

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Adverse childhood experiences (ACEs) are used to describe all types of abuse, neglect, and other potentially traumatic events occurring in children under the age of 18 years.1 ACEs include emotional abuse, sexual abuse, physical abuse, neglect, abandonment, lack of affection, domestic violence, mental health issues, use of alcohol or drugs, and imprisonment.2 ACEs are a risk factor for mental health disorders and can have negative effects such as chronic stress responses.3 Several studies have shown that the risks of developing a mental disorder, such as anxiety, depressed mood, posttraumatic stress disorder, suicide attempts, and substance abuse, are highest after ACEs.145 ACEs are globally positioned as a matter of public mental health.6 In the United States, just under half (46%) of children have experienced at least one ACE.7 Previous studies8910 have substantiated the link between ACEs and negative outcomes, including poor academic achievement, poverty, unemployment, disability, and early death.
Children and youth exposed to stress are likely to develop depression, anxiety, or maladaptive behavior, as well as to suffer from difficulties with emotional regulation and interpersonal relationships, affecting school functioning and learning.11 A study examined young children at risk of neglect and abuse and demonstrated that a four-year accumulation of ACEs tripled the risk of the disease two years later.12 The type of stress that results when children and adolescents experience ACEs might stimulate a negative activation of the body stress response systems.13 Chronic stress exposure could lead youth to perceive their environments as unpredictable and threatening.14 The reorganization of the stress systems of children requires that they experience safety in their environments.15 Therefore, the ACEs of children and stress can be considered closely related.
ACEs are an important clinical status index that directs planning and intervention in moving toward trauma-informed care.16 Because ACEs may lead to such negative health and psychological effects, it is necessary to recognize factors that may help to protect children and adolescents from ACEs.17 Furthermore, research findings have shown that a person's cumulative ACE score has a relationship over their lifetime to various health, social, and behavioral issues.1819 As demonstrated in prior research,16 ACE assessments may be an essential component, before implementing psychosocial interventions in children and adolescents. ACE timing is important in the prevention and treatment of somatic and mental conditions associated with ACEs.20 ACE-related studies could prevent ACEs, mitigate the effects of ACEs, and foster child and family resilience.6 We need to concentrate on the improvement of mental health among children, youth, and families to identify, resolve, and prevent ACEs.
Until now, the correlation between ACE and mental health results has mostly been investigated among adults in previous research.202122 One study23 reported that the prevalence of ACEs in a pediatric population could explain the onset and developmental impact of trauma. Nevertheless, investigations into understanding the adverse experiences of children and adolescents in Korea have been limited. Therefore, we aimed to examine the degree of ACE and correlation with stress in Korea's children and youth.
METHODS
Subjects
The sample subjects were selected from 3,937 children and adolescents from 23 elementary, middle, and high schools and 11 local children's community centers in one city in Korea. The children's community center was defined as a children's welfare service organization that provides after-school care, education, and play activities for children younger than 18 years of age who need community care. We selected classrooms that could be surveyed at the school identified and selected the subjects that could be surveyed at the final selected school. Multilevel cluster samples were extracted, and schools and local children's community centers were surveyed from among the local organizations. Respondents were excluded if they were missing survey data, resulting in a final sample size of 3,556.
Measurements
The measurement comprised questionnaires concerning demographic characteristics such as sex, age, academic achievement, and socioeconomic status (SES), questions about the level of stress, and ACEs. The SES and academic function were categorized into five levels which were ‘high, middle-high, middle, low-middle, and low' according to the student's response as our prior study.2425 The survey was conducted from March to October 2017.
ACEs Study is the research conducted by the U.S. health maintenance organization Kaiser Permanente and the Centers for Disease Control and Prevention. Ten categories of ACEs were included in the survey.2627 The ACEs is a valid and reliable measure of childhood adversity that has been used extensively in large-scale ACEs studies.28 Children and adolescents were asked if they had experienced the ACE category. The ACE category and items were as follows: 1) emotional abuse (Did a parent or other adult in the household often or very often swear at you, insult you, put you down, or humiliate you? Or act in a way that made you afraid that you might be physically hurt?); 2) physical abuse (Did a parent or other adult in the household often or very often push, grab, slap or throw something at you? Or ever hit you so hard that you had marks or were injured?); 3) sexual abuse (Did an adult or person at least 5 years older than you ever touch you or have you touch their body in a sexual way?); 4) lack of affection (Did you often or very often feel that no one in your family loved you or thought you were important or special? Or your family did not look out for each other, feel close to each other, or support each other?); 5) neglect (Did you often or very often feel that you did not have enough to eat, had to wear dirty clothes, and had no one to protect you? Or were your parents too drunk or high to take care of you or take you to the doctor if you needed it?); 6) abandonment (Was a biological parent ever lost to you through a divorce, abandonment, imprisonment, or other reason?); 7) domestic violence (Was your mother or stepmother often or very often pushed, grabbed, slapped, or had something thrown at her? Or, Sometimes, often, or very often kicked, bitten, hit with a fist, or hit with something hard? Or, was ever repeatedly hit over at least a few minutes or threatened with a gun or knife?); 8) alcohol or drugs (Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?); 9) mental health issues (Was a household member depressed or mentally ill or did a household member attempt suicide?); and 10) imprisonment (Did a household member go to prison?) (Supplementary Table 1). The response for each category was ‘Yes’ or ‘No’. Counting each ACE as one, respondents were reported as having an ACE score of 0 to 10.27 In our study, internal consistency was measured using Cronbach's α.29 Cronbach's α-level was 0.767 for the total ACEs scale.23
In this study, the stress scale was selected from the national survey questionnaire of National Youth Policy Institute in 2011.30 Assessment of type of the stress is a self-reported stresses such as the relationship with parents/siblings/friend/opposite gender/senior and junior/teacher, physical appearance (e.g., height, body, and face), physical health, mental health, family circumstances (economic status), the difficulty of deciding the occupation (future plan), and academic function. In our study, internal consistency was measured using Cronbach's α.29 Cronbach's α-level was 0.880 for the total stress scale.
Data analyses
SPSS Statistics 22.0 (IBM Corp., Armonk, NY, USA) was used to perform statistical analyses. Internal consistency, measured by Cronbach's alpha, was used to assess reliability of the questionnaires. A chi-square test was conducted to determine whether the sex frequencies differed significantly. A chi-squared test is a statistical hypothesis test that is accurate to be conducted when the test statistic is chi-squared based on the null hypothesis, specifically Pearson's chi-squared test and its variants.31 Pearson's chi-squared test is used in one or more sections of a contingency table to assess if there is a statistically significant difference between the predicted frequencies and the observed frequencies.32 In addition, it was analyzed the each ACE scores, sex, and type of school. Correlation coefficient between ACEs and scores of stress responses were computed with correlation analysis in SPSS. The p-value of 0.05 was set for statistical significance.
RESULTS
According to the demographic characteristics of respondents, 1,523 boys (43.1%) and 2,024 girls (56.9%) were included in the final analysis. The mean age was 13.77 years (standard deviation = 2.23). By type of school, 1,751 students (49.2%) were elementary students, 1,206 (33.9%) were middle school students, and 599 (16.8%) were high school students. Regarding SES, more than half of the respondents were at the middle level (n = 1901, 53.5%), followed by 1,016 (28.6%) at the high-middle level. Regarding academic achievement, most of the respondents (1,212; 34.1%) were categorized as middle level, followed by high-middle-level (1,092; 30.7%) (Table 1).
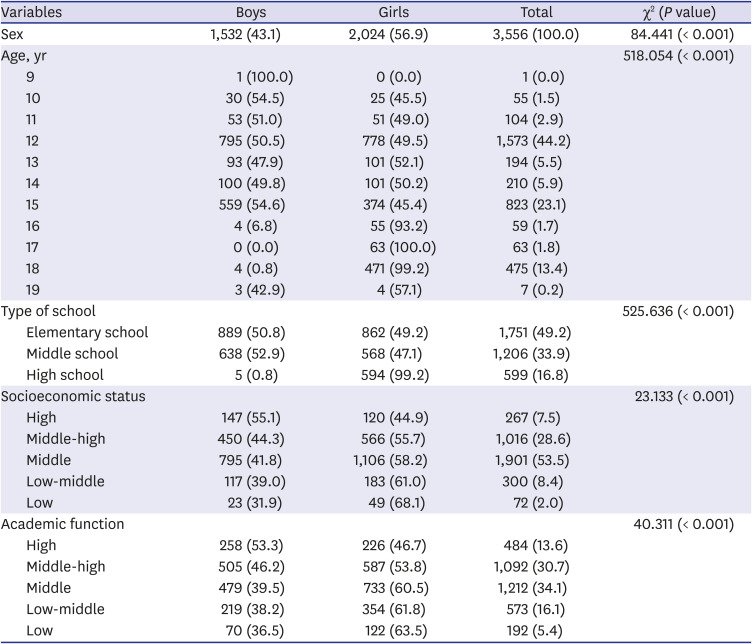
Table 1
Demographic characteristics of the respondents (n = 3,556)
![]()
Overall, 23.5% (n = 835) reported at least one ACE and 1.8% (n = 63) reported experiencing four or more ACEs. Boys of the respondents (24.5%) reported more ACEs than girls (22.7%) (Table 2 and Fig. 1).
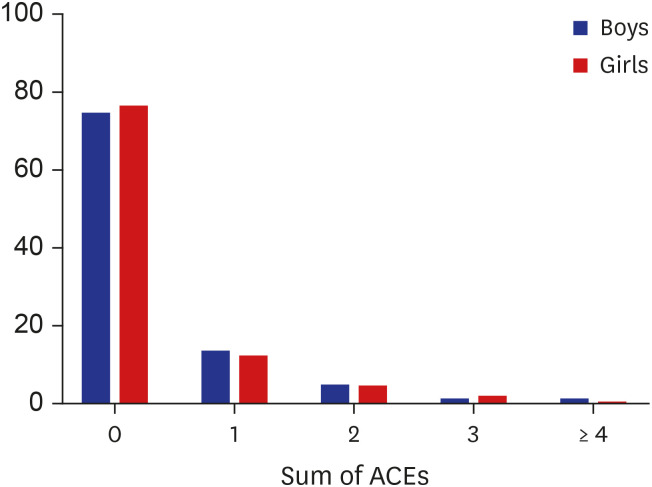
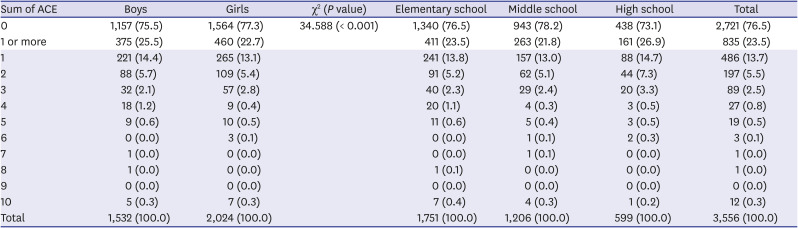
Fig. 1
Sum of ACEs among the urban pediatric population in Korea (n = 3,556).
ACEs = adverse childhood experiences.
![]()
Table 2
Cross-sectional analysis of the sum of adverse childhood experiences (n = 3,556)
![]()
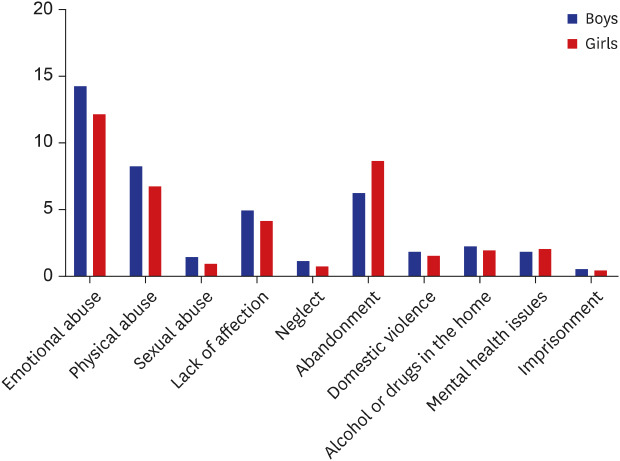
The most common ACEs were emotional abuse and physical abuse. A total of 13.2% (n = 468) respondents reported being victims of emotional abuse, 7.7% (n = 275) reported being victims of abandonment, and 7.5% (n = 268) reported experiencing physical abuse. Of all young children, 4.6% (n = 164) reported experiencing a lack of affection (n = 164). A total of 2.2% (n = 78) respondents reported living with a household member who had a substance abuse problem, and 2.1% (n = 75) reported having a household member with mental health issues. Among them, 1.8% (n = 65) of respondents reported being victims of domestic violence, followed by 1.3% (n = 47) who were victims of sexual abuse. Another 1.1% (n = 39) reported experiencing neglect. Few children reported that they lived with a household member who had been to prison (3.6%, n = 24) (Table 3 and Fig. 2).
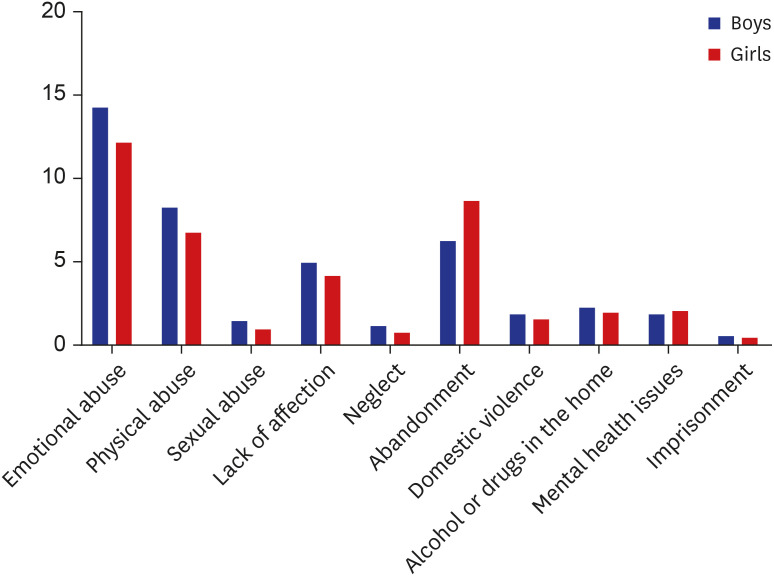
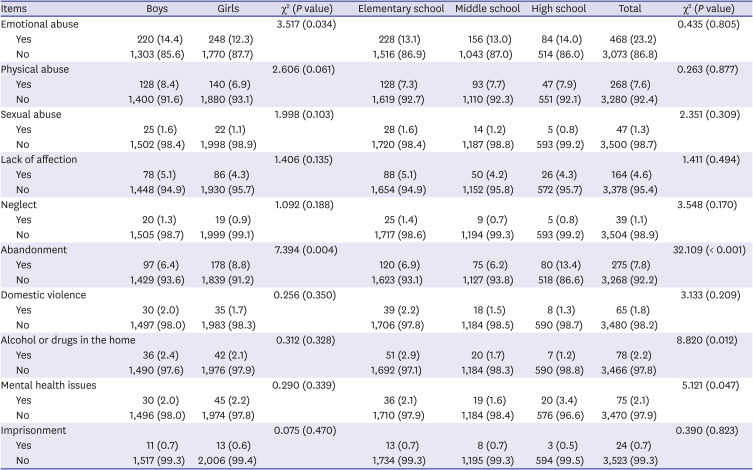
Fig. 2
Response items of adverse childhood experiences among the urban pediatric population in Korea (n = 3,556).
![]()
Table 3
Cross-sectional analysis by detailed items of adverse childhood experiences (n = 3,556)
![]()
Additionally, the self-reported measures of stress were associated with the ACE score (Supplementary Table 2).
DISCUSSION
This is the first study of self-reported ACEs from a community-based pediatric population on mental health outcomes in Korea. The data from this study revealed that children and adolescent ACEs are correlated with stress.
First, our results showed that 23.5% of children had at least one ACE. In the 2007 Minnesota Student Survey, one of the most well-designed studies comprising 136,549 students (6th, 9th, and 12th grades), 28.9% of students reported at least 1 ACE.9 The multiple types of ACEs should be considered as risk factors in children and adolescents. The research from the 2011/2012 National Survey of Children's Health (NSCH), a nationally representative survey by the United States Maternal and Child Health Bureau, reported that 56% of 33,747 adolescents (ages 12–17 years) had experienced at least one ACE.17 The frequency of 56% was higher than 23.5% and 28.9% of ACEs (> /1) in our study and the Minnesota study,9 respectively. In the national sample study in the US,17 the reports on ACEs were delivered by the parent or guardian in contrast to our study and the Minnesota study,9 in which children and adolescents responded to ACEs through a self-reported questionnaire. Previous research has suggested that individuals who have experienced traumatic events and emotional or physical abuse are unlikely to reveal their adverse experiences spontaneously.33 We found that 23.5% of students revealed more than one ACEs, and the result was similar to the data in the US community study9 with self-reporting among the community samples. In comparison, studies from the high-risk population showed a higher prevalence of ACEs than in our community sample. From these reports, one or more ACEs were reported as 50% to 80%, and the prevalence was reported differently according to the trauma exposure, the juvenile offender, and adolescent groups in socioeconomically disadvantaged communities.233435363738
Second, our results of the sum of ACEs indicate that boys accounted for 25.5% and girls were reported as 22.7%. In particular, boys (14.4%) reported more emotional abuse experience than girls (12.3%), and girls (8.8%) reported more abandonment experience than boys (6.4%). The prospective cohort study (n = 9,959; aged from 0 to 16 years) conducted in the United Kingdom reported that the distribution of ACE scores was similar in boys and girls.39 There were differences in the prevalence of bullying (28.6% in boys and 23.7% in girls) and physical abuse (17.1% in boys and 20.9% in girls) by sex. According to the reports of the ACEs in 1,284 adolescents (aged 10–14 years) in resource-poor neighborhoods,40 the boys reported more exposure than girls to physical neglect (32.95%), violence victimization (52.27%), and sexual abuse (8.77%). The community-based study of high school seniors (n = 1,093) from public schools in the US metropolitan area showed that the sexual abuse of youth was more detrimental to boys than girls. However, the number of boys that reported sexual victimization was low. Additionally, boys who had experienced ACEs were more likely to engage in antisocial behavior early in young adulthood than girls with similar ACEs.41 However, the findings were inconsistent with ours in that the 2007 Minnesota Student Survey9 showed that girls more commonly reported all types of ACEs. Additionally, boys were least likely to report household dysfunction and experiences of abuse. The degree of associated risk for outcomes differed between boys and girls. Early ACE surveys indicated females more frequently reported ACEs in the clinic-based sample, but the difference was not statistically significant.42 Further understanding of ACE differences by sex and the potential impact of ACEs on mental health are needed.
Third, the most common ACEs in our study were emotional abuse reported by 13.16% of all respondents (14.4% of boys and 12.3% of girls). In the UK cohort study between birth and 16 years, the prevalence of emotional neglect was 26.5% in boys and 21.2% in girls.39 Our findings are consistent with previous results that emotional abuse (33%) was identified most commonly among 60,598 respondents.43 This is similar to the finding that adolescents (n = 1,284) 10–14 years of age in 14 countries most commonly reported emotional abuse (51.87%).40 The emotional abuse is associated with the highest predictor of attempted suicide and depressive disorders.4445 In Korea, the suicide rate and proportion of adolescents who attempt suicide have gradually increased. Emotional abuse was shown to be related to internalizing problems,45 and the factors of emotional abuse need more attention in future practical research.
Fourth, our results indicate that exposure to adverse experiences is highly correlated with various stress responses. This is consistent with previous findings46 that a stress response could occur if children experience ACEs, such as emotional or physical abuse, or exposure to violence or chronic neglect. Several authors have found relationships between children's and adolescents' adverse experiences, stress, and health.122347 The results of the present study are similar to a previous finding48 showing the effects of ACEs, perceived stress and social support on the health of 321 undergraduates. It showed that higher levels of ACEs were associated with greater stress levels and lower levels of social support.48 Additionally, altered neurobiological processes from ACEs were demonstrated to increase sensitization to stress, and a prior study49 suggested that ACEs may have developmental origins for adult mental health. Among the ACEs, maltreatment, social isolation, and low SES stand out as the contributing factors to inflammation, depression, and the clustering of metabolic risk markers.4
ACEs are related to many physical and psychological adverse outcomes. If an individual does not address and recover from traumatic experiences, the negative effects might be magnified through generations.1346 The New Hampshire Division for Children Youth and Families has taken a trauma-informed approach to screen and assess the children of trauma and mentor their parents.2 Hence, early mental health intervention could prevent the short- and long-term adverse outcomes associated with ACEs. Even without current exposure to ACEs, the analysis of ACEs could provide methods to prevent or mitigate the impact of ACEs should they occur.6 Thus, we must improve the psychosocial environment of children to prevent multiple mental health risks. Prevention and early intervention could assist in supporting the healthy development of pediatric populations and mitigate the lifelong and transgenerational health effects of trauma. To accomplish that, we should consider the cultural impacts and negative perceptions of mental service interventions in Korea, particularly the application of programs for young children.50 With this consideration, developing trauma-informed mental health policies to prevent ACEs and early intervention in the school and community are needed in Korea.
Our study has several limitations. The results were specific to one city district and may not be generalizable to other communities. The participants in local children's community centers were not randomly selected; thus, selection-bias could exist. The results were based on the self-reporting of ACEs by children and adolescents, and the actual ACE conditions may have been underreported by respondents when completing the questionnaire. Despite these limitations, our findings have implications for future research understanding and youth mental health prevention. The results of this study show the need for national universal screening of ACEs in children and adolescents.
The findings of this study suggest the need for assessments for planning prevention and intervention services for ACEs. Understanding the extent of ACEs, effects of ACEs on mental health status, and subsequent treatment process for prevention could be improved.51 Thus, retrospective research should be conducted to show that mental health and ACEs are correlated in children. Further research should focus on developing evaluation and treatment systems that improve the mental health of children.
 XML Download
XML Download