6 ± 27.8 years. Of these 582 patients, 168 (28.9%) had myringosclerosis (MS+ group) and 414 (71.1%) did not have myringosclerosis (MS− group). The mean ± SD age of the MS+ group was 39.84 ± 26.17 years, while that of the MS− group was 33.84 ± 28.29 years (P < 0.05) (Table 1). VTI was performed most commonly in patients 0–9 years old (190 patients, 32.65%) followed by patients 50–59 years old (90 patients, 15.46%); distinct myringosclerosis formation rates were observed in each age group (Fig. 2). Patients in this study who were < 6 years old had a lower rate of myringosclerosis formation than patients ≥ 6 years old (P < 0.05) (Fig. 3).
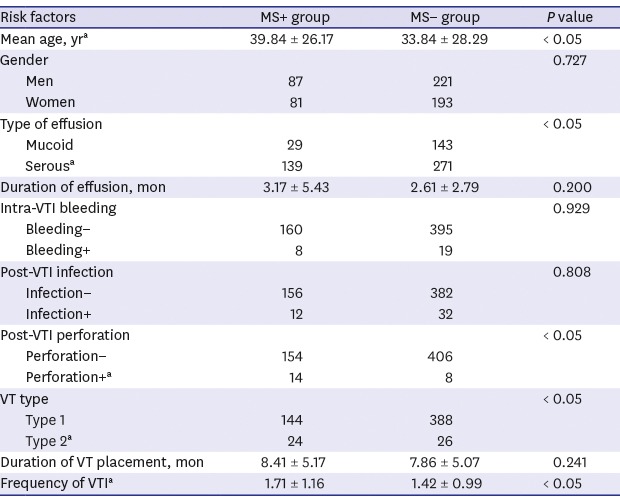
Table 1
Analysis of possible risk factors of myringosclerosis after ventilation tube insertion

Fig. 2
Myringosclerosis formation after ventilation tube insertion, stratified according to age group.
MS+ = with myringosclerosis, MS− = without myringosclerosis.

Fig. 3
Comparison of myringosclerosis formation after ventilation tube insertion, stratified according to age (threshold at 6 years old).
MS+ = with myringosclerosis, MS− = without myringosclerosis.
Myringosclerosis was observed in 87 of 308 men patients (28.25%) and in 81 of 274 women patients (29.56%); thus, there was no significant gender-related difference in the incidence of myringosclerosis. With regard to possible risk factors, serous effusion, type 2 VT, post-VTI perforation, and frequent VTIs were associated with the formation of myringosclerosis after VTI (P < 0.05). Post-VTI infection, intraoperative bleeding, duration of effusion, and duration of VT placement were not significantly related to myringosclerosis formation (Table 1). A logistic regression analysis was performed to examine the association of explanatory variables: serous effusion, type 2 VT, post-VTI perforation, and frequent VTIs, further confirming the significance of each variable in the formation of myringosclerosis (P < 0.01, P = 0.028, 0.002, 0.002 respectively).
Among the possible risk factors for myringosclerosis formation, the duration of effusion and frequency of VTI were related to the severity of myringosclerosis. The duration of effusion was longer in the grade 3 and 4 group than in the grade 0 group, while the frequency of VTI was higher in the grade 1 and 2 group than in the grade 0 group (P < 0.05) (Fig. 4).

DISCUSSION
In the present study, the rate of myringosclerosis formation after VTI was 28.9%, which was consistent with the findings of previous reports (32% and 35%).1112 VTI related to OME was most commonly performed in patients 0–9 years old, followed by patients 50–59 years old; these increased incidences may be related to dysfunction of the immature Eustachian tube and OME induced by aging of the Eustachian tube, respectively. These findings were supported by the results of previous studies regarding changes in the Eustachian tube lumen and cartilage calcification with age.1314 However, the incidence of myringosclerosis after VTI was highest among patients 20–29 years (68.2%) and lowest among patients 0–9 years (17.9%), although it was difficult to identify a clear statistical tendency due to differences in the numbers of patients in each group. According to a prior study of 126 school children who were 5–12 years old, the incidence of OME was much lower in children aged ≥ 6 years.15 The opening function of the Eustachian tube has been reported to improve significantly with age, and improvement is most common in pre-school age patients (3–7 years old).16 Thus, maturation of the structure (length) and function (active opening mechanism) of the Eustachian tube and maturation of the immune system by the age of 6 years could be associated with the observed reduction in the incidence of otitis media.17 When patients in the present study were stratified based on the age threshold of 6 years, the incidence of myringosclerosis formation after VTI was found to be higher in the group ≥ 6 years old than in the group < 6 years old. Our findings suggested that the degree of Eustachian tube maturation may be related to the formation of myringosclerosis and the occurrence of OME, although further studies are needed to confirm this hypothesis.
Various classification methods have been proposed based on histology or morphology of myringosclerosis, and most are related to the process by which myringosclerosis develops.3 Selcuk et al.3 classified myringosclerosis into three types based on the maturation of tympanosclerosis plaque: type I is characterized by fibroblasts, calcium crystals, and loose connective tissue under microscopic examination; these “pearl” tissues can be easily removed. Type II is characterized by calcification foci and large bundles of collagen, while type III is characterized by diffuse calcification and chondroblast-like cells. These histological findings show the sequence of myringosclerosis maturation. Akyildiz18 divided tympanosclerotic plaque into two types based on surgical detachment features: type 1 plaque is soft and easily removable with some calcium accumulation; in contrast, type 2 plaque is hard, white, fragile, and cannot be easily removed from peripheral tissues. However, these previously proposed classification systems require biopsy, which causes difficulty in preoperative evaluation of myringosclerosis. In the present study, we classified myringosclerosis based on severity in the TM.
The pathogenesis of myringosclerosis has not been fully elucidated. Mattsson et al.19 reported that free oxygen radicals generated by hyperoxic conditions in the middle ear resulted in the accumulation of sclerotic deposits. Karlidağ et al.20 reported that lower concentrations of antioxidants may increase the damage created by free oxygen radicals, providing an environment more favorable for the formation of myringosclerosis. Healed inflammation or scar tissue after recurrent inflammation have also been suggested as possible factors underlying the pathogenesis of myringosclerosis.821 There is no established treatment for myringosclerosis; however, some studies have demonstrated that the formation of myringosclerosis could be reduced by using antioxidants to reduce free radicals, as well as by applying topical vitamin E, N-acetylcysteine, sodium thiosulfate, and ciprofloxacin.2519222324 Erdurak et al.25 reported that VTI with radiofrequency myringotomy, instead of incisional myringotomy with a cold knife, could reduce the formation of myringosclerosis.
Chronic inflammation of the middle ear and trauma to the TM are regarded as the most important factors related to the formation of myringosclerosis; however, other factors have not been investigated in detail.9 Yaman et al.7 reported that age was not a significant factor associated with the formation of myringosclerosis, although it was identified as a risk factor for the formation of myringosclerosis in this study. Although results vary among studies, the majority of studies (including the present study) have indicated that gender is not a risk factor for myringosclerosis formation.71126 The duration of VT placement was considered to be an important factor in our study and in previous studies.711
Other risk factors have been analyzed in previous studies. Patients with a greater number of otitis episodes in the past year and those with a greater number of otorrhea episodes in the past year had higher rates of myringosclerosis after VTI.11 In addition, the anterior-inferior quadrant was identified as the highest risk quadrant for myringosclerosis formation, compared to the posterior-inferior quadrant, as a site of myringotomy.11 Yaman et al.7 reported that myringosclerosis was more likely to develop after VTI than after myringotomy alone. Koc and Uneri27 reported a higher rate of tympanosclerosis in patients with atherosclerosis, in comparison to the normal population; this result suggested that a genetic predisposition may be an additional risk factor for myringosclerosis formation. In the present study, the severity of myringosclerosis formation after VTI was related to the duration of effusion and frequency of VTI. Longer duration of effusion could result in a longer exposure time to middle ear inflammation, which may lead to more severe myringosclerosis formation.
There were some limitations in our study. Due to the retrospective nature of the study and the range of factors related to the formation of myringosclerosis, confounding factors may not have been effectively controlled, thereby reducing the impact of the findings.
This study identified the following risk factors for the formation of myringosclerosis after VTI: older age at onset, nature of middle ear effusion, post-VTI perforation, type 2 VT, and frequent VTI. A longer duration of effusion and more frequent VTI were associated with increased myringosclerosis severity. These risk factors for myringosclerosis formation may be useful in prediction of myringosclerosis before VTI, as well as in prevention after the procedure.
 XML Download
XML Download