

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Patients with lumbar spinal stenosis (LSS) present with symptoms of the lower extremities, including neurogenic intermittent claudication as a typical symptom.12 On the other hand, patients suffering from peripheral arterial disease (PAD) present with vascular claudication.3 It is important for orthopedic surgeons to differentiate between the claudication caused by these two different pathologies. Vascular claudication of PAD typically occurs after walking for a distance with resultant vascular insufficiency caused by an imbalance between muscular oxygen demand and supply.4 Resting from activity may help to relieve the symptoms. Neurogenic claudication of LSS is caused by narrowing of the spinal canal and neural foramen, which is aggravated by standing and relieved by sitting down and leaning over.5 It can be difficult to differentiate vascular and neurogenic intermittent claudication due to atypical signs and subjective symptoms. The exact diagnosis often cannot be made on clinical evidence alone, and ultimately requires imaging.6
Spine surgeons occasionally make the mistake of performing spinal surgery in patients who have vascular intermittent claudication arising from PAD and radiographically asymptomatic spinal stenosis. However, untreated PAD is progressive and increases the risk of severe vascular events. Therefore, one of the most important aspects in the evaluation of patients with PAD is the earliest possible identification of cases at greater risk of developing critical ischemia and, therefore, of losing the limb. Deep vein thrombosis and pulmonary embolism is a potentially life-threatening complication in patients undergoing elective spine surgery for LSS, and mechanical prophylaxis such as the wearing of elastic stockings is an effective preventive measure.7 However, elastic stockings may cause acute limb ischemia in patients with PAD, so perioperative screening of PAD in LSS patients becomes all the more important.8
The ankle-brachial index (ABI) is currently the most common clinical diagnostic test for PAD because it is simple, noninvasive, inexpensive, and specific. There have been several studies to evaluate the incidence of PAD in patients with LSS using ABI.910 However, its sensitivity is unreliable, especially in populations with severe calcified arteries.11 Run-off computed tomography angiography (CTA) of the lower extremities has become the method of choice for imaging of the vessels in patients with suspected PAD because it is fast, well tolerated, and allows for exact treatment planning even with low-dose protocols.1213 In a retrospective study, an ABI cutoff value of 0.99 was found to be optimal for detecting ≥ 50% stenosis and a cutoff value of 0.87 was optimal for detecting ≥ 75% stenosis using CTA as a gold standard. However, the diagnostic ability of ABI to detect PAD was impaired by the presence of diabetes.14
The aims of this study are to study the prevalence of PAD in LSS patients with symptoms of intermittent claudication, and to study the independent risk factors for PAD. We aim to specify the cases where it is necessary to perform CT angiography as a preoperative screening tool in surgery for spinal stenosis.
Go to : 
METHODS
Subjects
This study involved a retrospective analysis of subjects with radiographic evidence of LSS and symptoms of intermittent claudication, who underwent 3D CTA of the lower extremities at the orthopedics department in our institution during a three-year period from August 2013 to August 2016. Subjects with CT or magnetic resonance imaging of the lumbar spine suggesting LSS at a particular level and with Fontaine stage IIb claudication (intermittent claudication after less than 200 meters of walking), and who were therefore considered to be candidates for spinal surgery or intervention procedures, were selected for CTA examination to rule out PAD. CTA findings were graded according to five categories; normal (0% reduction in diameter), mild (1%–49% reduction in diameter), moderate (50%–74% reduction in diameter), severe (75%–99% reduction in diameter), and complete occlusion. These categories corresponded to those used in other imaging studies on PAD.1516 Subjects were identified from the picture archiving and communicating system and follow-up data were obtained. Subjects' information on gender, age, weight, height, diabetes mellitus (DM), hypertension, ischemic heart disease (IHD), cerebrovascular disease (CVD), hyperlipidemia and smoking history were obtained from hospital medical notes. Subject demographics are presented in Table 1. The five categories on CTA findings were divided into two groups; categories 1 and 2 as non-PAD group and categories 3, 4, and 5 as PAD group. More than 50% luminal narrowing was determined to be clinically significant and considered to be the threshold for treatment for PAD.
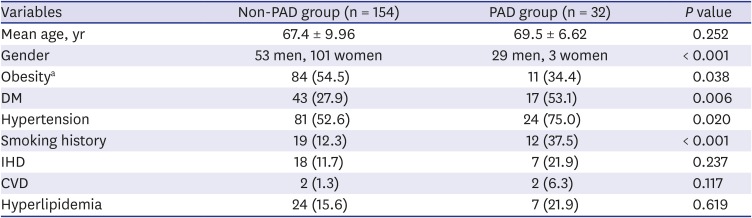
Table 1
Demographics of PAD cohort and non-PAD cohort
Values are presented as mean + standard deviation or number (%).
PAD = peripheral arterial disease, DM = diabetes mellitus, IHD = ischemic heart disease, CVD = cerebrovascular disease, BMI = body mass index.
aBMI ≥ 25.0, as defined by the Korean Society for the Study of Obesity, 2018 Guideline.
![]()
Inclusion and exclusion criteria
All subjects with 3D CTA undertaken after a visit for evaluation of claudication symptoms at our orthopedics outpatient clinic were included in the study. Intermittent claudication was defined as lower-limb cramping or pain brought on by exertion, and relieved by rest. The common symptom for inclusion was intermittent claudication after less than 200 meters walking, over a period of more than three months. Subjects with psychiatric diseases, any suspicion of spinal infection or who had already received lumbar spinal surgery were excluded from the study. Subjects at high risk for contrast media- induced nephropathy (CIN), such as those already on renal dialysis, could not be included in the study. Two hundred four consecutive subjects were recruited. Among those excluded, nine had already received spinal surgery, six had evidence of infection, and three were taking medication for psychiatric diseases. One hundred eighty-six subjects were included in the final study.
Statistical analysis
In univariate analysis, both the paired t-test and the χ2 test were used to compare each demographic parameter between the two groups. All variables found to be significant in univariable analyses were included in the conditional multivariable regression model using forward stepwise selection. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Statistical analysis was carried out using SPSS version 22.0 software (SPSS Inc., Chicago, IL, USA). A P value of < 0.05 was considered to indicate statistical significance.
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board (IRB) of the Seoul Metropolitan Government-Seoul National University Boramae Medical Center (IRB No. 20190822/30-2019-84/093). Informed consent was waived by the IRB.
Go to :
RESULTS
Thirty-two subjects were classified into the PAD group and referred to the general vascular team in our hospital, where they received appropriate treatment for PAD. Seven subjects received antiplatelet or anticoagulant therapy, while 25 subjects either received endovascular angioplasty or underwent surgical bypass. The remaining 154 subjects were classified into the non-PAD group, of which 117 underwent definitive surgery such as posterior lumbar interbody fusion for spinal stenosis and a further 37 underwent conservative treatment.
The non-PAD group had 53 men and 101 women with a mean age of 67.4 years, while the PAD group had 29 men and 3 women with a mean age of 69.5 years. The mean age was not significantly different between the two groups (Paired t-test, P = 0.252) (Table 1).
The percentage of men (90.6%) in the PAD group was significantly higher than the non-PAD group (34.4%). The prevalence of DM, hypertension and smoking history (past or present) was significantly higher in the PAD group according to χ2 test. The prevalence of obese subjects (defined as BMI ≥ 25.0) was significantly higher in the non-PAD group (P = 0.038 in χ2 test). The percentages of IHD, CVD, and hyperlipidemia were not significantly different between the two groups.
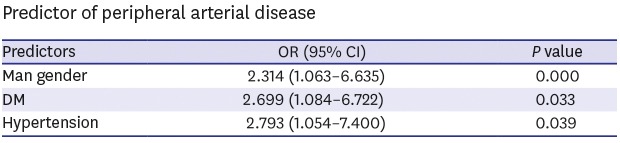
From the above results, man gender, low BMI, DM, hypertension, and smoking history were extracted as characteristics of patients with clinically significant PAD. A forward conditional multivariate regression analysis was conducted for these factors to investigate independent predictors of PAD (Table 2). Variables were entered and removed from the model based on 0.05-entry and 1.0-removal criteria. Only hypertension, DM, and man gender were found to be statistically significant predictors of PAD. Multivariate results demonstrated that hypertension (OR, 2.793; 95% CI, 1.054–7.400) was the most significant risk factor, followed by DM (OR, 2.699; 95% CI, 1.084–6.722) and man gender (OR, 2.314; 95% CI, 1.063–6.635). Of the 20 subjects that were men with both DM and hypertension, 13 (65%) were diagnosed with PAD. Of the 32 subjects in the PAD group, only three (9.3%) were free of both DM and hypertension.

Go to :
DISCUSSION
PAD is a growing problem in industrial nations because of its progressive character and the positive correlation with advanced age.17 The reported prevalence of PAD is 4.5% among men older than 55 years.18 Both LSS and PAD are usually associated with degenerative conditions and share some clinical features; therefore achieving a differential diagnosis in a clinical setting is often difficult.
Screening for PAD commonly includes foot pulses and the ABI, but concerns persist regarding their accuracy. Williams reported that diabetic neuropathy was associated with a reduced sensitivity of ABI (38%).19 The inability of ABI to detect arterial disease in the presence of detectable peripheral neuropathy resulted in false-negative results in one-third of limbs, and was even less sensitive than palpation of foot pulses. In some cases, the ankle artery is incompressible and the systolic pressure at that location cannot be measured in spite of cuff inflation at more than 250 mmHg. This situation is related to calcification of the arterial wall and may occur in patients with medical calcinosis, diabetes, and end-stage renal disease. When vascular calcification is present, stenotic disease cannot be detected by the ABI.20
When diagnosing LSS, it is important to bear in mind that concurrent PAD is possible. In a nationwide multicenter study in Japan, it was found that 6.7% of LSS patients had PAD and comorbidity of diabetes, history of cerebrovascular disorder, and history of IHD are characteristics of LSS patients with PAD.10
The purpose of this retrospective cohort study was to use CTA in subjects with stage IIb claudication and radiographic evidence of LSS to sort out subjects with concomitant PAD, and to study any relationship between the prevalence of comorbidities such as diabetes and hypertension with PAD in LSS patients. Out of 186 subjects with radiographic evidence of LSS, thirty-two were diagnosed with clinically relevant PAD (defined as > 50% luminal narrowing on CTA findings) for a calculated prevalence of 17.2%. In other countries, the prevalence of PAD (usually defined as ABI < 0.90 in either leg) in the general population is reported to be 3%–19%,2122 and several studies also demonstrated that the risk of PAD is significantly higher in older people and in men.2324 Although the diagnostic standard for the evaluation of PAD is still digital subtraction angiography, this technique has several disadvantages such as invasiveness and high cost, and is slowly being replaced by other noninvasive exams such as CT and MR angiography. The clinical utility of CTA in the evaluation of PAD has been found in a few studies.2526 Schernthaner et al.12 showed that CTA can be a viable and reliable noninvasive imaging method for the evaluation and triage of patients with stage II PAD, and that its findings are a highly accurate basis for treatment decisions and planning. In the clinical setting, it is important for surgeons to keep in mind that claudication in a patient with radiographic evidence of LSS is not always of neurogenic origin. An arterial pulse examination was deemed to be insufficient for PAD screening in lumbar stenosis patients in a prospective multicenter study,27 while the validity of ABI for the differential diagnosis of PAD and LSS was checked in one retrospective study.9 To the best of our knowledge, no previous studies have checked CT angiograms as a preoperative study in patients with LSS to rule out PAD. We have shown that routine CTA exams in certain LSS patients can be useful for preventing missed diagnosis of PAD and in guiding further treatment.
Our study has certain limitations. First, based on its retrospective design, uncertainty over missing and erroneous medical records exists, which could seriously affect our results. Second, subjects at high risk for CIN could not undergo CTA and were therefore excluded from the study. CIN, defined as a relative increase of serum creatinine levels of at least 25% over the baseline value, occurs at a rate of 1%–6% in unselected patient populations and up to 40%–50% in high-risk patient populations such as those with preexisting renal insufficiency.28 This selection bias could have affected the results of our study because patients with renal sufficiency could also be at high risk of PAD. Third, ABI was not measured in all subjects. Further studies should try to elucidate whether ABI scores are correlated with PAD severity in CT angiography. Other variables such as osteoarthritic pain, neuropathic pain and psychosocial factors should also have been taken into consideration as they may have affected subjects' symptoms. Intermittent claudication symptoms as told by the patient may be confused with arthritic symptoms in the hip, knee, or ankle and peripheral neuropathy associated with diabetes.
The current study showed that man gender, DM and hypertension were the greatest risk factors for PAD. We conclude that man patients with diabetes and/or hypertension should be put under serious consideration for routine CT angiography examination when under evaluation for LSS and intermittent claudication. 3D CTA has the added advantage of guiding therapeutic strategies as high-image resolution techniques allow for better evaluation of the entire vascular tree in the lower extremities. The disadvantages are the need for radiation exposure to the patient and the usage of potentially nephrotoxic contrast material. Patients under risk for contrast-induced nephropathy should carefully be screened out before the examination takes place. Reports on treatment results and follow-up examinations should be studied in future reports to determine how accurate CTA is in guiding decisions for management of intermittent claudication.
Go to :
 XML Download
XML Download