

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19), which began at the end of 2019, has spread worldwide since March 2020, threatening the health and life of many people and amplifying social and economic risks. Fear has been increasing given that COVID-19 spreads faster than the swine flu and has a higher fatality rate, and anxiety about infection has been increasing given that there is no cure yet.12 As an infectious disease disaster continues, serious psychological and social stress may occur.34 According to a recent survey conducted in Korea about COVID-19, about 20% of the citizens were at moderate or high risk for anxiety and depression that required attention.5 With the added stress of fear of getting infected with COVID-19, they may become more vulnerable. New infectious diseases such as COVID-19 are not just a challenge for the health and the medical fields but also a crisis for the whole country, creating enormous psychological and social losses. Therefore, management of the mental and psychological impact must also be paid attention to.678
In the case of new risks such as infectious diseases, the general public tends to obtain information through external channels, such as print and TV media, as well as social media, especially when they do not have any or much knowledge of specific risks associated with them.9 For highly infectious diseases about which very little is known, people actively use and become highly dependent on media to resolve the uncertainty caused by the lack of information. Although media reports on diseases may have positive effects on promoting healthy behaviors and may reduce anxiety by increasing general public knowledge on the disease and improving coping management strategies, it can also have negative effects of spreading unfounded fears and anxiety through unconfirmed articles, exaggerated reporting, and use of sensational language.101112
The primary dissemination of knowledge is through the media (e.g., print, TV media, and social media). Therefore, it is the media that determines people's overall attitudes, risk control, risk perception, and behavior towards infected people.1314 According to the media usage survey results related to H1N1, the usefulness of acquiring H1N1 related information was found to be high, but the reliability and accuracy of the information were found to be low. Also, it was felt highly likely that incorrect information and knowledge could lead to distorted perceptions and actions.10 It has been reported that the misconceptions regarding the disease and behavior based on these misconceptions leads to a negative perception of infected people and leads to stigma or prejudice against them. Similar results regarding the advantages and disadvantages of media were found in subsequent studies related to Middle East Respiratory Syndrome.1516 Due to the nationwide spread of COVID-19, public anxiety and fear are becoming more prevalent, and inaccurate information accessed through various media further adds to the public anxiety. Considering this situation, it is necessary to examine the overall relationship among people's level of knowledge about COVID-19, fear of infection, prejudice towards infected people, and anxiety, as a result of the general public's use of media related to COVID-19.
While the diagnosis, tracking, monitoring, and quarantine measures for COVID-19 are being established in many countries, epidemiological studies on disease-related media use and the resulting psychosocial effects are lacking. Therefore, this study aimed to examine how the COVID-19 related use of media by the general public affects anxiety. Specifically, the use of media for COVID-19 was presumed to affect the knowledge of the disease, and it was assumed that this effect was connected to the prejudice toward the infected people and the fear of infection, ultimately increasing public anxiety. The research hypotheses of our study were as follows. 1) Exposure to COVID-19-related news via mass media may increase the fear of infection, general anxiety, and prejudice towards infected people. 2) The use of mass media will enhance our knowledge about COVID-19. 3) The public's knowledge about COVID-19 will reduce the fear of infection, general anxiety, and prejudice towards infected people. 4) Prejudice towards infected people and the fear of infection will have mediating effects of media usage related to COVID-19 and the COVID-19 knowledge level on anxiety. We believe that our study can contribute to developing social strategies to reduce anxiety related to the COVID-19 pandemic.
Go to : 
METHODS
Study design and participants
This was an online-based study that was part of studies on the psychosocial effects of COVID-19 in the general population and people with mental health problems. Details of the data collection method were described previously.17 Briefly, between April 24 and May 5 of 2020, the third month of the COVID-19 outbreak in Korea, we conducted an anonymous online survey with 1,500 residents aged 19–65 years from the Seoul metropolitan area (Seoul and Gyeonggi Province around Seoul, n = 500), Daegu (n = 500), and Gwangju (n = 500). All participants were selected from among the panels of an online survey service provider (EMBRAIN PUBLIC) using a proportional stratified sampling method.
Research tools
COVID-19 related media use
For COVID-19 related media use, a questionnaire about the use of news for information gathering was created. The questionnaire consisted of two questions, “I have more time to watch the news than before.” and “I frequently check the news related to COVID-19.” Their answers were evaluated based on a 5-point Likert scale. The higher the score, the higher the level of media usage. The reliability of the questionnaire was Cronbach's α = 0.736.
Knowledge about COVID-19
In accordance with guidelines by the Central Disease Control Headquarters, we constructed a questionnaire to investigate knowledge of transmission and prevention of COVID-19. The questionnaire consisted of a total of six items, including three true statements and three false statements (Table 1). A score of 0 was given for incorrect and unknown answers, and 1 point was given for correct answers. The higher the score, the higher the level of knowledge. The reliability of these items was Cronbach's α = 0.704.
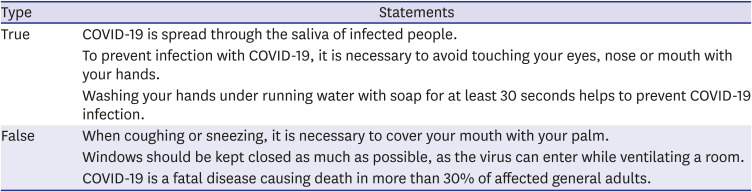
Table 1
Questionnaire to investigate knowledge of COVID-19
![]()
Fear of COVID-19 infection
Among the questionnaires that we developed in our previous study to investigate the psychosocial experiences and distress associated with COVID-19,17 we selected the factor of ‘fear of COVID-19 infection' for this study. The questionnaire comprised seven items that were modified from a previous study18 regarding the severe acute respiratory syndrome infection and were created based on clinical experience. All items on the questionnaire were rated using a 5-point Likert scale, from “Not at all (1 point)” to “Very much (5 points)”. The higher the score, the greater the fear of infection. The reliability of these items was Cronbach's α = 0.876.
Prejudice towards people infected with COVID-19
This factor was composed of three items from the stigma scale related to the swine flu outbreak10 and modified for COVID-19. The questionnaire consisted of 3 questions that were evaluated based on a 5-point Likert scale. The higher the score, the higher the level of prejudice against the infected person. The reliability of the items was Cronbach's α = 0.711.
Anxiety
This study used the Korean version of the Generalized Anxiety Disorder Scale (GAD-7) developed by Spitzer et al.19 and translated by the National Mental Health Center in Korea to assess the anxiety status of users of primary health care centers. The GAD-7 consisted of a total of 7 questions, and every question was evaluated based on a 4-point Likert scale, from “not disturbed at all (0 points)” to “be disturbed almost every day (3 points).” Out of the highest possible score, 21 points, a score of 0-4 points was classified as normal, whereas scores of 5 points or higher were classified as anxious. The higher the score, the higher the level of anxiety. The reliability of the items was Cronbach's α = 0.926.
Statistical analysis
For data analysis, this study used SPSS 20.0 and AMOS 20.0 (SPSS Inc., Chicago, IL, USA). Cronbach's α was calculated to measure the reliability of the questionnaires and frequency analysis, mean, standard deviation, and normality tests were performed. To conduct the structural equation model analysis and evaluate the goodness of fit of the model, χ2, comparative fit index (CFI), Tucker Lewis index (TLI), and root mean square error of approximation (RMSEA) were used.
Ethics statement
The study was approved by the Chonnam National University Hospital Institutional Review Board (CNUH-2020-092). Electronic informed consent was obtained from each participant prior to starting the investigation.
Go to :
RESULTS
Sociodemographic characteristics of the study subjects
Table 2 shows the sociological and demographic characteristics of the study subjects.
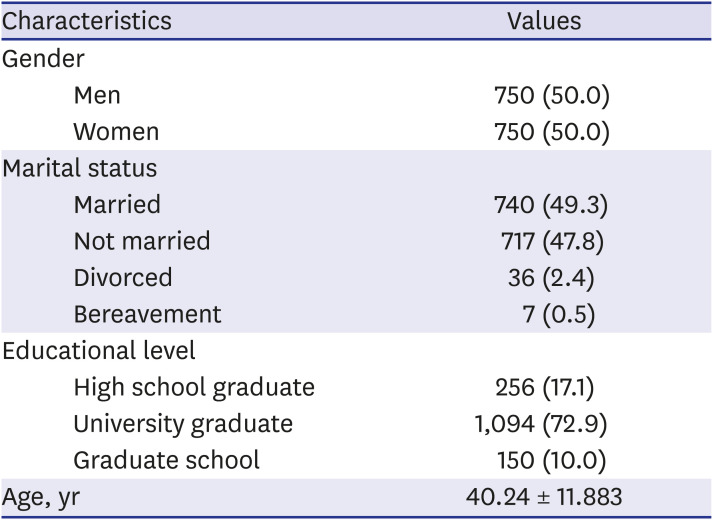
Table 2
Sociodemographic characteristics of participants (n = 1,500)
![]()
Descriptive statistics of measurement variables
In order to conduct the structural equation model analysis, the measurement variables must be normally distributed. Given the normal distribution (skewness < 2, kurtosis < 7) in the structural equation model,20 the skewness and kurtosis of the variables used in this study met the conditions required to apply the structural equation model (Table 3).
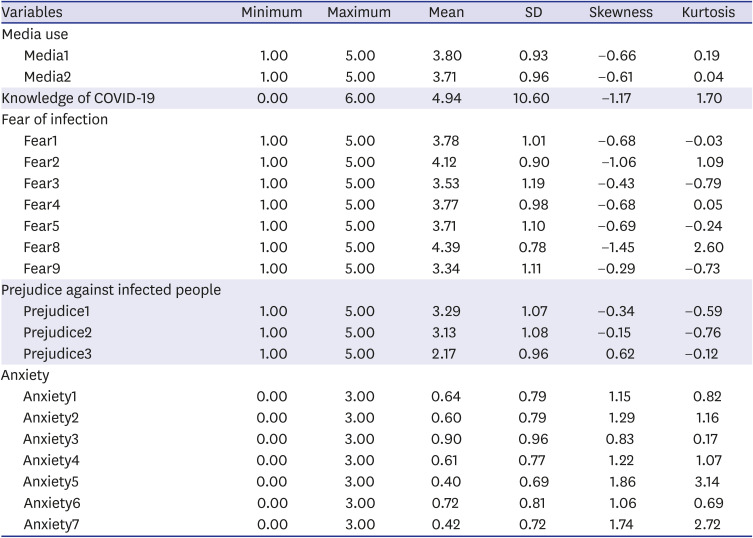
Table 3
Descriptive statistics of variables
![]()
Testing the research model
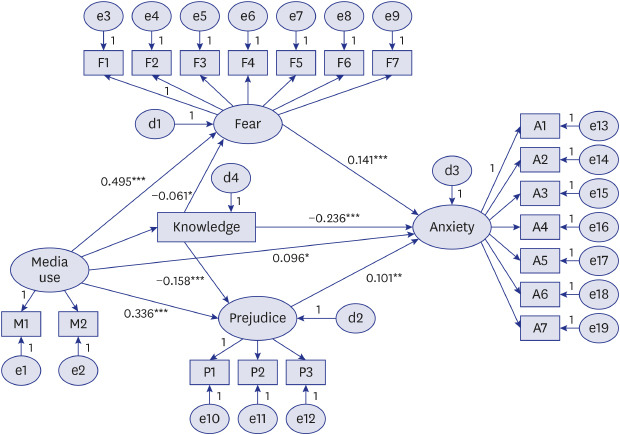
This study tested the goodness of fit of the model using CFI, TLI, and RMSEA, which are not sensitive to sample size and have proven evaluation standards based on the principle of parsimony.21 The goodness of fit of the model was found to be satisfactory for all fit indices except χ2 (Fig. 1 and Table 4).
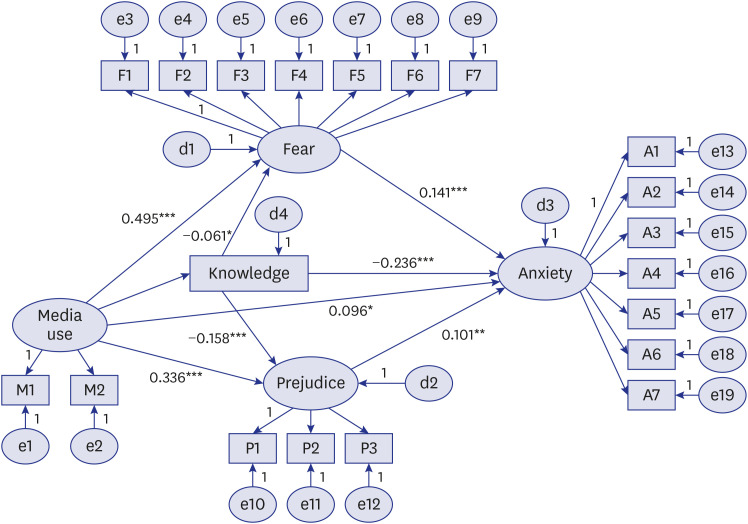

The effects of media use on fear of infection (t = 14.156, P < 0.001), prejudice against infected people (t = 8.854, P < 0.001), and anxiety (t = 2.471, P < 0.05) were significant. Knowledge about COVID-19 had significant protective effects on fear of infection (t = −2.390, P < 0.05), prejudice against infected people (t = −5.284, P < 0.001), and anxiety (t = −9.014, P < 0.001). However, the effect of media use on knowledge about COVID-19 was not statistically significant (Table 5).
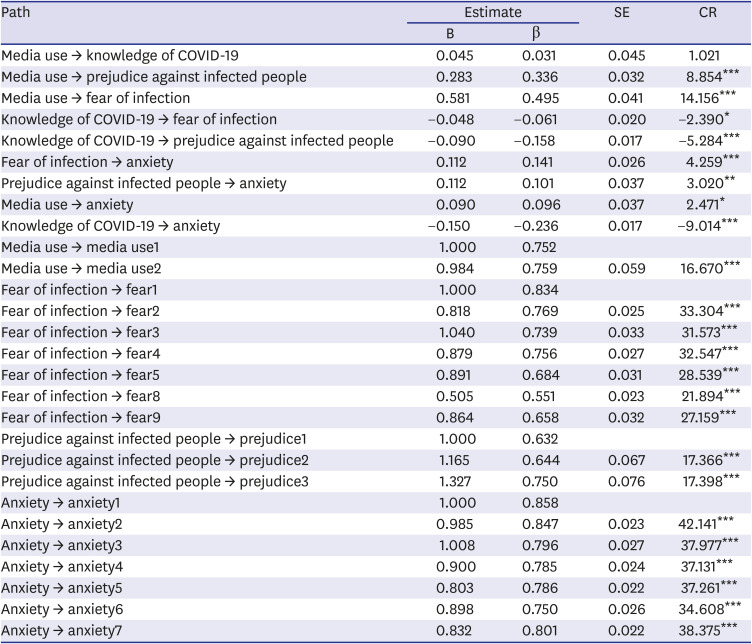
Table 5
Estimates of study model
B = unstandardized estimate, β = standardized estimate, SE = standard error, CR = critical ratio.
*P < 0.05; **P < 0.01; ***P < 0.001.
![]()
Testing the mediation effect
To test the mediation effect, analysis was performed using the bootstrapping method. First, in the pathway of COVID-19 knowledge–prejudice against infected person-anxiety, the partial mediation effect of prejudice against infected people was found to be significant (β = −0.270, P = 0.002). Second, in the pathway of media use-prejudice against infected people-anxiety, the partial mediation effect of prejudice against infected people was found to be significant (β = 0.050, P = 0.002). Third, in the pathway of media use-fear of infection-anxiety, the partial mediation effect of fear of infection was found to be significant (β = 0.088, P = 0.002) (Table 6).
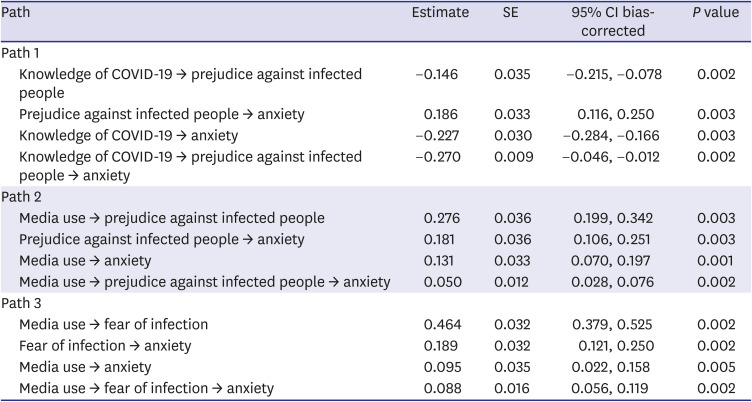
Table 6
Analysis of mediating effects
![]()
Go to :
DISCUSSION
Using the structural equation model, this study analyzes the effect of the general public's use of COVID-19-related media and the level of knowledge on anxiety, and the mediating effect of fear of infection and prejudice against infected people in these causal relationships. Through this analysis, the study attempted to expand the importance of media influence on infectious diseases and provide basic data for psychological countermeasures against COVID-19. The research findings of the direct effect on the structural relationship between the major variables used in this research model are as follows.
While media use was found to have significant effects on fear of infection, prejudice against infected people, and anxiety, it did not improve knowledge about COVID-19 (research hypothesis 1: supported; research hypothesis 2: rejected). These outcomes are contrary to previous research findings that disease information obtained through the media increases disease knowledge.162223 Through this study, it was confirmed that the use of media did not affect the formation of correct knowledge, but rather may reinforce the fear of infection and social stigma towards infected people. This supports a prior study that argued that there is confusion and fear among the public at the time of the outbreak of an infectious disease and the demand for information from the media is strong, but the accuracy and reliability of the information disseminated thus is unclear and may or may not be useful for knowledge formation.101124 It can be said that this is a result that suggests the negative effect of using the media since it can spread fear and anxiety about diseases with exaggerated reports and unverified articles.
Moreover, it was confirmed that knowledge about COVID-19 had a significant effect on fear of infection, prejudice against infected people, and anxiety (research hypothesis 3: supported). Since media is the most utilized source of information, and an intermediary playing an important role in the transformation of a general risk into an individual risk,925 it is important to not only prepare a manual to respond to infectious diseases but also to deliver accurate knowledge about infectious diseases. In addition, the media must strive to deliver correct information, avoid interest-oriented reporting, and comply with disaster reporting rules. To make people more objectively aware of the risk of infectious diseases through media in the event of an infectious disaster such as COVID-19, a persuasive strategy must be used and information with proven reliability must be delivered so that the meaning of risk perception can be understood from various angles.
Furthermore, it was confirmed through the results of this study that the use of media in an infectious disaster situation could affect the increase of anxiety, so it should be recognized that disaster prevention and recovery are also among the roles of the media. Official announcements by authorities or institutions should also be verified as much as possible for their authenticity and accuracy, and public anxiety should be corrected by strengthening the social responsibility of the media.
Following are the results related to the mediating effect of the fear of infection and the prejudice against the infected person in the causal relationship between the use of media/knowledge level on COVID-19 and anxiety. First, the partial mediating effect of prejudice against infected people in the pathway of COVID-19 knowledge-prejudice against infected person-anxiety was found to be significant (research hypothesis 4: supported). This outcome is in line with the findings of a prior study that there is a correlation between the level of knowledge about infectious diseases and the discriminatory thoughts against infected people.102627 In addition, it supports the findings of another study that argued that lack of information and knowledge about COVID-19 can raise public anxiety and horror by triggering negative emotions such as fear of infected people.282930 This suggests that having the right knowledge about COVID-19 can reduce stigma towards infected people and ultimately reduce anxiety. Since distorted perceptions and attitudes towards infected people may likely appear in the early stages of epidemic10 when there is not much information out there, the media should provide fast and accurate information in real-time and strengthen communication strategies aimed at mutual understanding to increase the level of implementation of infection-preventive behaviors and discourage discrimination and distrust.
Moreover, the partial mediation effect of prejudice against infected people was found to be significant in the pathway of media usage-prejudice against infected person-anxiety, and the partial mediating effect of fear of infection was also found to be significant in the pathway of media usage-fear of infection-anxiety (research hypothesis 4: supported). These findings suggest that the levels of anxiety due to the information provided through the media in the COVID-19 situation may vary depending on the fear of infection or the stigma towards the infected person, which may be caused by the perception of low-risk control. This also supports the findings of previous studies93132 that the newer the risks are, the greater is the tendency of people to acquire relevant knowledge through the media. These studies argue that if correct and balanced information is not provided, fear of infection may spread by overestimation of risk, which then amplifies fear and increases psychological and social stress. Therefore, by organizing and delivering information on COVID-19 with a focus on accuracy, reliability, fairness, and ease of understanding, the mental health of the general public should be protected. The media must focus on providing information without any distortion or prejudice, and through proper understanding and response to the risk of infection.
Suggestions for future research centered on the limitations of this study are as follows. First, since this study was conducted in the context of the media reporting environment and the spread of COVID-19 in Korea, it has a limitation in generalizing the outcomes for other cultures. Therefore, it is necessary to verify the research model in various countries and cultures in future studies. Second, in this study, the relationship between variables such as fear of infection and prejudice against infected people was examined based on the levels of media usage. However, it is necessary to analyze the relationship with distorted perceptions of infection based on the usage behavior and relative influence of various media. Moreover, in the case of a causal relationship between knowledge about COVID-19 through media and mental health, it is necessary to expand and compare the influencing factors centering on parameters, such as infection-preventive behavior or health promotion behavior. As the COVID-19 pandemic continues, a study on symptoms such as depression and insomnia is warranted, as well as research on the relationship between the relevant causes. Third, in this study, structural equation model analysis was conducted focusing only on the individual characteristics of the study subjects. Nevertheless, in future studies, it should be expanded to a multi-layered model so that the effects of individual-level variables as well as regional variables, such as the number of confirmed patients, the number of deaths, medical support, and mental health support, can be analyzed. Despite these limitations, this study is meaningful in that it offers a theoretical basis for psychological countermeasures considering the lack of studies related to the influence of media and knowledge level on the anxiety caused by COVID-19.
Go to :
 XML Download
XML Download