

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Periprosthetic joint infection (PJI) is a devastating complication after total joint arthroplasty (TJA).123 It is a serious challenge for individual patients as well as the health care system. Extensive efforts; preoperative screening of patients at risk of PJI, mitigation of the risk factors, medical preparation, use of prophylactic antibiotic, clean environment of operating room and optimized surgical strategies, have been made continuously to prevent PJI.4567810 Despite these efforts, the rate of PJI has not reduced a lot.11 Reportedly, the nationwide incidence of PJI was 2.0 to 2.7% in the United States1213 and 1.6% in Canada.14 The number of TJAs has been increased worldwide due to the global trend of aging.1516 Studies from North America showed continuous increase of PJI incidence in accordance with the increment of TJAs.121718 Between 2000 and 2013, the percentage of revision total hip arthroplasties (THAs) due to PJI increased from 10.9% to 13.7% in the United States.19 PJI is a tremendous burden for individual patients and surgeon as well as healthcare system.2021222324
Once occurred, PJI usually requires prolonged antibiotic treatment and multiple surgical interventions.2 Medical costs were significantly greater for infected joint arthroplasties than for uninfected arthroplasties.2526
Even though awareness of nationwide PJI incidence is of utmost importance to establish medical policies for PJI in each country, there have been no nationwide studies on the epidemiology and economic burden of PJI in East Asia.
The purpose of this study was to evaluate the incidence rate and medical cost of PJI in Korea and to project the future incidence using a nationwide medical claim database.
Go to : 
METHODS
Data sources and collection
We analyzed the Korean Health Insurance Review and Assessment (HIRA) database from 2010 to 2018 for an epidemiological investigation of PJI in Korea. In Korea, almost all citizens (97%) are obligated to register into the Korea National Health Insurance Program (KNHIP). Patients pay an average of 30% of the total medical costs to clinics or hospitals that manage almost all diseases, except for cosmetic surgery or some new unproven therapies, which not covered by the insurance. All medical institutions in Korea submit claims with data including basic demographics of patients, diagnoses according to International Classification of Diseases 10th revision (ICD-10), procedures including operation, prescription records and the medical cost of each procedure to the HIRA to reimburse 70% of the total medical cost. The whole medical costs of the remaining 3% of the Korean citizens, who are registered into the KNHIP, are paid by a medical aid program of the government. The data of the patients covered by the medical aid program are submitted to HIRA in the same manner as KNHIP. Thus, it is possible to extract every medical data of almost whole Korean patients from the HIRA database, which have been used in previous epidemiological studies from Korea.272829303132
We identified annual numbers of primary THAs, total knee arthroplasties (TKAs) and PJIs during the 9-year period. The procedure codes of N0711/N2070 and N2072/ N2077 were used for the identification of THAs and TKAs, respectively. And, diagnostic codes of T845 and T847 were used to identify PJIs.3334
Based on the identified annual numbers, the annual PJI/TJA ratio was calculated. From the medical claim data, the hospitalization cost of PJI at each patient was obtained.
Medical cost of PJI in Korea
We identified the total hospitalization cost of PJI patient at each year from the medical claim data. Subsequently, average cost per PJI patient was obtained in each year.
Future projection of PJIs
We obtained projected number of Korean population through 2030 from the Korean Statistical Information Service (KOSIS) (http://www.kosis.kr), which is the central government organization for statistics.35 From the calculated PJI incidence, future burden of PJI was projected using Quasi-poisson regression model. R software version 3.6.3 was used for the projection and statistical analyses.
Ethics statement
This study was approved for exemption by Institutional Review Board of the Seoul National University Bundang Hospital (SNUBH X-1910-568-908).
Go to :
RESULTS
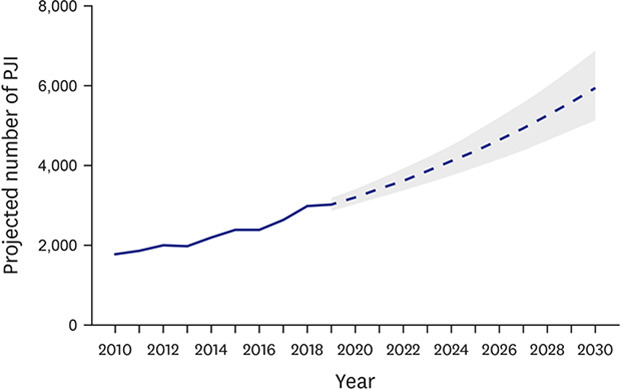
From 2010 to 2018, 87,213 primary THAs and 706,297 primary TKAs were done, and 20,249 PJI patients were treated in Korea. During the 9-year period, the annual volume of TJA increased from 72,766 to 106,933, and the annual number of PJI increased from 1,786 to 2,989 (Fig. 1).

Even with the increments in TJA volume and the PJI number, the PJI/TJA ratio remained stable between 2.3% and 2.8% (Table 1).

Table 1
Number of total joint arthroplasties and periprosthetic joint infections with their ratio in Korea from 2010 to 2018
THA = total hip arthroplasty, TKA = total knee arthroplasty, TJA = total joint arthroplasty, PJI = periprosthetic joint infection.
![]()
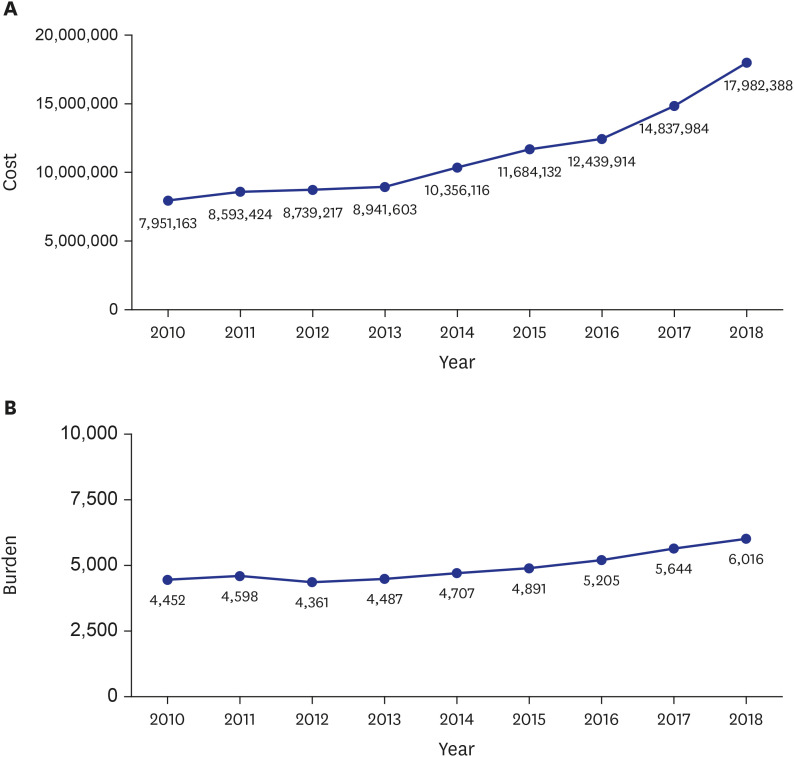
Total annual cost of PJI treatment increased during the 9-year period (Fig. 2A). Total nationwide cost increased from $7,951,163 in 2010 to $17,982,388 in 2018. The mean cost for each PJI patient was $4,452 in 2010 and $6,016 in 2018 (Fig. 2B).
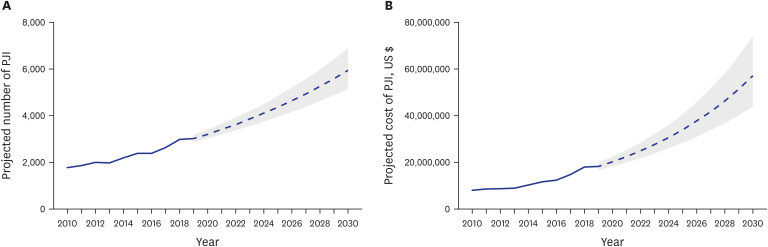
The number of PJIs was projected to be 5,944 (95% confidence interval, 5,133–6,883) in 2030 (Fig. 3A). The total cost of PJI treatment was projected to be $57.0 million (95% confidence interval, $ 44-74 million) in 2030 (Fig. 3B).
Go to :
DISCUSSION
PJI is the most serious complication after TJA and a growing economic challenge.18 Kamath et al. analyzed Nationwide Inpatient Sample (NIS) data of 235,857 revision THA and 301,718 revision TKA procedures.36 In their study, PJI was the most common reason for revision TKA (25%) and the third common reason for revision THA (15%) in the United States. It was the most common reason for major severity of illness in revision TJA. The revision procedures for PJI had the longest length of hospital stay, and the medical costs of revision for PJI were the second highest next to periprosthetic fracture. Though strenuous endeavors and researches were done in past 2 decades, there was no substantial improvement in the success rates of PJI treatment.37 More effective strategies for PJI prevention and novel techniques for treating PJI are warranted.
Several studies from the United States reported the incidence, medical cost and future burden of PJI using nationwide database.1213 Kurtz et al.12 characterizes the patient and clinical factors influencing the economic burden of PJI in the United States using the 2001 to 2009 NIS data. In their study, the PJI incidence ranged between 2.0% and 2.4% of TJAs and steadily increased over time and the annual cost of revisions for PJI increased from $320 million to $566 million during the study period. According to the increment of demand for TJI, the economic burden of PJI was projected to exceed $1.62 billion by 2020.
Bozic et al.13 differentiated the number of patients, respective demographic trends, the indications for revision, patient severity of illness scoring and resource utilization including cost and hospitalization between 235,857 revision THAs and 301,718 revision TKAs using the NIS data between October 2005 and December 2010. In their study, the incidence of PJI was 2.79% in THA and 2.66% in TKA. Revision TKAs increased by 39%, while revision THAs increased by 23%. Patients undergoing revision THAs were older than those undergoing with revision TKAs. PJI (25%) and mechanical loosening (19%) were two most common reasons for revision TKA compared with dislocation (22%) and mechanical loosening (20%) for revision THA. Patients undergoing revision THA were sicker than those undergoing revision TKA (> 50% major severity of illness score versus 65% moderate severity of illness score). Mean length of hospital stay was longer and mean hospitalization costs were slightly higher for revision THAs than for revision TKAs. PJI and periprosthetic fracture were two most common reasons for prolonged hospitalization high costs for revision THAs and TKAs. The revision burden for THA was greater than for TKA by 52%, but revision TKAs were increasing at a faster rate (Table 2).

Table 2
National burden of periprosthetic joint infection in the United States and Korea
| Author | Country | Database | Study period | No. of TJA | No. of PJI |
|---|---|---|---|---|---|
| Kurtz et al.12 | USA | NIS | 2001–2009 | 575,368 → 1,007,523 | 11,658 → 21,964 (88.4%, ↑) |
| Bozic et al.13 | USA | NIS | 2006–2010 | 704,938 → 924,856 | 111,778 |
| Current study | Korea | HIRA | 2010–2018 | 72,766 → 102,963 | 4,204 → 6,928 (64.8%, ↑) |
NIS = Nationwide Inpatient Sample, HIRA = Health Insurance and Review and Assessment, TJA = total joint arthroplasty, PJI = periprosthetic joint infection.
![]()
There might be ethnic and regional differences between Western countries and East Asian countries in the incidence and economic burden of PJI. Nevertheless, there was a paucity of study on the burden and future projection of PJI in East Asia. Only one study assessed 140 revision TKAs and 4,047 primary TKAs performed at 5 centers in Hokkaido, Japan from 2006 to 2011.38 In that study, the revision burden of TKA was 3.3%. The most common reason for revision TKA was mechanical loosening (40%). Other reasons were PJI (24%), wear/osteolysis (9%), instability (9%), implant failure (6%), and periprosthetic fracture (4%). The male proportion in PJI patients was higher than in primary TKA patients (33% versus 19%).
To the best of our knowledge, our study is the first study on the nationwide burden of PJI from East Asia. In this study, the PJI burden of Korea was comparable with that (2.0%–2.7%) of the United States, even the heterogeneity of study design.1213 The burden is also increasing along with the increase of aged population and their demand of TJA in Korea (Table 1).
Two studies estimated the economic burden of PJI in the United States. Brochin et al. assessed hospitalization cost of PJI in THA revisions and total knee arthroplasty revisions using NIS data.3334
In 2018, Brochin et al.33 extracted data on revision THAs from the 2003-2013 NIS database and assessed PJI prevalence and hospitalization costs. Overall PJI prevalence was 15.0%. Adjusted prevalence increased from 13.1% in 2003 to 16.4% in 2013, while adjusted median PJI hospitalization costs increased from $28,240 in 2003 to $31,529 in 2013. The stratified analyses showed that PJI prevalence increased from 13.0% in 2003 to 17.4% in 2013. Similarly, hospitalization costs for the PJI increased by 14% from a median of $27,490 in 2003 to $31,312 in 2013.
Another study from the same institution assessed trends and hospitalization costs of revision TKAs from the 2003-2016 NIS database. Overall prevalence of PJI after TKA was 25.5% and the prevalence had slightly increased from 25.3% in 2003 to 28.9% in 2016 (P < 0.001). The median hospitalization costs for PJI revision decreased slightly from $23,247 in 2003 to $20,273 in 2016, while median cost per-day slightly increased from $3,452 in 2003 to $3,727 in 2016, probably due to decreasing length of stay. The lowest prevalence was seen in small (≤ 299 beds) hospitals (22.9%) and the highest prevalence in urban teaching hospitals (27.3%). In stratification analyses, PJI prevalence increased in larger (≥ 500 beds) hospitals from 24.4% in 2003 to 30.7% in 2016, while the prevalence decreased in small-sized hospitals. Overall prevalence of PJI in revision TKAs appeared to be slightly increasing. The authors suggested that the increasing trends in large hospitals and decreasing trends in small-sized hospitals was due to a shift in the PJI patients from small to large volume hospitals. The decreasing trends in total costs, even with increasing trends in per-day costs were due to a strong impact of shortened length of stay and a more efficient treatment over the years. In these two studies, the median hospitalization cost of the PJI was more expensive than that of Korea by 4.6–7.2 folds.
This study has a strength of reliability because all the data was derived from HIRA database, which enrolled almost all Korean citizens and precluded any selection bias.
There are several limitations inherent to this study. First, it was a retrospective review of the HIRA database, which did not elicit detailed information such as condition of the PJI patients, causative infecting organisms, type of infection (superficial versus deep), chronicity of infection (acute versus chronic), type of treatments(one-stage versus two-staged revision). Second, it was not evident whether each institution used the MSIS criteria39 for the diagnosis of PJI.
Our study showed the increase of future burden of PJI number and economic cost in Korea. The results would be useful for worldwide estimation of PJI and establishment of healthcare policies of PJI in East Asia.
Go to :
 XML Download
XML Download