

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Trauma is the leading cause of death worldwide, in adults aged ≤ 39 years, and is one of the greatest health problems in both low and high-income countries.1 However, systematic efforts to lower trauma-related deaths are limited; with the exception of a few countries with well-established trauma systems, no countries have shown a marked reduction in trauma-related death rates.2 Most healthcare fields in Korea have made some progress; however, trauma care remains at a rudimentary stage, and continuous quality control using consistent and objective scales is lacking.
Preventable trauma death review is a classic quality control trauma care systems tool, defined as the review of trauma-related avoidable deaths in which the patient would have survived if transferred to an appropriate hospital in time for appropriate treatment.3 Despite limitations, this index is still important in determining the performance of trauma care systems. The preventable trauma death rate has been measured inconsistently using different methods in Korea, with reported rates of 50.4% in the late 1990s, 35.2% in 2009–2010, and 30.5% in 2015.456
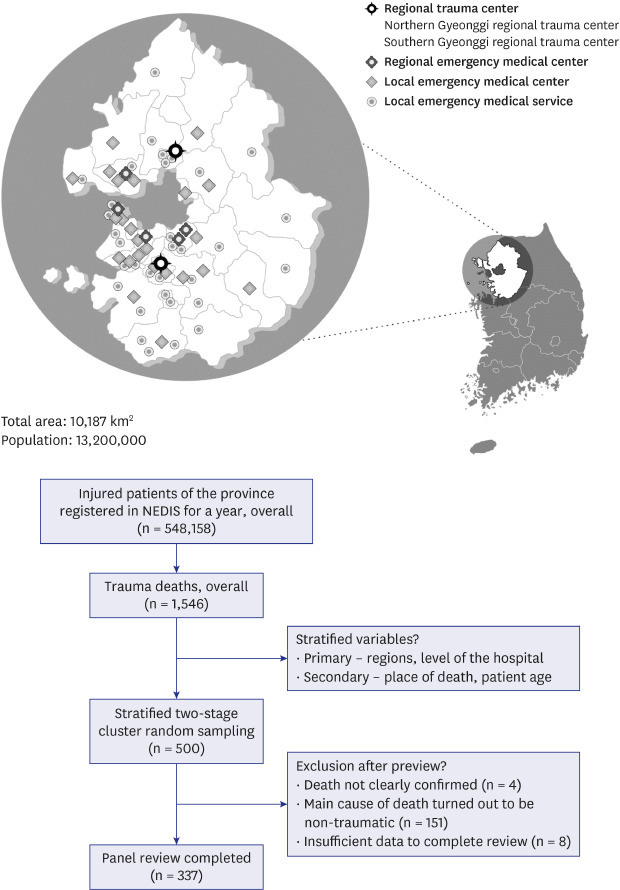
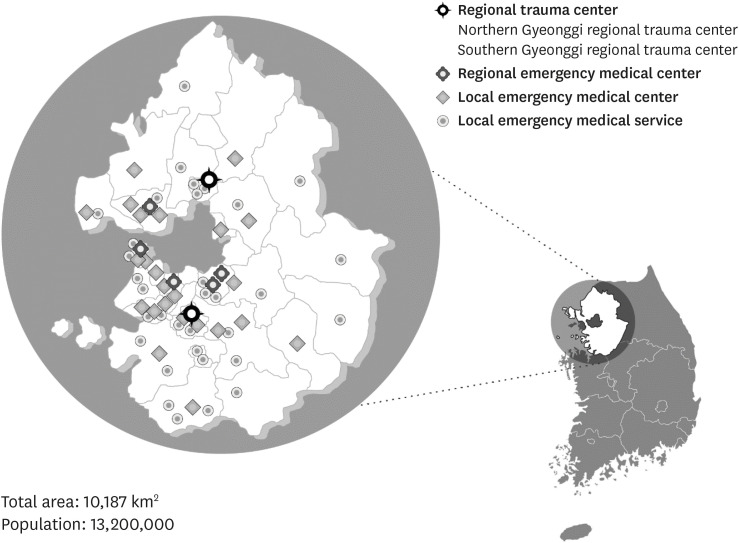
Gyeonggi-do, the region evaluated in our study, is about the size of the Los Angeles County in the United States. It is densely populated with approximately 13.09 million people, a quarter of the entire Korean population.7 Along with Seoul, Gyeonggi-do is the most urbanized and medically dense Korean region with 57 emergency medical care facilities, including five regional emergency medical centers at the time of survey (Fig. 1). However, compared with the high accessibility to emergency medical care, its trauma care system, similar to many others in Korea, is still at a rudimentary stage with multiple problems. A review of trauma-related deaths in this region can be used as the basis for reorganizing resources and establishing inclusive trauma systems in the region.
This study aimed to obtain a reliable measure of the preventable trauma death rate in a single province as of 2017, analyze the related problems, and obtain foundational data for devising enhancement measures that can be used for regional-level quality control, to advance the national trauma system in Korea.
METHODS
Study population
This study included data on those who experienced trauma-related deaths from 64 hospitals providing emergency medical care in the Gyeonggi Province from January 1, 2017 to December 31, 2017. Trauma-related death was defined as the deaths of patients who had presented to the emergency department (ED) and had one or more S or T codes as per the Korean Standard Classification of Diseases (KCD) seventh edition (nearly identical to the 10th revision of the International Statistical Classification of Diseases and Related Health Problems) in their diagnosis while exiting the ED or hospital (excluding patients with a code for frostbite, addiction, intoxication, drowning, burns, other and unspecified effects of external causes, or complications regarding surgical and medical care). As of December 31, 2017, 400 out of 402 total emergency medical care facilities in Korea had registered their data (99.5%); 64 emergency medical care facilities in Gyeonggi Province were registered. Overall, 1,546 trauma-related deaths were registered by 57 of the 64 hospitals in Gyeonggi Province. Of these, 263 patients were dead on arrival (DOA) (17.0%), 97 deaths occurred in the ED (6.3%), 848 deaths occurred after hospital admission (54.8%), and 338 deaths were after transfer (21.9%).
Sampling
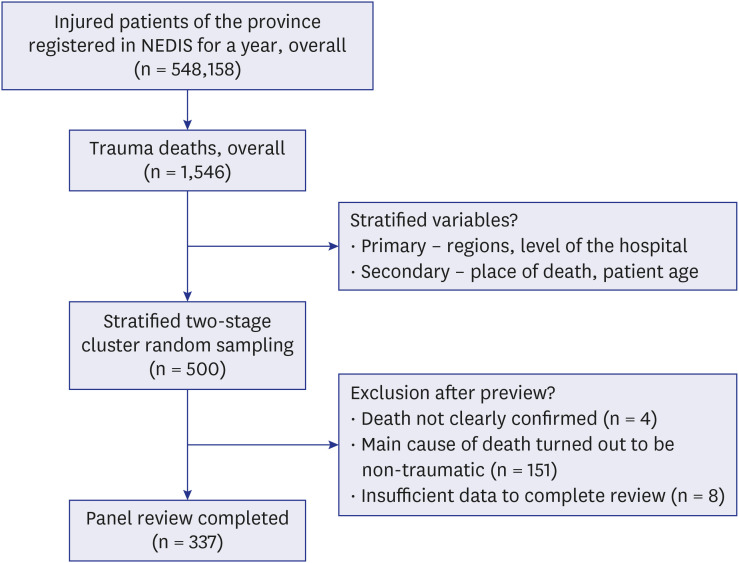
The study and target populations were identical in background characteristics, and to compute a regionally representative preventable trauma death rate in Gyeonggi region, a stratified two-stage cluster sampling method was applied, and stratification was designed as a double layer (Fig. 2). The National Emergency Department Information System (NEDIS), a database containing information on patients presenting to the ED in Korea, with documentation of the treatment process in real-time, was used as the sampling frame. Sampling was performed on all cases in facilities with deaths after transfer to a second facility, according to the sample size of facilities with no deaths after transfer to a second facility. Sample size for each facility was set according to the type of hospital (regional trauma center [RTC], regional emergency medical center, local emergency medical center, local emergency medical service), number of deaths (≥ 100, 50–99, 30–49, 10–29, < 10), place of death (DOA in first facility, death in ED in the first facility, death after hospital admission in the first facility, death after transfer to second facility), and patient age (≤ 14 years, 15–54 years, ≥ 55 years). For patients aged ≤ 14 years, the entire patient pool was sampled. Deaths from all RTCs were sampled, and deaths from all regional emergency medical centers, except for one center, were sampled. The extracted sample consisted of 478 cases from 42 facilities, with deaths after transfer to a second facility, and 22 cases from six facilities without deaths after transfer to a second facility, totaling 500 cases from 48 facilities (80 cases from 2 RTCs, 75 cases from four regional emergency medical centers, 265 cases from 23 local emergency medical centers, and 80 cases from 19 local emergency medical services).
Data collection and type of data
With permission from the local government, patient medical records were collected from hospitals that transferred the sampled trauma patients to the 48 study hospitals. Based on the preventable trauma death review form (Supplementary Data 1) that we developed, the study hospitals submitted the necessary data and completed checklists. Types of data included emergency care record, death certificate, CD containing image copies, and copy of medical record. The copy of the medical record had to contain initial care record at the ED, the progress note, nursing care record, imaging and blood test results, and admission/discharge record. We requested additional data when needed, and medical records were collected from the 48 hospitals in which the trauma patients had died and from the 221 hospitals that had transferred these patients to the final hospitals to investigate the 500 cases included in our study.
Composition of designated assistants and preventable death panel and multidisciplinary reviewing
The preventable trauma death review form was based on the preventable trauma death evaluation form with an embedded audit filter as in the World Health Organization (WHO) guidelines for the trauma quality improvement program.1 Designated assistants consisting of seven trauma coordinators working in RTCs nationwide investigated and recorded the general characteristics of patients, injury-related information, and transport and treatment-related information using the preventable trauma death review form prior to the review by the preventable death panel. The preventable death panel consisting of 15 dedicated trauma professionals working in RTCs nationwide, performed an initial evaluation of the preventability of deaths using the data extracted by the designated assistants. For a multidisciplinary review, three teams were formed, with each team consisting of two general surgeons, one thoracic surgeon, one neurosurgeon, and one emergency physician. After individual evaluations, the panels from each team came together to present the cases they had reviewed, and they discussed and reached a consensus for a final assessment of the preventability of trauma-related deaths.
Criteria for preventable trauma deaths
The criteria presented by the WHO guidelines for trauma quality improvement programs1 were used as the criteria for the preventability of trauma-related deaths. These criteria assess preventability in consideration of the severity of trauma and appropriateness of the provided treatment. Preventable trauma deaths were computed by summing “preventable (P)” and “potentially preventable (PP)” deaths.
Qualitative analysis
The preventable trauma death rate was computed using the selected sample; we also extracted data on patients who died after inter-hospital transfer, who showed a substantially high preventable trauma death rate in a previous study,4 and patients who died after hospital admission. These patients having the highest percentage of various trauma death stages were therefore analyzed to provide feedback to enhance the quality of trauma patient care. These additional data were only used for qualitative analysis and were not included in the computation of the preventable trauma death rate. All preventable trauma deaths included in the qualitative analysis were classified according to five causes of death: bleeding, sepsis/multi-organ dysfunction syndrome (MODS), central nervous system (CNS) injury, respiratory failure, and cardiac issues. One main cause of death was chosen, but more than one cause of death could be recorded.
Statistical analyses
The population was estimated using the weighted values of sampling rates. The methods used for mortality estimation and adjustment in a previous study4 were used. Risk factors of preventable trauma deaths were identified using multiple logistic regression analysis, and variables previously identified to potentially impact the preventable trauma death rate were used as explanatory variables. Variables included in the logistic regression model were age, type of hospital, inter-hospital transfer, time from accident to death, time from accident to arrival at the hospital, and mechanism of injury. Risk factors were analyzed using the observed number of death cases instead of the estimated population. We also analyzed consistency among panels using the Cohen's Kappa index to establish the reliability of the results.
RESULTS
General characteristics
After excluding 163 patients (four patients, death was not clearly confirmed; 151 patients, cause of death was non-traumatic; and eight patients, insufficient data) from the total sample of 500 patients, the preventable trauma death rate was computed based on 337 patients. Table 1 shows the baseline characteristics of the subjects. In addition to the values for stratified samples, estimates calculated based on them and percentage in the population are also presented in Table 1. There were more men in our sample (67.1%), with a mean age of 59 years, and 75.7% of the sample was ≥ 55 years. The most common type of hospital in which trauma-related deaths occurred was the local emergency center (48.4%), and approximately 77.2% of patients presented to the center via the 119 emergency medical service (EMS) instead of being transferred from another hospital. The most common mechanism of injury was a traffic accident (34.7%), and in most cases, the time from accident to death was ≥ 7 days (27.7%). In most cases, the time from accident to arrival at the hospital was < 1 hour (51.8%).
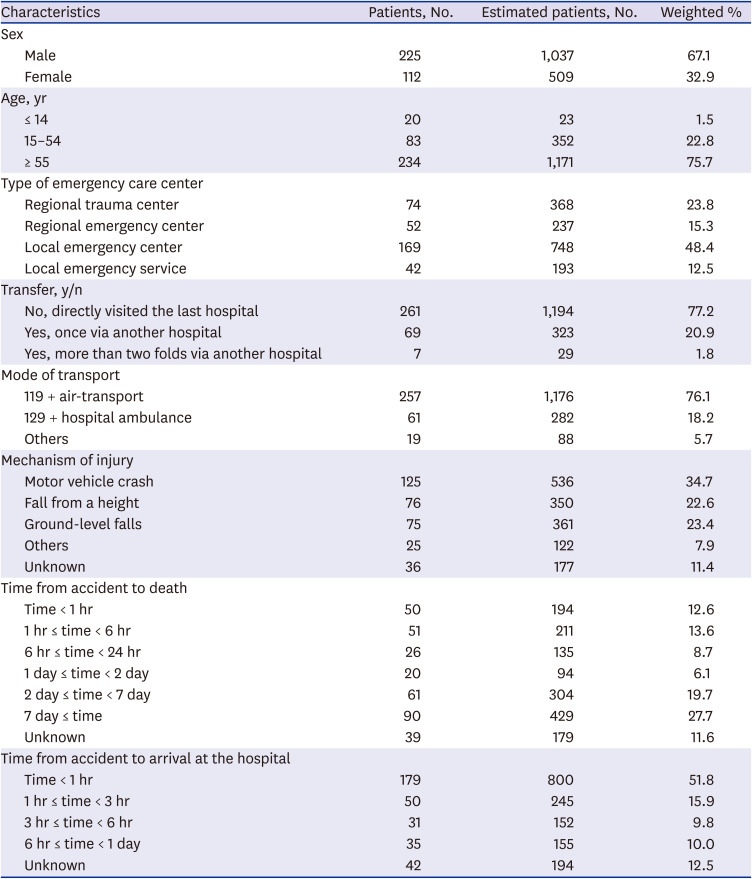
Table 1
Baseline characteristics of the study participants (n = 337) (estimated n = 1,546)
![]()
Preventable trauma death rate and relevant factors
The preventable trauma death rate in Gyeonggi region in 2017 was estimated to be 17.0% (95% confidence interval [CI], 13.7–20.3), and 2.9% (95% CI, 0.0–6.2) of these deaths were P deaths, while 14.1% (95% CI, 11.1–17.1) were PP deaths (Table 2). The Cohen's Kappa index of inter-rater reliability, measured after randomizing and sampling 120 cases, was 0.25 (fair reliability). The time from accident to arrival at the hospital influenced the preventable trauma death rate, though the risk was higher in patients who arrived at the ED within 1–3 hours (P = 0.01) and those who arrived within 3–24 hours (P = 0.09) of the accident than in patients who arrived within 1 hour of the accident. No significant differences were observed despite the risk being higher in patients who died < 6 hours after the accident (P = 0.06) compared with those who died between 6–24 hours after the accident The risk was also higher in patients admitted to non-RTC emergency care centers than in patients admitted to RTCs (P = 0.06) (Table 3).
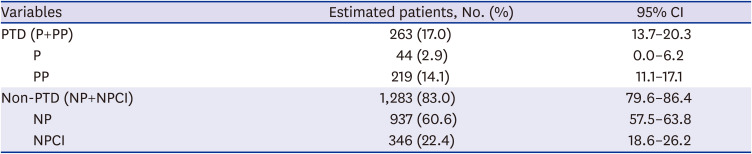
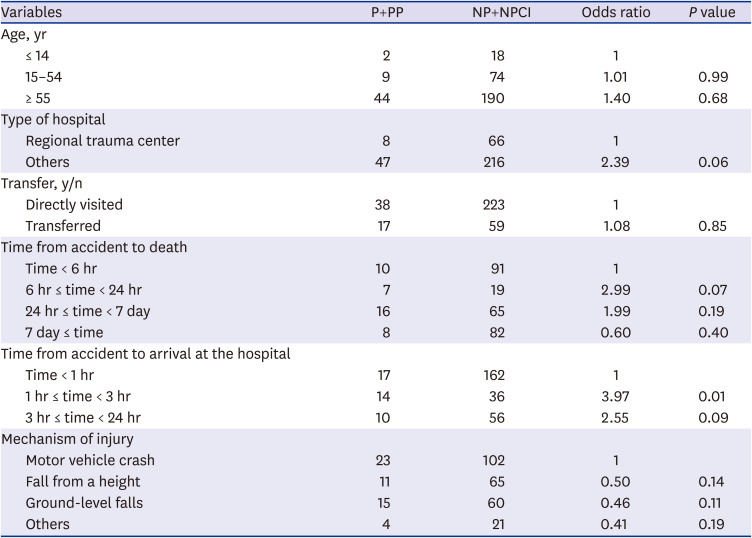
Table 2
Preventable trauma death rate (estimated n = 1,546)
CI = confidence interval, PTD = preventable trauma death, P = preventable, PP = potentially preventable, NP = non-preventable, NPCI = non-preventable, but with care that could have been improved.
![]()
Table 3
Factors associated with preventable trauma death (n = 337)
P = preventable, PP = potentially preventable, NP = non-preventable, NPCI = non-preventable, but with care that could have been improved.
![]()
Percentage of impact on preventable trauma death rate by stage and causes
Stages that affected preventable trauma deaths occurring in emergency care centers in Gyeonggi Province were classified into the pre-hospital stage, inter-hospital transfer stage, and hospital stage. The hospital stage (86.7%) had the greatest impact, followed by inter-hospital transfer stage (8.4%) and pre-hospital stage (4.9%). Of the 86.7% patients experiencing problems at the hospital stage, only 10.3% experienced them in an RTC, while 76.4% experienced them in a hospital other than an RTC (Table 4). The causes of death in preventable cases included hemorrhage in 39 (42.9%) cases, sepsis/MODS in 26 (28.6%) cases, CNS injury in 14 (15.4%) cases, respiratory failure in 11 (12.1%) cases, and cardiac failure in two (2.2%) cases. In one patient who experienced hemorrhage, the contribution to “death from traumatic brain injury and hemorrhagic shock” was considered to be identical and duplicated.
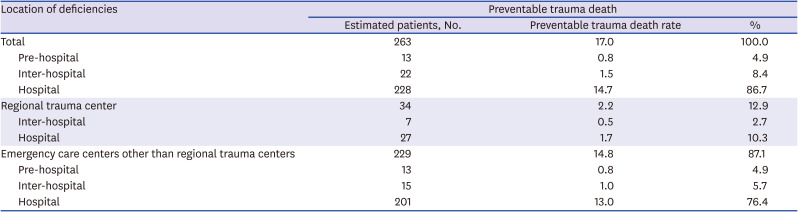
Table 4
Location of deficit and hospital types according to the preventable trauma death rate (n = 263)
![]()
Qualitative analysis of preventable trauma deaths
In addition to the 337 effective samples selected for determining the preventable trauma death rate, we analyzed an additional 10% of cases classified under “deaths after inter-hospital transfer” and “deaths after admission,” which were subgroups with the highest preventable trauma death rates in a previous study4; in total, 524 patients were included in the analysis of trauma-related death. Of the 524 patients, 93 were determined to have experienced preventable trauma-related deaths. The most common cause of death in preventable trauma-related deaths was hemorrhage, followed by sepsis/MODS, CNS injury, respiratory failure, and cardiac issues (Table 5). The opportunities for improvement (OFIs) in 39 patients in whom hemorrhage was the cause of death were analyzed and presented in Table 6, with a duplicate selection being included. Among the hospital-level problems, delayed surgery or embolization for hemostasis, experienced by 30 patients, was the most common OFI, followed by delayed/insufficient transfusion (experienced by 25 patients). We observed delays in diagnosis and intensive care treatment in 26 patients who died from sepsis/MODS. All 14 patients who died from CNS injuries had traumatic brain injury, with delayed craniotomy or failure to perform craniotomy as the main OFIs in these cases. When craniotomy was performed, the average time from arrival at the final destined hospital to surgery was 8.7 hours (median value, inter-quartile range; 3.3–15.0 hours).

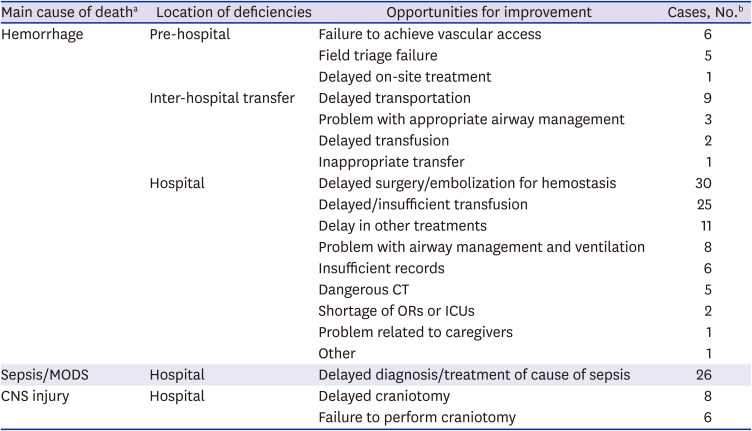
Table 5
Causes of death in preventable cases (n = 93)
| Causes of death | Cases, No. (%) |
|---|---|
| Hemorrhagea | 39 (42.9) |
| Sepsis/MODS | 26 (28.6) |
| CNS injurya | 14 (15.4) |
| Respiratory failure | 11 (12.1) |
| Cardiac issue | 2 (2.2) |
MODS = multi-organ dysfunction syndrome, CNS = central nervous system.
aIn one case, the contribution of hemorrhage and CNS injury to the cause of death were considered identical and duplicated.
![]()
Table 6
Opportunities for improvement in preventable trauma deaths according to main cause of death and location of deficiency
CT = computed tomography, OR = operation room, ICU = intensive care unit, MODS = multi-organ dysfunction syndrome, CNS = central nerve system.
aThe three most common causes of death are presented. bA single case may appear multiple times due to two or more identified opportunities for improvement.
![]()
DISCUSSION
The first reported preventable trauma death rate in Korea was 50.4% in 19978; since then, there has been a consistent decline in this rate, with the most recent report showing a rate of 30.5% in 2015, suggesting an improvement.4 This rate is similar to that reported by Motomura et al.9 in Chiba Prefecture in 2011 (29.0%), although it is still higher than those reported in countries with stable trauma care systems, such as the United States and Canada. In 2005 in the US, the rate was 6.7% in Utah,10 and 2.4% in California, in 1998.11 The preventable trauma death rate in Gyeonggi Province in 2017 was 17.0% according to this study, which is a substantial improvement from that reported in a national survey using 2015 data.4 This may be attributable to the high accessibility to trauma care in Gyeonggi Province, as it is a medically dense area compared with other regions in Korea. The establishment of diverse emergency medical care facilities that have not been designed for trauma care may poorly reflect the actual outcome of the trauma care system.12 If the improvement in the preventable trauma death rate in Gyeonggi region found in this study is a result of enhancement in the quality of the trauma care system, this could be attributable to the two RTCs in southern/northern Gyeonggi Province that opened in 2016 and 2017, respectively.
The time from accident to arrival at the hospital and RTC as the final care institution were identified to have significant effects on the determination of preventability. This is understandable since reducing the time taken from the accident to definitive treatment and establishing designated trauma centers are critical to the success of early trauma care systems worldwide. However, delayed transfer to the final treatment facility seems to be affected by the transfer process instead of the initial transportation in the pre-hospital stage. Unnecessary inter-hospital transfers and excessive testing and procedures performed at transferring hospitals resulting in delays in patient arrival at the final treatment facility have been reported in a prior study conducted in Gyeonggi Province.8 Twenty-seven of the 228 patients who experienced preventable trauma deaths due to problems in the hospital stage were speculated to have died due to problems at an RTC (Table 4). Considering that 23.8% of all trauma-related deaths (368/1,546) occurred in an RTC, the number of trauma-related deaths that had occurred in one of the 62 hospitals other than an RTC in Gyeonggi Province was more than three-fold higher than that in one of the two RTCs (368 vs. 1,178); however, there were 7.4 folds more hospital-stage problems that led to preventable trauma deaths (27 vs. 201). This highlights the distinct difference in the capacity to treat severely injured patients, between RTCs and other hospitals. Assuming that RTCs have an unlimited pool of resources and thus can accept an unlimited number of patients, inter-hospital transfer complications could have been prevented if patients were transferred to an RTC for initial treatment. In such cases, we can substitute the fraction of preventable trauma deaths that occurred in the hospital stage in hospitals other than an RTC (13%) with the fraction of preventable trauma deaths that occurred in an RTC (1.7%); this leads to a total preventable trauma death rate of 4.2% (pre-hospital stage 0.8% + inter-hospital transfer stage 0% + hospital stage 3.4% [1.7%+1.7%]). With this calculation, we can estimate that 198 regional trauma patients could be additionally saved per year. With a total preventable trauma death estimate of 263, preventable trauma deaths can be lowered by 75.3% (198/263) according to our findings. However, trauma-related deaths were calculated based on the NEDIS database; a higher estimate of trauma-related deaths may be derived if the trauma-related deaths that were not registered in the NEDIS were taken into consideration. Although this is a simple arithmetic estimate that disregards the capacity of RTCs for accepting patients, it presents implications for the direction of future regional trauma systems. Currently, RTCs in southern and northern Gyeonggi together have 173 bed-spaces, and they serve a function similar to that of a level 1 trauma center, as defined in the resources for optimal care of the injured patient.13 Considering the 12-million population in the region and the lack of designated trauma care facilities other than a level 1 facility, the capacities of these RTCs are substantially low. This can be addressed by establishing a truly inclusive regional trauma system, by restructuring the available medical resources, making them trauma care appropriate, and by modifying the pre-hospital transport system so that severe trauma patients are directly transported to an RTC. Thus, a consultative organization that can coordinate non-RTC emergency medical care facilities, 119 EMS, and local governments with the existing RTCs is needed, and the recently founded Gyeonggi Trauma Systems Organization could play an important role to this end.
Instead of merely calculating the preventable trauma death rate, this study ultimately aimed to enhance the quality of trauma care by providing constructive feedback to facilities that encountered preventable trauma deaths. For this purpose, we performed a qualitative analysis by including an additional 10% of “deaths after inter-hospital transfer” and “deaths after admission,” which showed the highest preventable trauma death rates in a prior study.4 We focused on identifying OFIs that can be used as a basis for establishing corrective action plans to reduce preventable trauma death rates. Based on previous studies and guidelines,110131415 OFIs were identified and listed according to the main cause of death: hemorrhage, sepsis/MODS, CNS injury, respiratory failure, and cardiac issues.
Of the patients who experienced a preventable trauma death with hemorrhage as the cause of death, delayed surgery for hemostasis or radiological intervention was the most commonly mentioned factor in relation to “opportunities for improvements,” followed by delayed blood transfusion. Although not presented in the tables, surgery or intervention could not be performed in 21 patients among those with action taken for hemorrhage as the main cause of death; moreover, 17 patients in whom surgery or intervention were performed, there was a median delay of 2 hours and 56 minutes after admission, in providing hemostatic measures. The medical staff failed to perform hemostatic measures within an hour in all cases except for three cases that occurred in an RTC. This result is consistent with that of a prior report, which showed that delayed hemostatic measures were the most common problem found in relation to preventable trauma deaths, even in mature trauma systems.111415 Coping with deadly traumatic hemorrhages is a very complex process requiring the involvement of many departments. Many previous reports have shown that the occurrence of preventable trauma deaths can be reduced by establishing effective quality improvement.161718 There was a report of a quality improvement case in which the above-mentioned problems were rectified by revising the initial transportation guidelines while transporting severe trauma patients with a potential risk of death from hemorrhage, to a RTC that could perform emergency surgeries or radiological interventions, as well as by educating and training emergency medical care teams with the contents.19 Issues related to blood transfusions were found in many patients who experienced preventable trauma deaths; in six patients, the medical staff failed to perform transfusions until the patient's death. Even when performed, it was substantially delayed, with a median time of 64 minutes. This may be due to a lack of provision of emergency transfusions and the need for massive transfusion protocols in facilities other than RTCs.20 The lack of this type of protocol can have a grave impact on treatment outcomes in those with severe traumatic hemorrhages. Therefore, designated trauma centers must have detailed protocols.21 A recent study at Penn Medicine Lancaster General Health in 2016 evaluated opportunities for improving the massive transfusion protocol when 11 patients were found to have massive transfusion problems. Therefore, a standard training procedure known as crew resource management (CRM) was implemented, which was associated with decreased mortality.22 The concept of CRM, originally established for the aviation industry quality management attributes most mistakes to the lack of communication and coordination rather than personal error. The CRM approach could be used to solve problems that occur during transfusion processes. In addition, this type of problem solving may need to include a more detailed massive transfusion protocol.2324
In the case of sepsis/MODS and CNS injury—the second and third most common causes of death after hemorrhage, respectively—delays in treatment at the hospital stage were identified as major OFIs. Regarding cases of sepsis/MODS, the development of corrective action plans should focus on the proper and timely identification and removal of sources of infection that may lead to sepsis. These sources include contamination in the early period that originated from the trauma itself and secondary infections in the late stage that were developed during intensive care. Traumatic brain injury was the main cause of death of all CNS injury patients. In these cases, delay in craniotomy was identified as a major OFI from the review of preventable trauma deaths caused by subdural or epidural brain hemorrhage requiring emergency craniotomy. When craniotomy was performed, the average time until craniotomy after arriving at the final destined hospital was more than double of that recommended by the WHO guidelines for trauma quality improvement programs (“within 4 hours”).1 In fact, when considering the time spent in the process of transfer before arrival at the final destined hospital, this delay becomes even longer and more serious. Furthermore, 43% (6/14) of CNS injury patients died before craniotomy could be performed. Therefore, reducing the delay in craniotomy is one of the most urgent OFIs identified during the process of early trauma resuscitation that should be addressed to reduce preventable trauma death rates.
This study has some limitations. First, we conducted this study using data from an administrative district of Korea; therefore, the generalization of our results to the entire country would be limited, even though the studied region is one of the largest and most populated provinces in Korea. Second, the retrospective study design precluded the analysis of unrecorded factors or missing values. Third, the evaluation of “preventability” relied entirely on the analysis by expert panels, which has limitations in objective reproducibility, although the Cohen’s Kappa index indicated fair reliability similar to that in previous studies.425
The regional preventable trauma death rate in Gyeonggi Province in 2017 was found to be 17.0%. Although this is an improvement from that found in prior studies, many problems were discovered in the inter-hospital transfer stage and hospital stage in emergency medical care facilities other than an RTC. Further, several OFIs regarding bleeding control were identified. To address this, close cooperation among the existing RTCs, other emergency medical care facilities, 119 EMS, and local governments is crucial, and an inclusive regional trauma system needs to be established to enhance further advances in trauma care.
 XML Download
XML Download