

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) cases in the world are 17,507,359 as of July 31, 2020.1 Korea has about 52 million population, 18% of which is a pediatric population ≤ 19 years.2 As of July 31, 2020, 14,305 individuals were confirmed with COVID-19 in Korea. The first pediatric patient was a 10-year Korean girl diagnosed on February 18, 2020.3 As of July 31, 2020, 1,028 Korean children ≤ 19 years have been diagnosed with COVID-19 (21.8 pediatric patients per 100,000 population ≤ 19 years). The proportions of pediatric cases ≤ 19 years and ≤ 9 years are 7.2% and 1.7% of all confirmed cases, respectively by data of the Korea Centers for Disease Control and Prevention (KCDC).4
Respiratory virus infection among school-aged children is an important epidemiologic consideration. Data on severe acute respiratory syndrome coronaviru-2 (SARS-CoV-2) transmission from a pediatric index case to others at school settings are limited. However, it is unclear whether school closures are effective during coronavirus outbreaks due to SARS, Middle East respiratory syndrome (MERS), or especially SARS-CoV-2 of which transmission dynamics appear to be different.
It has been several months since schools are closed in more than 190 countries in the world, affecting 1.57 billion children, about 90% of the world student population. According to the United Nations Educational, Scientific and Cultural Organization (UNESCO), countrywide school closure peaked to 194 countries on April 13, 2020, and it decreased to 40 countries on July 31, 2020.5
Korea also delayed the school opening after winter vacation and closed the schools because of COVID-19 outbreak. However, online and off-line (in-person) school opening proceeded. We reviewed the pediatric epidemiology of COVID-19 according to the timeline of school opening delay and school re-opening using the data of the KCDC, and Korean Ministry of Education (KMOE) website.6
We examined whether school opening led the increase of pediatric COVID-19 cases in Korea, a country that had never been lockdown, only performed varying degrees of social distancing and rigorous contact tracing with rapid testing for early detection.
METHODS
Information on the source of national epidemiology data is described in the Supplementary Data 1.
School opening delay and re-opening policy
Information on the school opening delay and re-opening policies was achieved from the press release by the Korean Ministry of Education (KMOE).7 Online classes opened by using online education platforms such as “EBS Online class” of Korea Educational Broadcasting System (EBS). A decision on the off-line school opening was made in collaboration with KCDC, taking into account the opinions of school teachers, parents, and the Metropolitan and Provincial Offices of Education. Then, the guidelines were released for personal hygiene, infection prevention measures, procedures to follow when suspected symptoms occur in students. In addition, KMOE recommended that the number of students attending classes would not exceed a certain proportion to avoid overcrowding in schools. However, dolbom (day care) classes for young children and elementary students (grade 1–3, G1–G3) were maintained when children could not participate in online classes (e.g., both parents are working).
In the case of high school senior students (G12), they attended the school for off-line classes daily considering the urgent academic need for the university entrance examination.8 Except for G12 students, the number of students who attended off-line classes was determined by the number of confirmed COVID-19 patients in the local area where the schools are located and the size and/or characteristics of each school. Specific recommendations are listed in Table 1. In addition, whenever a confirmed case was identified, the school was closed, and the contacts were subjected to SARS-CoV-2 polymerase chain reaction.789

Table 1
Schedules and method for school attending according to the school situation
G = grade.
aA total number of students in a school is 60 or less; bMore than once a week, one week in-person and two weeks online, etc.
![]()
This study analyzed the data that is publicly available from the reports by KCDC and policy announcement by KMOE. Data of exposure in school or kindergarten were collected by KCDC and KMOE daily press released report. Details of how they maintained the social distancing among students are described in the Supplementary Data 1 and Supplementary Fig. 1.47
RESULTS
Epidemiology of COVID-19 in Korea
As of July 31, 2020, 1,563,796 (3.1%) persons were tested for SARS-CoV-2, and among those tested, 14,305 (0.9%) individuals were confirmed with COVID-19 (27.6 patients per 100,000 population). Korea implemented varying degrees of social distancing strategies with rigorous contact tracing and rapid testing on any suspected cases. Table 2 also shows the total cumulative confirmed cases and daily number of new cases.

Table 2
Epidemiology of COVID-19 in Korea by mitigation strategies
![]()
The first community transmission case was diagnosed on February 16, about four weeks from the first imported patient on January 20. In addition, the heralding case for the large outbreak related religious group was identified on February 18. This led the investigation of a religious group related massive outbreak in Daegu metropolitan area and Gyeongsangbuk-do (province) in February and March 2020, and daily number of new cases were recorded as high as 813 patients on February 29 (Fig. 1 and Table 2).410
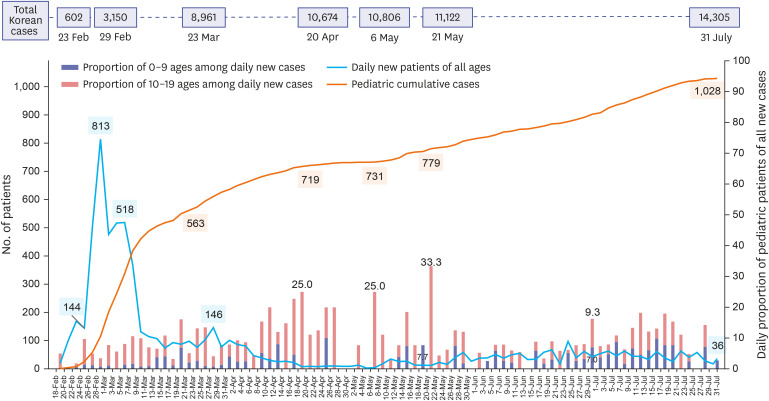
Fig. 1
Epidemiology of pediatric patients with COVID-19 in Korea from February 18 to July 31, 2020. Total numbers of confirmed patients on each date are also shown (black squares). The number of daily new cases of all ages including adults (grey line), the cumulative number of pediatric cases (≤ 19 years old) (blue line), and the proportion of pediatric patients of all daily new cases (yellow and green bars) are shown.
COVID-19 = coronavirus disease 2019.
![]()
Korean government raised the alert level from orange to red on February 23, and executed social distancing (level 2) on February 29. And the government further recommended enhanced social distancing (level 3) on March 23 (Table 2). On April 20, with the relative control of the daily outbreaks in the nation, the distancing level was reduced from enhanced social distancing (level 3) to social distancing (level 2). On May 6, the number of daily new confirmed cases were two, (the number of daily new patient is under ten for 3 days), and dynamic social distancing (level 1) was started (Table 2).
The Korean government never closed the border to other countries or executed the lockdown strategy to control the outbreak of the nation. However, additional various measures were implemented for international visitors or returning Koreans from abroad, and COVID-19 diagnosis and treatment are provided to all individuals also with foreign nationality free of charge as same as Koreans. More information is described in Supplementary Data 2.
School closure and opening delay according to the evolving stages of COVID-19 epidemiology in Korea
Fig. 1 shows the cumulative number of pediatric cases from February 18 to July 31 and a proportion of pediatric patients of the daily new patients in all populations. It also shows the total number of COVID-19 cases of all ages, including adults on dates when the Korean government implemented a change for social distancing.
During the surge of COVID-19 in Daegu metropolitan area and Gyeongsangbuk-do, the number of pediatric cases also rose abruptly as adult cases from one pediatric case on February 18, and 522 cases on March 17 when the third school opening delay was announced. Many older adolescents were also related to the religious group in those areas. Although the pediatric numbers rose rapidly in February and early March, since the number of daily new patients of all ages was so high, the proportion of pediatric patients seemed relatively low.10
With this epidemic situation, the KMOE decided to delay the school opening for the new school year, which usually starts on March 2 every year. Eventually, the school openings were delayed three times in Korea (Table 3). The first delay was decided when the national alert level was lifted from orange to red on February 23, because of the outbreak surge. The second delay was announced on March 2 after the number of daily new patients recorded 813 on February 29 with the overwhelming outbreak in Daegu. The third delay was decided while further data were being sought, and safety measures were planned to help decision for school opening. The school closure continued until April 6, 2020. Meanwhile, additional mathematical modelling and simulation study on school openings in Korea became available in early April 2020.11 Of note, the proportion of pediatric cases appeared high in mid-April and mid-May. However, the numbers of daily new cases of all populations were maintained at a low level (less than 50 cases per day), and the absolute number of new pediatric cases per day did not significantly increase.4

The impact of school opening on the epidemiology of COVID-19 in the pediatric population up to July 31, 2020
The dates for school openings for students at different grades (online and off-line) are shown in Table 4 and Fig. 2. The number of pediatric COVD-19 patients and the proportions of pediatric patients of all confirmed cases are shown in Fig. 2A and 2B with school opening dates.
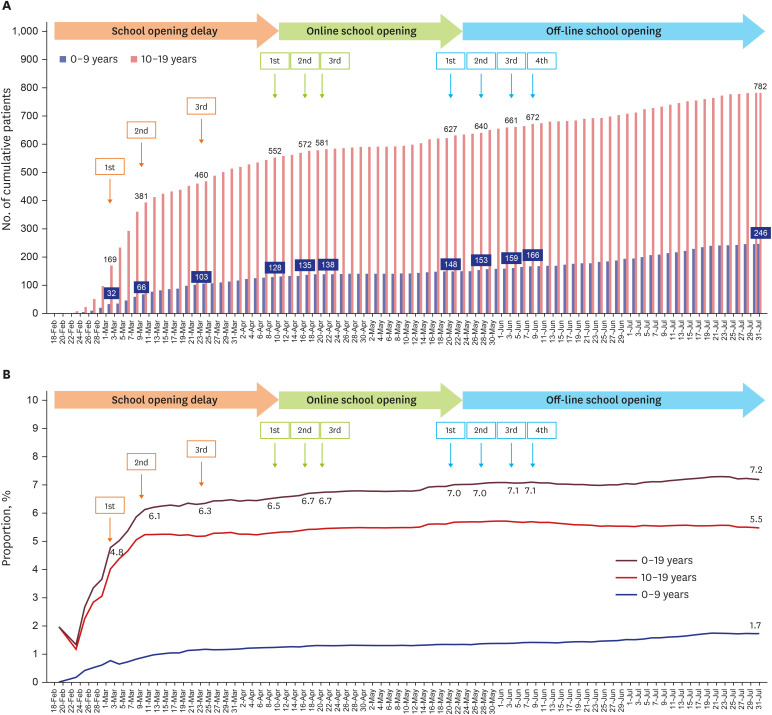
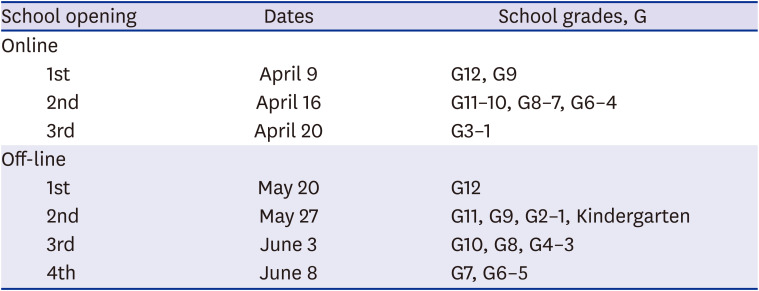
Fig. 2
Pediatric patients (0–19 years) with COVID-19 during school opening delay and re-opening period. (A) Number of cumulative patients. (B) Proportions of pediatric patients.
COVID-19 = coronavirus disease 2019.
![]()
Table 4
Step-wise school opening online and off-line in Korea during COVID-19 pandemic in 2020
In Korean education system, children in G1–G6 are in elementary schools, students in G7–G9 in middle schools, and students in G10–G12 are in high schools.
COVID-19 = coronavirus disease 2019.
![]()
Online classes started three steps on April 9, April 16, and April 20, with high school senior students (12th grade, G12) and middle school senior students (9th grade, G9) first. As of April 9, the number of total confirmed cases in all ages was 10,423 (20.1 patients per 100,000 population), and the number of pediatric COVID-19 cases (≤ 19 years) was 680 (6.5% of all confirmed cases).4
Off-line (in-person) classes started at four steps on May 20, May 27, June 3, and June 8 with high school senior students (12th grade, G12) who went to school first in the 2020 school year. As of May 20, the number of total confirmed cases in all ages was 11,110 (21.4 per 100,000 population), and the number of pediatric COVID-19 cases (≤ 19 years) was 775 (7.0% of all confirmed cases). As of July 31, 72 days from the first off-line opening, the number of pediatric COVID-19 cases (≤ 19 years) was 1,028, and the proportion of pediatric patients of all confirmed cases was 7.2%.4
There was no obvious trend for the sudden increase of pediatric cases or the proportion of pediatric cases of all confirmed cases in the nation before and after the off-line (in-person) school opening until July 31 when most schools started summer vacation.
SARS-CoV-2 exposure at school setting after off-line (in-person) opening
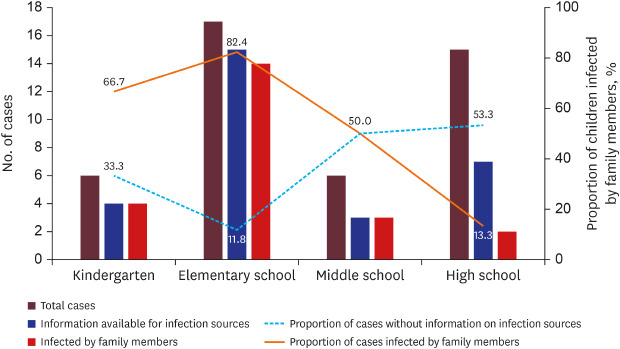
Table 5 and Fig. 3 summarize SARS-CoV-2 exposures and investigation at schools where a pediatric case was the index case at the school since the off-line school opening on May 20. As of July 31, 44 children (index students) attended 38 schools and kindergartens and exposures occurred in other students and staff members: 14 high schools, six middle schools, 13 elementary schools, and six kindergartens. Among 44 pediatric cases, 29 (65.9%) cases were available for the source of infection, 23 cases (79.3% of cases with infection source identified, 52.3% of total cases) were infected by their family members. One case was from the church outbreak, and five students were from the acting academy outbreak.
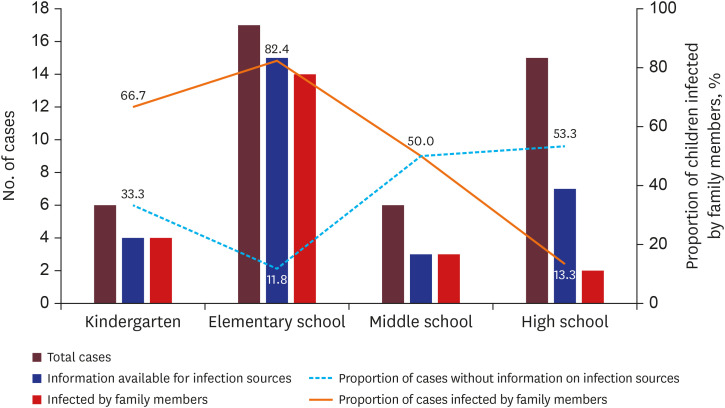

Fig. 3
Number of pediatric patients in each school setting and information availability for infection sources.
![]()
Table 5
Summary of SARS-CoV-2 exposures by index students at schools and kindergarten after school re-opening
Data are presented as number (%).
SARS-CoV-2 = severe acute respiratory syndrome coronaviru-2.
aAdditional 1,071 individuals tested because of exposures from two brothers in the same family, one was an elementary school student, and the other was a middle school students.
![]()
At kindergartens, four children (4/6, 66.7%) were infected by their family members, and the information on the source of infection was not available in two children. More than 800 children and staff members in the kindergartens were tested for SARS-CoV-2. There were no secondary cases from kindergarten exposures (Table 5 and Supplementary Table 1).
At elementary schools (G1–G6, 7–12 years), 17 cases were confirmed, and more than 3,000 students and staff members were tested. Among the 17 cases, the source of infection was available in 15 (88.2%) cases, and 14 students were infected by the family members (82.4%). There was only one elementary school where the secondary cases were observed; one 11-year-old child in the 5th grade transmitted the virus to two other children. One child was infected in the same classroom, and the other was not in the same class but was infected at the same exercising gym (Table 5 and Supplementary Table 1).78121314
At middle schools (G7–G9, 13–15 years) and high schools (G10–G12, 16–18 years), 21 students were confirmed, and more than 7,500 students and staff members were tested. In middle school exposures, among six adolescents, three were infected by family members (3/6, 50.0%). In high schools, only two adolescents were infected by family members (2/15, 13.3%). There were no secondary cases from middle school and high school exposures (Table 5 and Supplementary Table 2). Of note, five students (G12) from four different high schools were infected at the same acting academy in Daegu. In the academy, they practiced acting and singing for their university entrance examination without wearing a mask. However, they did not transmit SARS-CoV-2 in their own school where they followed the rules for distancing among students and wearing a mask.13
The proportions of index students who did not have information on infection sources were higher in older age groups (middle school and high school students) than in younger age groups (kindergarten and elementary school students) (52.4% vs. 17.4%, P = 0.014). In the younger age group, almost 80% of children were infected by family members, but the proportion of students infected by family members decreased with age (P < 0.001) (Fig. 3).47
Discussion
This report describes the impact of school opening on pediatric COVID-19 epidemiology in Korea. There was no significant increase in the number of pediatric patients or the proportion of pediatric patients among all confirmed cases in the nation after the off-line (in-person) school opening. School opening did not cause significant school-related outbreak with good adherence to safety measures for symptom monitoring, personal hygiene, wearing masks, and distancing among students.
Closing and re-opening of schools and preschools is a major educational, political, and a public health issue worldwide. There are concerns about the transmission of the virus among children and teenagers in the closed space of the school. However, the negative impact of limiting social and physical activities for an extended period in children is worrisome. In addition, significant inequalities among children with a high- and low-socioeconomic environment may exist in online learning accessibility and the level of care provided at home with prolonged school closure.
It is well-known that children are susceptible to many respiratory viral infections with frequent epidemics in the communities. Therefore, there were questions about the role of the pediatric population for the spread of the SARS-CoV-2. However, early transmission clusters were identified mainly from adults, making children less likely to be index cases in households or the communities. As data accumulated, a significant proportion of pediatric patients are known to be asymptomatic or mildly symptomatic, with an exception for unusual cases with multisystem inflammatory syndrome in children (MIS-C).1516 In addition, pediatric patients with COVID-19 also appeared to have similarly high viral loads at the early stage of illness as in adult patients.171819 Therefore, the possibility for virus transmission from pre-symptomatic or mildly symptomatic pediatric index case(s) to others can also be questioned.1920
However, there are limited data that reported the transmission among children that led to a large outbreak, especially in school exposure. A systematic review also suggested that children seem unlikely to be the main drivers of the COVID-19 pandemic.21 It is not clear whether the viral transmission dynamic in the pediatric population is different from that of adults, or this may be simply because most schools are closed for extended periods. There may be certain different features in the pediatric population that need to be further explored.
It is of interest that of more than 13,000 students and staffs tested from 38 schools and preschools, only one additional student was infected in the same classroom at the elementary school. Based on our data, we consider that spread of COVID-19 within Korean schools has been very limited even after off-line classes started while following the rules for symptom monitoring and distancing among students. Since rigorous contact tracing and tests have been performed in Korea from the early phase of pandemic, there is little possibility that there are hidden pediatric cases. In addition, a recent seroepidemiological survey reported that only 0.03% of tested positive for SARS-CoV-2 antibody among 3,055 Koreans.22 Therefore, we consider that transmission among children at school appears to be very low and what we observed in this study would represent the real situation of the Korean pediatric population.
Transmission from a pediatric index patient to others (children or adults) and susceptibility of children, when exposed to infected index case (children or adults), may be different from that of adults. The secondary attack rate from the index pediatric patient of the household has been reported as low as 0.5% (0 to 2.6%) in Korean data.23 In addition, low angiotensin-converting enzyme 2 (ACE2) gene expression was observed in nasal epithelium of children relative to adults.24 These findings may help explain why COVID-19 is less prevalent in children.
It is of note that the infection sources were more likely available in the younger age group (kindergarten and elementary school) than the older age group. When the information on infection source was available, the majority of the younger children were infected by family members. In a study from China, they also reported that 90.1% of 171 pediatric cases were related to family clusters.25 In a study from Switzerland on 40 pediatric cases, they investigated the dynamics of infection in their families; one or more adult family member was suspected or confirmed for COVID-19 before symptom onset of the study child in 79% of households.26 Therefore, the most common infection sources for pediatric cases appear to be their adult family members; children are not the primary source of infection or did not cause large outbreaks at school.2728 Careful attention should be paid to older adolescents who may have more sources of infection outside of the household.28
There are some limitations to this study. First, our epidemiologic data are not complete since our data were collected from publicly available press releases without detailed epidemiologic information. Second, we only analyzed the situation when the index patient was a student and did not examine the situation when the index patient was an adult staff. However, overall, there were no large school outbreaks after in-person school opening in both situations when exposures occurred after a student or an adult staff was identified as the index at school. Third, we could not analyze the data in detail by the region, which could be added in the future study. Finally, the data mainly contained numbers of the confirmed cases and exposed individuals who were tested, but detailed epidemiologic investigation data was insufficient. However, we tried to fill up the data as much as possible by follow-up data search when the additional information was released on any additional student cases (either yes or no) in the same school of the index student.
Although there are several reports from the school exposure investigation in various countries,2930 there has been limited report that systematically described national progress on school closure, online opening, and off-line opening with an epidemiological analysis based on all the reported numbers of the total national pediatric population.
Of note, Korea had the second wave of a large outbreak in mid-August and mid-September, which caused the school opening delay at the end of summer vacation and transient school closure. However, this time, G12 students continued to go to school, and the school opened again for off-line (in-person) classes within one month. This was quite different from March to May situation when the school reopened again after 72 days for all students. The pediatric proportion of all confirmed cases remained stable, and most of all, there were no school-related outbreaks that led the nation-wide school closure again.
In conclusion, Korea had a successful transition from school closure to re-opening for online and off-line (in-person) classes with various efforts to keep our pediatric population safe while they attend the school during COVID-19 pandemic. More information will be needed on whether, compared to adults, children are less susceptible to SARS-CoV-2 when exposed, or less capable of transmitting the virus to others when they are the primary cases. Impact of school opening in various epidemiological situation in the community (low level vs. high-level transmission) needs to be carefully examined with the degree of adherence to the school guideline related to COVID-19.
 XML Download
XML Download