

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ruptured intracranial aneurysms usually results in subarachnoid hemorrhage (SAH) and intracranial hematoma, which often leads to death or neurological dysfunction.1 Although great progress has been made in craniotomy,2 endovascular interventional embolization for intracranial aneurysms has become widespread because of its minimally invasive characteristics. However, there are still some complications associated with interventional embolization that lead to permanent defects or death, including thrombo-embolic events, intraprocedural and postprocedural aneurysmal rerupture, vasospasm, parent artery obstruction, collapsed coils, coil and/or stent migration, coil malposition and so on. Among them, intraprocedural rerupture (IPR) of intracranial aneurysms during embolization is one of the most common, most dangerous and inevitable complications, because of the difficulties in hematoma and/or SAH elimination, the subsequent malignant cerebral edema and intracranial hypertension, as well as the limitation of salvage therapy for IPR. Previous studies demonstrated that the incidence of IPR in patients with ruptured cerebral aneurysms was about 1.4%–7.7%.345 Despite the factors affecting IPR have been sporadically reported,5678 most previous researches investigated the risk factors for IPR in patients with unruptured aneurysms,67 or by merging both ruptured and unruptured aneurysms.8 The factors increasing the risk of IPR occurrence in patients with ruptured aneurysms are still controversial. Because of the differences in clinical characteristics between ruptured and unruptured intracranial aneurysms, the treatment and management strategies differ between patients with ruptured and unruptured aneurysms. Thus, study to accurately assess risk factors leading to IPR in ruptured aneurysms patients is needed. The present research was designed to investigate the risk factors for IPR in patients with ruptured cerebral aneurysms.
Go to : 
METHODS
Patients
This was a retrospective single-center study. A total of 1494 patients with ruptured intracranial aneurysms who underwent endovascular interventional embolization between January 2010 and December 2019 at the department of neurosurgery in our hospital were included in the study. The criteria for inclusion were as follows: SAH confirmed by head computed tomography or magnetic resonance imaging and if necessary by lumbar puncture, ruptured intracranial aneurysms confirmed by computed tomography angiography (CTA) or digital subtraction angiography (DSA), receipt of endovascular interventional embolization. The patients excluded from this study were those with cerebral arteriovenous malformations, intracranial vascular abnormalities and coagulation dysfunction. According to whether IPR had occurred, patients enrolled in this study were categorized into IPR and non-IPR groups.
Endovascular procedure
All endovascular treatments and evaluations were performed by one of two proficient endovascular neurosurgeons each with more than 10 years of experience. One neurosurgeons performed 735 cases and the other performed 759 cases. There was no significant individual difference between them. All patients underwent the endovascular procedures under general anesthesia within 5 days after the onset of SAH. After the right or left femoral artery was successfully punctured and cathetered by Seldinger's technique, 5,000 U heparin was intravenously administered, and followed by intravenous infusion of 1,000 U per hour to maintain the activated clotting time at twice the normal level throughout the process. Angiography was performed to determine the best working angle, and the most appropriate microcatheter and microwire were selected for each patient according to the characteristics of aneurysms. After the microcatheter was placed in the appropriate position, the micro-coils were used to tamponade aneurysms. The stents and balloons were selected on a case-by-case basis.
For patients with cerebral vasospasm after SAH, nimodipine was infused intra-arterially before coiling and continued throughout the procedure at a rate of 1–2 mg per hour. The dosage of nimodipine was adjusted according to blood pressure to ensure that the decrease of systolic blood pressure did not exceed 15 mmHg. Acute treatments of vasospasm also included nitroglycerin and/or verapamil. Once an IPR occurs, delivery of coils was continued, and the packing was completed as rapidly as possible. Heparin was stopped immediately and reversed with protamine. Craniotomy and/or external ventricular drainage were performed if necessary. For patients with poor clinical condition, mild therapeutic hypothermia was adopted if needed.9
Data collection
The following information was collected for all enrolled patients: 1) baseline characteristics, including age, gender, past medical history, as well as clinical condition before and after coil embolization; 2) characteristics of aneurysms: location, multiple aneurysms, aneurysm size, aneurysm shape, wide neck; 3) treatment related factors: time from symptom onset to intervention, treatment modality, cerebral vasospasm during aneurysm embolization.
Clinical condition before coil embolization was assessed according to preoperative Hunt and Hess Grade, which was dichotomized into good clinical condition (Hunt and Hess Grade I–III) and poor clinical condition (Hunt and Hess Grade IV–V). Clinical condition after coil embolization was assessed according to Glasgow Outcome Scale (GOS) at discharge, which was dichotomized into good outcome (GOS 4 or 5) and poor outcome (GOS 1–3). IPR was highly suspected based on clinical symptoms, such as a sudden increase in blood pressure and/or a sudden decrease in heart rate, and even pupil dilatation. It was diagnosed when extravasation of contrast material, microguidewire or microcatheter perforation, and the protruding of coils from the confines of the aneurysm wall were visualized on DSA. Aneurysm size was measured by the senior neurointerventional surgeons on the basis of precise measurements made on three-dimensional angiography, defined as the largest diameter from the neck to the dome of the cavity at the optimal projectile angle. Wide-neck aneurysm was defined as an absolute neck width ≥ 4 mm or a dome to neck ratio ≤ 2. Irregular morphology of aneurysm was defined as the presence of small bleb(s) or daughter or secondary aneurysm(s) protruding from the aneurysm fundus, or other irregular shapes, such as bilobed or multilobed structure.10 Cerebral vasospasm after SAH was defined using both clinical and radiological criteria.11 Objective imaging methods, such as transcranial doppler, CTA and DSA, were used to diagnose intracranial atherosclerosis. Intracranial atherosclerosis was diagnosed as varying degrees of luminal stenotic lesions involving intracranial arteries, (including anterior cerebral artery, middle cerebral artery, posterior cerebral artery, intracranial vertebral artery, basilar artery and intracranial internal carotid artery [ICA]), and accompanied by dyslipidemia, especially elevated low-density lipoprotein cholesterol (> 3.64 mmol/L). In addition, elevated high sensitivity C-reactive protein, homocysteine and lipoprotein (a) could be used as an auxiliary index for the diagnosis of intracranial atherosclerosis. Intracranial stenosis was defined as a localized narrowing of the lumen by 50% or more that can affect the parent arteries.12 ICA atherosclerosis was defined as present when the ICA stenosis was more than 30%, and categorized into 3 grades according to the degree of stenosis: mild (< 50%), moderate (50%–70%), and severe (> 70%).
Statistical analysis
All statistical analyses were performed using SPSS 20.0 for Windows (SPSS Inc, Chicago, IL, USA). Continuous variables were expressed as the mean ± standard deviation, and categorical variables were expressed as frequencies (%). The differences between two groups were tested with t-test for continuous variables, and χ2 test for categorical variables. Fisher's exact test was performed if sample size was too small. Univariate analysis and multivariate logistic regression analysis was performed to identify the risk factors for IPR in patients with ruptured aneurysms. The receiver operating characteristic (ROC) analysis was performed to determine the cutoff values (with the highest sum of specificity and sensitivity) of continuous variables for IPR during coil embolization. A value of P < 0.05 was considered to indicate statistical significance.
Ethics statement
This study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The research protocol was approved by the Medical Ethics Board of the Renmin Hospital of Wuhan University (approval No. WDRM201912-036). Informed consent was obtained from all patients enrolled in this study or their next of kin.
Go to :
RESULTS
Baseline characteristics of the patients
A total of 1,494 patients with ruptured intracranial aneurysms were recruited in this study: 658 men and 836 women, with an average age of 51.7 ± 12.0 years (ranging from 23 to 77 years), and the aneurysm size ranged from 1.2 to 38.3 mm, with an average size of 7.4 ± 4.8 mm. The patients’ descriptive statistics were listed in Table 1. There was no significant difference in age, gender, past medical history, clinical condition before coil embolization, characteristics of aneurysms except for the size and shape of intracranial aneurysms, and the treatment strategies between the two groups. Compared to non-IPR group, the IPR group scored significantly higher on the rate of poor outcome, cerebral atherosclerosis, aneurysms with irregular morphology and vasospasm during embolization. The mean size of aneurysms in IPR group was significantly smaller than that in non-IPR group. The time from symptom onset to intervention was significantly shorter in non-IPR group.
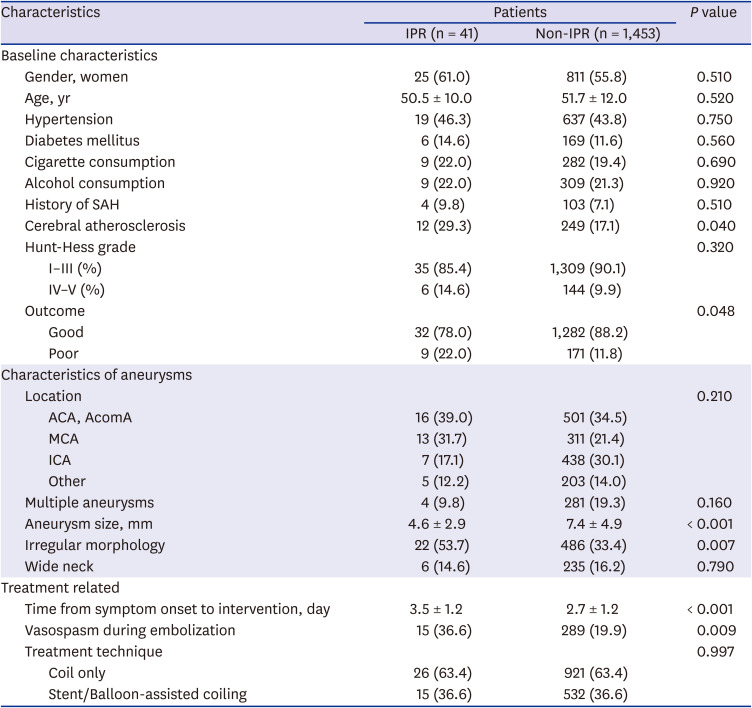
Table 1
The clinical characteristics of patients with ruptured intracranial aneurysms
Data area presented as number (%) or mean ± standard deviation.
ACA = anterior cerebral artery, AcomA = anterior communicating artery, ICA = internal carotid artery, IPR = intraprocedural rerupture, MCA = middle cerebral artery, SAH = subarachnoid hemorrhage.
![]()
Clinical features of IPR
There were 41 cases suffered from IPR, showing that the incidence rate was 2.7%. The aneurysms in patients with IPR were mainly located in the distal segments of the main branches of the ICA. Totally, 15 patients of IPR (36.6%) presented with cerebral vasospasm during embolization. Among them, 12 cases presented with cerebral vasospasm caused by SAH before endovascular treatment, and 3 patients suffered from cerebral vasospasm caused by stimulation of arterial wall induced by microguidewire and/or microcatheter in the process of conveying. The clinical features of patients with IPR were summarized in Table 2.
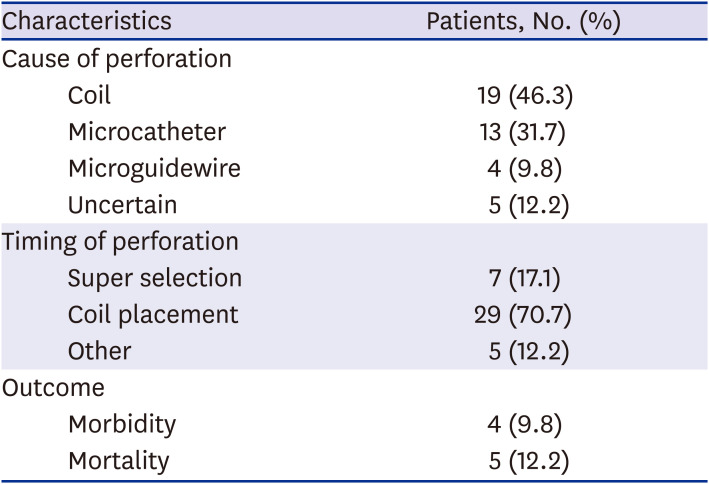
Table 2
Characteristics of patients with intraprocedural rerupture
![]()
The timing of IPR was as follows: 29 occurred during coil placement, 7 during super selection, and 5 during the other processes, such as angiography. Of the 36 patients with IPR during coiling or microcatheter positioning, there were 7 cases of berry aneurysm (19.4%), and 23 cases of small aneurysm (63.9%). Among the 19 aneurysms with IPR induced by coils, 8 ruptures occurred in the framing stage, 5 occurred in the filling stage, and 6 occurred in the finishing stage. IPR occurred in the dome of aneurysms in 8 patients, of which 5 happened in the framing stage and 3 in the filling stage; IPR happened in aneurysm wall in 2 cases, 1 of which occurred during the framing stage and 1 during the filling stage; IPR occurred in the neck of aneurysms in 4 cases, all of which happened in the finishing stage. The other 5 patients lacked detailed information regarding the site of IPR. After immediate salvage treatment, 32 patients survived without neurological impairment, 5 patients died of extensive SAH, and 4 patients suffered from different neurological deficits: 1 patient suffer from persistent vegetative state, 1 presented with global aphasia, 1 with numbness and weakness in the left arm and 1 with a severe right paralysis and slurring of speech. The mortality and disability rates of IPR were 12.2% and 9.8%, respectively.
Risk factors for IPR in patients with ruptured aneurysms
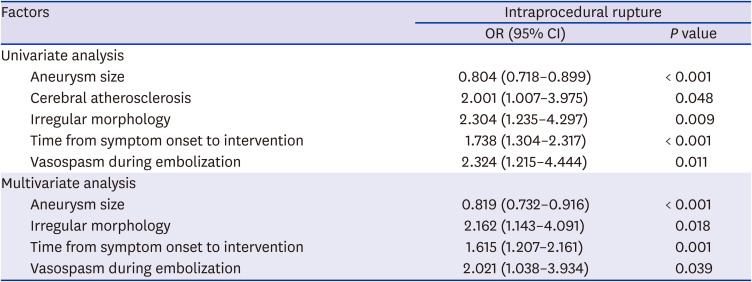
Five factors identified by univariate analysis were further analyzed by multivariate logistic regression model and 4 risk factors for IPR were identified, including aneurysm size, aneurysms with irregular morphology, time from symptom onset to intervention and vasospasm during embolization (Table 3). The ROC curve analysis indicated that the area under the curve (AUC) for aneurysm size was 0.697 (95% confidence interval [CI], 0.616–0.778; P < 0.001). By applying the cutoff value of 3.4 mm, the sensitivity and specificity of the aneurysm size in predicting IPR in patients with ruptured aneurysms were obtained as 78.8% and 53.7%, respectively (Fig. 1A). The AUC for the time from symptom onset to intervention was 0.659 (95% CI, 0.577–0.741; P = 0.001); the cutoff value of the time from symptom onset to intervention was 2 days, with a sensitivity of 78.0% and a specificity of 45.2% (Fig. 1B).
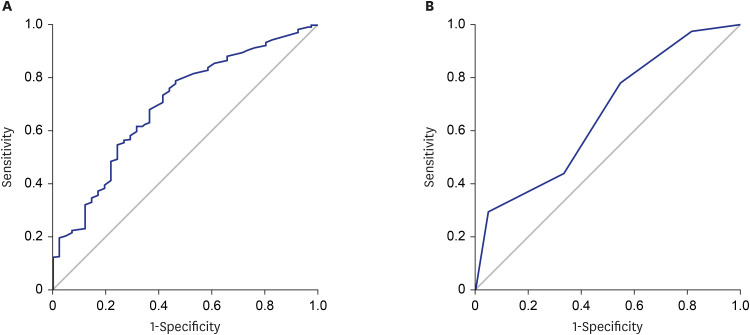 | Fig. 1The ROC curves for aneurysm size and time from onset to intervention. (A) The cutoff level of the aneurysm size for IPR. The cutoff level of 3.4 mm shows a sensitivity of 78.8% and a specificity of 53.7%. The AUC is 0.697. (B) The cutoff value of the time from onset to intervention for IPR. The cutoff level of 2 days shows a sensitivity of 78.0% and a specificity of 45.2%. The AUC is 0.659.ROC = receiver operating characteristic, IPR = intraprocedural rerupture, AUC = area under the curve.
|
Table 3
Logistic regression analysis of risk factors for intraprocedural rupture
![]()
Go to :
DISCUSSION
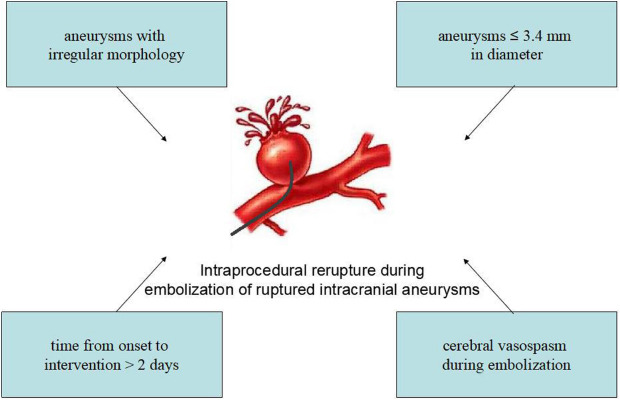
IPR in patients with ruptured intracranial aneurysms during coil embolization is devastating and can lead to serious clinical consequences such as periprocedural neurological deficits and death. A better understanding and preoperative systemic evaluation of risk factors for IPR may be conducive to the prevention of IPR and the improvement of the prognosis of patients. However, little comprehensive research has been performed to investigate the risk factors for IPR in patients suffering from aneurysmal SAH. This study aimed at evaluating IPR, while especially focusing on the risk factors for IPR among patients with ruptured aneurysms during coil embolization. As shown in the results, the prevalence rate of IPR was 2.7%, which is in line with previous studies.345 Our results also clearly indicated that aneurysms ≤ 3.4 mm in diameter, aneurysms with irregular morphology, time from symptom onset to intervention > 2 days as well as cerebral vasospasm during embolization appeared to be independent risk factors for IPR in patients with ruptured aneurysms.
As is known to all, atherosclerosis is one of the factors contributing to the formation of intracranial aneurysms.1314 Nevertheless, previous research demonstrated that cerebral atherosclerosis is a protective factor against rupture.15 The role of atherosclerosis in patients suffering from IPR is still under debate. Our results demonstrated that cerebral atherosclerosis was not an independent risk factor for IPR. To analyze reasons for the different conclusions, one reason may be that not all patients with severe intracranial atherosclerosis were included in this study because some of them underwent craniotomy for aneurysm clipping instead of interventional embolization. Further studies should be conducted to confirm this conclusion.
Recent studies have shown that small aneurysm size was significantly associated with the occurrence of IPR in patients with ruptured and unruptured cerebral aneurysms.71617 A similar conclusion can be drawn from our research. In this study, we found that aneurysm size, which was one of the independent risk factors for IPR in patients with ruptured aneurysms, had an OR value that was less than 1, suggesting that the smaller the aneurysm size, the greater the risk of IPR in patients with aneurysmal SAH. Mitchell et al. found that aneurysm size ≤ 4 mm was a risk factor for IPR in ruptured aneurysms.16 However, some researchers have found that aneurysms less than 3 mm in diameter increased the risk of IPR.418 The reason for this difference may be that the critical point of aneurysm size is artificially classified, which has a certain impact on the accuracy of the conclusion. To avoid this kind of defect, we used ROC curves and AUC analysis to determine the cutoff value of aneurysm size for IPR in ruptured aneurysms patients. In predicting the occurrence of IPR, we found that the cutoff value of aneurysm size was 3.4 mm, suggesting that IPR is more likely to occur in patients with ruptured aneurysms no more than 3.4 mm in diameter.
Irregular morphology of aneurysm has been widely recognized as a risk factor for rupture.1920 However, the relationship between IPR and the shape of aneurysm is still controversial. Li et al. found that irregular morphology was an independent predictor of IPR in patients with unruptured cerebral aneurysms.6 It is possible that aneurysms with irregular morphology may have weak arterial walls and are more likely to rupture. However, in another study by Kawabata et al.,7 no relationship was found between irregular morphology of aneurysm and IPR. A similar conclusion was obtained by Zhang et al.4 for patients with ruptured intracranial aneurysms; they found that the morphological features of aneurysms were not concerned with IPR. Our results clearly indicated that irregular morphology was an independent risk factor for IPR. Conflicting conclusions may be drawn partly because some researchers did not include the morphology of aneurysms as a parameter in their studies.7
In this study, we also found that time from symptom onset to intervention > 2 days was one of the risk factors for IPR in patients with aneurysmal SAH, which is different from the findings of a previous study in unruptured aneurysms. The reason for this may be as follows: 1) With time, the fibrinolysis of the fibrin clot surrounding the site of aneurysm rupture makes IPR more likely to occur. 2) The patients received a series of treatments to reduce intracranial pressure before embolization, which led to the increase of transmural pressure of aneurysms and increased the risk of IPR.
With regard to the relationship between vasospasm and IPR, there was a conspicuous correlation shown in our study, which is in line with previous researches.3 Cerebral vasospasm often occurs in the acute phase of aneurysmal SAH, and can be caused by hemodynamic fluctuations or stimulation of arterial wall induced by microguidewire and/or microcatheter in the process of conveying, which makes it harder for neuro-interventionologists to deliver the microcatheter and microguidewire, and complete embolization of intracranial aneurysms. This restricted access makes interventionists to choose a suitable size of microcatheter or microwire with smaller diameter, which is flexible and prone to bend and twist when crossed the tortuous or spastic vessels. In this case, the tip of a circuitous microcatheter or microwire can easily jump forward in an uncontrolled manner, leading to rupture of an aneurysm. To minimize the risk of neurological injury and maximize the outcomes from IPR, a potential protocol could be described briefly as follows: First, intra-arterial infusion of nimodipine should continue throughout the procedure. Second, choose the most appropriate microwire or microcatheter according to the patient's condition. Third, interventionists should make efforts to deliver the microcatheter or guidewire as gently and smoothly as possible.
The limitations of this study are as follows: First, the number of patients with IPR is relatively small in this single-center retrospective clinical study, which may result in a certain degree of statistical bias, so the multicenter large sample study is desired to establish. Second, in our hospital, not all patients with ruptured aneurysms are treated with endovascular interventional embolization. Therefore, some factors, which may be responsible for IPR in patients with ruptured aneurysms, have not been systematically included and assessed. Finally, the influence of interventional technique on IPR should not be neglected, but there is no suitable way to measure it.
In conclusion, the present study identified some important factors associated with the incidence of IPR in patients with ruptured cerebral aneurysms, suggesting that aneurysms with irregular morphology, aneurysms ≤ 3.4 mm in diameter, time from onset to intervention > 2 days and cerebral vasospasm during embolization were independent risk factors for IPR in patients with aneurysmal SAH. Neurointerventional surgeons should pay enough attention to the factors that may increase the risk of IPR for patients with ruptured aneurysms so as to minimize the occurrence of this complication.
Go to :
 XML Download
XML Download