

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Breast cancer is the most frequently diagnosed cancer and the leading cause of cancer mortality among women.1 Hormone receptor (HR)-positive breast cancer (estrogen receptor- and/or progesterone receptor-positive) is the most common subtype of breast cancer, comprising about 80% of all breast cancers.2 Over the last decade, aromatase inhibitors (AIs) have been the standard adjuvant endocrine treatment for postmenopausal women with HR-positive breast cancer and metastases.34 AIs have been shown to improve disease-free survival and overall survival compared with tamoxifen therapy alone.56 Furthermore, there is a growing body of evidence supporting the benefit of extending the treatment with AIs beyond the initially recommended five years to up to ten years in patients at high-risk of long-term recurrence, including those with positive axillary lymph nodes.7
AIs control plasma estrogen levels by inhibiting or inactivating aromatase, the enzyme regulating the peripheral conversion of androgens to estrogens.8 Since this conversion is the primary source of endogenous estrogens in postmenopausal women,9 AIs relatively rapidly lower the levels of circulating estrogen.8 At the same time, AI treatment significantly increases the levels of bone turnover markers compared to patients not on treatment, indicating a negative bone balance caused by severe estrogen depletion.10 AIs result in significantly higher bone loss than the physiologic postmenopausal bone loss711 and increase the risk of osteoporotic fractures.1213 In a meta-analysis13 of seven trials comparing AIs with tamoxifen in postmenopausal women with early-stage breast cancer, AIs significantly raised the risk of bone fractures (7.5% vs. 5.2% for tamoxifen; odds ratio [OR], 1.47; 95% confidence interval [CI], 1.34–1.61). Once AI treatment is concluded, bone turnover normalizes, and bone mineral density (BMD) and fracture risk can improve in some women.1213 The recent introduction of extended AI therapy has consequently led to growing concerns about the fracture risk in these breast cancer patients.1415
Osteoporotic fractures frequently occur in the vertebrae, hip, wrist, and humerus.16 According to the location, the prognosis and severity of these fractures differ. Although fractures of the spine are frequent, hip fractures have the higher mortality rate among these fractures. While previous study15 showed an increased fracture risk in women taking AI, there is little data on the specific fracture risk for different locations in these patients.
The objective of this meta-analysis was to assess whether AIs affect the risk of osteoporotic fractures in breast cancer patients differently depending on the location.
METHODS
Search methods for the identification of studies
This meta-analysis was carried out according to the updated guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis.17 MEDLINE (PubMed), Embase, and Cochrane Library databases were used to search the studies to August 2020. An overview of the search strategy is presented in the Supplementary Table 1.
Two authors independently screened the titles and abstracts to identify studies on osteoporotic fractures in breast cancer patients treated with AIs. Disagreements were resolved by discussion with a third party to reach consensus. The reasons for ineligibility or exclusion of studies were recorded and described.
Study selection criteria
The systematic review was designed to answer the following question: Does AI treatment affect the risk of osteoporotic fractures differently depending on the location in breast cancer patients? The PICOS18 method was used to define the selection criteria as follows: the P (population) was patients with breast cancer; I (intervention) was treatment with AIs, including anastrozole, exemestane, and letrozole; C (comparison) was patients with breast cancer who did not receive AIs; O (outcome) was the incidence of osteoporotic fractures in specific locations (hip, vertebral, and non-vertebral fractures); and S (study type) was randomized controlled studies only.
The exclusion criteria were as follows: 1) treated osteoporosis, 2) treated with chemotherapy or hormone replacement, and 3) review, case report, or in-vitro study.
Two authors reviewed the retrieved full manuscripts to detect whether the fractures existed after AI treatment in patients with breast cancer. They also examined the reference lists of all potentially eligible studies and review articles to find additional related publications. Articles that met the selection criteria were included in the meta-analysis.
Outcome measures and data extraction
Two authors independently extracted the following data from each included article into predesigned data collection forms in Microsoft Excel (Microsoft Corporation, Redmond, WS, USA): 1) study identification: first author's name, year of publication, and country; 2) study design; 3) participants: sample size; 4) interventions: details about the diagnostic criteria for osteoporotic fracture; 5) primary outcome measure for the meta-analysis was the difference in the incidence of osteoporotic fractures (hip, vertebral, and non-vertebral fractures) between cases and controls. The risk of fractures was also evaluated for the different sites of fractures (hip, vertebral fracture, and non-vertebral fracture); and 6) measuring tools. Disagreements were resolved by discussion with a third party to reach consensus.
Quality assessment and publication bias
Two authors independently evaluated the quality of all studies using the Cochrane Collaboration's tool19 for assessing the risk of bias in randomized trials. Disagreements were resolved in discussion with a third party aimed at consensus.
This tool19 assesses six sources of bias: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other potential bias. Overall risk assessments (high, unclear, and low) were based on the approach presented in the Cochrane Handbook. We evaluated the presence of publication bias using Begg's funnel plot20 and Egger's test.21
Statistical analysis
The primary analysis involved a proportion meta-analysis of the data from all relevant studies that reported the incidence of osteoporotic fractures. For the subgroup analyses according to the fracture location in the spine, hip or other (binary outcomes), the effect sizes were calculated as risk ratios (RR), and the studies were weighted according to the number of included patients.
A fixed-effects or random-effects model was used to quantify the pooled effect size of the included studies, depending on the heterogeneity of the data. Heterogeneity between comparable studies was tested using the χ2 and I2 test; P > 0.1 and I2 < 50%, respectively, were used as established criteria to determine statistical heterogeneity. All statistical analyses were performed using R software (R Foundation for Statistical Computing, Vienna, Austria).22
RESULTS
Description of the included studies
The primary search of the databases yielded 1,116 records. After 145 duplicates were removed, 971 articles were screened by title and abstract. As a result, 146 full-text articles were selected and reviewed for eligibility. A total of 30 studies (117,974 participants) were finally included in the systematic review (Fig. 1 and Table 1).
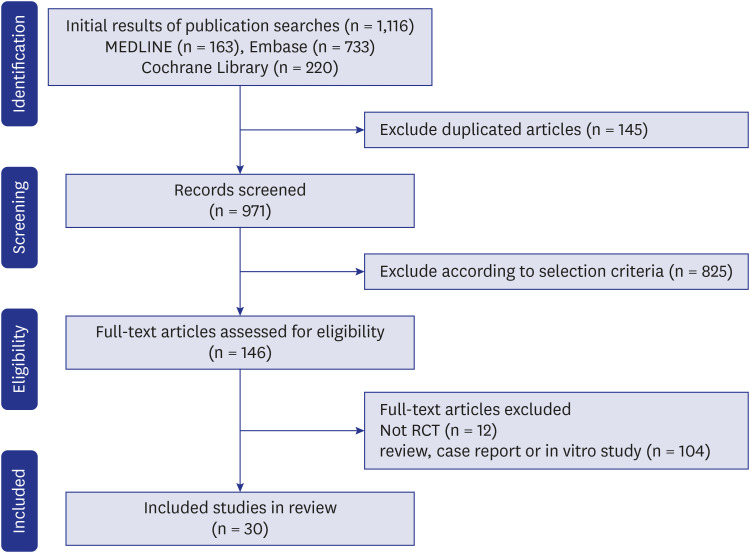
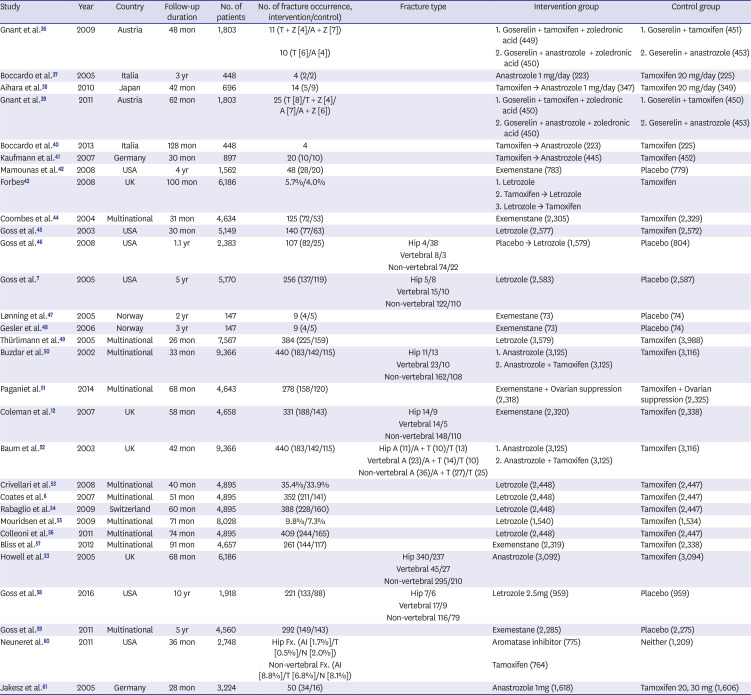
Fig. 1
Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow diagram for the study selection in this meta-analysis of the risk of osteoporotic fractures in breast cancer patients on aromatase inhibitor treatment.
RCT = randomised controlled trial.
![]()
Table 1
Osteoporotic fractures in patients with aromatase inhibitor for breast cancer
| Study | Year | Country | Follow-up duration | No. of patients | No. of fracture occurrence, intervention/control) | Fracture type | Intervention group | Control group |
|---|---|---|---|---|---|---|---|---|
| Gnant et al.36 | 2009 | Austria | 48 mon | 1,803 | 11 (T + Z [4]/A + Z [7]) | 1. Goserelin + tamoxifen + zoledronic acid (449) | 1. Goserelin + tamoxifen (451) | |
| 10 (T [6]/A [4]) | 2. Goserelin + anastrozole + zoledronic acid (450) | 2. Geserelin + anastrozole (453) | ||||||
| Boccardo et al.37 | 2005 | Italia | 3 yr | 448 | 4 (2/2) | Anastrozole 1 mg/day (223) | Tamoxifen 20 mg/day (225) | |
| Aihara et al.38 | 2010 | Japan | 42 mon | 696 | 14 (5/9) | Tamoxifen → Anastrozole 1 mg/day (347) | Tamoxifen 20 mg/day (349) | |
| Gnant et al.39 | 2011 | Austria | 62 mon | 1,803 | 25 (T [8]/T + Z [4]/A [7]/A + Z [6]) | 1. Goserelin + tamoxifen + zoledronic acid (450) | 1. Goserelin + tamoxifen (450) | |
| 2. Goserelin + anastrozole + zoledronic acid (450) | 2. Geserelin + anastrozole (453) | |||||||
| Boccardo et al.40 | 2013 | Italia | 128 mon | 448 | 4 | Tamoxifen → Anastrozole (223) | Tamoxifen (225) | |
| Kaufmann et al.41 | 2007 | Germany | 30 mon | 897 | 20 (10/10) | Tamoxifen → Anastrozole (445) | Tamoxifen (452) | |
| Mamounas et al.42 | 2008 | USA | 4 yr | 1,562 | 48 (28/20) | Exemenstane (783) | Placebo (779) | |
| Forbes43 | 2008 | UK | 100 mon | 6,186 | 5.7%/4.0% | 1. Letrozole | Tamoxifen | |
| 2. Tamoxifen → Letrozole | ||||||||
| 3. Letrozole → Tamoxifen | ||||||||
| Coombes et al.44 | 2004 | Multinational | 31 mon | 4,634 | 125 (72/53) | Exemenstane (2,305) | Tamoxifen (2,329) | |
| Goss et al.45 | 2003 | USA | 30 mon | 5,149 | 140 (77/63) | Letrozole (2,577) | Tamoxifen (2,572) | |
| Goss et al.46 | 2008 | USA | 1.1 yr | 2,383 | 107 (82/25) | Hip 4/38 | Placebo → Letrozole (1,579) | Placebo (804) |
| Vertebral 8/3 | ||||||||
| Non-vertebral 74/22 | ||||||||
| Goss et al.7 | 2005 | USA | 5 yr | 5,170 | 256 (137/119) | Hip 5/8 | Letrozole (2,583) | Placebo (2,587) |
| Vertebral 15/10 | ||||||||
| Non-vertebral 122/110 | ||||||||
| Lønning et al.47 | 2005 | Norway | 2 yr | 147 | 9 (4/5) | Exemestane (73) | Placebo (74) | |
| Gesler et al.48 | 2006 | Norway | 3 yr | 147 | 9 (4/5) | Exemenstane (73) | Placebo (74) | |
| Thürlimann et al.49 | 2005 | Multinational | 26 mon | 7,567 | 384 (225/159) | Letrozole (3,579) | Tamoxifen (3,988) | |
| Buzdar et al.50 | 2002 | Multinational | 33 mon | 9,366 | 440 (183/142/115) | Hip 11/13 | 1. Anastrozole (3,125) | Tamoxifen (3,116) |
| Vertebral 23/10 | 2. Anastrozole + Tamoxifen (3,125) | |||||||
| Non-vertebral 162/108 | ||||||||
| Paganiet al.51 | 2014 | Multinational | 68 mon | 4,643 | 278 (158/120) | Exemenstane + Ovarian suppression (2,318) | Tamoxifen + Ovarian suppression (2,325) | |
| Coleman et al.12 | 2007 | UK | 58 mon | 4,658 | 331 (188/143) | Hip 14/9 | Exemenstane (2,320) | Tamoxifen (2,338) |
| Vertebral 14/5 | ||||||||
| Non-vertebral 148/110 | ||||||||
| Baum et al.52 | 2003 | UK | 42 mon | 9,366 | 440 (183/142/115) | Hip A (11)/A + T (10)/T (13) | 1. Anastrozole (3,125) | Tamoxifen (3,116) |
| Vertebral A (23)/A + T (14)/T (10) | 2. Anastrozole + Tamoxifen (3,125) | |||||||
| Non-vertebral A (36)/A + T (27)/T (25) | ||||||||
| Crivellari et al.53 | 2008 | Multinational | 40 mon | 4,895 | 35.4%/33.9% | Letrozole (2,448) | Tamoxifen (2,447) | |
| Coates et al.6 | 2007 | Multinational | 51 mon | 4,895 | 352 (211/141) | Letrozole (2,448) | Tamoxifen (2,447) | |
| Rabaglio et al.54 | 2009 | Switzerland | 60 mon | 4,895 | 388 (228/160) | Letrozole (2,448) | Tamoxifen (2,447) | |
| Mouridsen et al.55 | 2009 | Multinational | 71 mon | 8,028 | 9.8%/7.3% | Letrozole (1,540) | Tamoxifen (1,534) | |
| Colleoni et al.56 | 2011 | Multinational | 74 mon | 4,895 | 409 (244/165) | Letrozole (2,448) | Tamoxifen (2,447) | |
| Bliss et al.57 | 2012 | Multinational | 91 mon | 4,657 | 261 (144/117) | Exemenstane (2,319) | Tamoxifen (2,338) | |
| Howell et al.23 | 2005 | UK | 68 mon | 6,186 | Hip 340/237 | Anastrozole (3,092) | Tamoxifen (3,094) | |
| Vertebral 45/27 | ||||||||
| Non-vertebral 295/210 | ||||||||
| Goss et al.58 | 2016 | USA | 10 yr | 1,918 | 221 (133/88) | Hip 7/6 | Letrozole 2.5mg (959) | Placebo (959) |
| Vertebral 17/9 | ||||||||
| Non-vertebral 116/79 | ||||||||
| Goss et al.59 | 2011 | Multinational | 5 yr | 4,560 | 292 (149/143) | Exemestane (2,285) | Placebo (2,275) | |
| Neuneret al.60 | 2011 | USA | 36 mon | 2,748 | Hip Fx. (AI [1.7%]/T [0.5%]/N [2.0%]) | Aromatase inhibitor (775) | Neither (1,209) | |
| Non-vertebral Fx. (AI [8.8%]/T [6.8%]/N [8.1%]) | Tamoxifen (764) | |||||||
| Jakesz et al.61 | 2005 | Germany | 28 mon | 3,224 | 50 (34/16) | Anastrozole 1mg (1,618) | Tamoxifen 20, 30 mg (1,606) |
T + Z = Tamoxifen + Zoledronic acid, A + Z = Anastrozole + Zoledronic acid, T = Tamoxifen, A = Anastrozole, A + T = Anastrozole + Tamoxifen, AI = aromatase inhibitor, N = neither.
![]()
Of the 30 studies, only 28 papers reported the incidence of osteoporosis fractures, and only 6 studies reported the incidence of fractures by location (hip, vertebral, non-vertebral). Therefore, 28 studies were included in the meta-analysis of the incidence of osteoporotic fractures in breast cancer patients treated with AIs, and 6 studies were used in the meta-analysis of the location-specific osteoporotic fracture incidence (Table 1).
Incidence of osteoporotic fractures
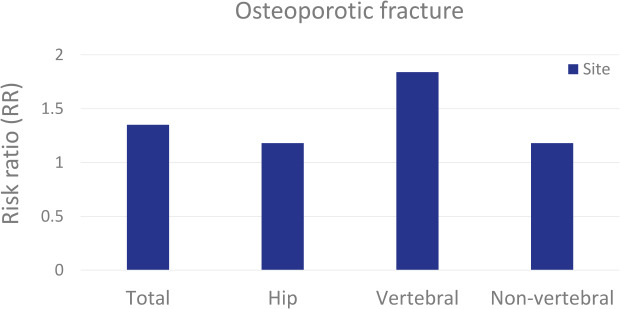
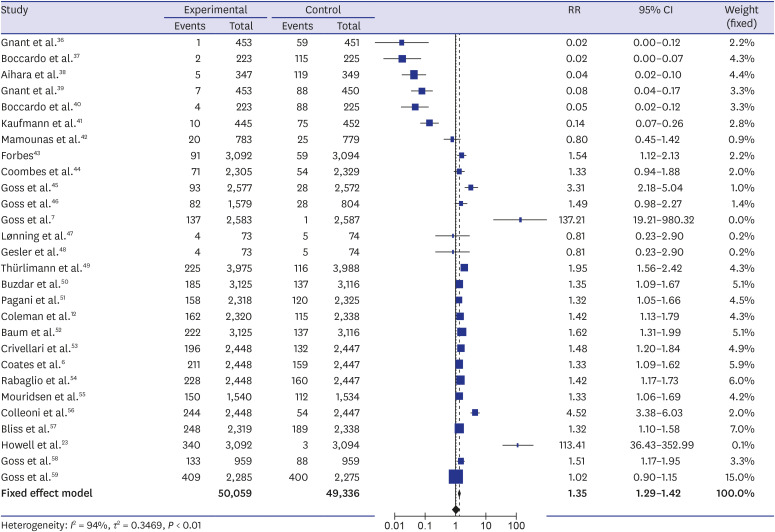
The analysis of 28 studies, involving a total of 99,395 (50,059 cases and 49,336 controls) patients, showed that the incidence of osteoporotic fractures was higher in AI users than that in non-users. The pooled estimate of the crude RR for osteoporotic fractures was 1.35 (95% CI, 1.29–1.42; P < 0.001) (Fig. 2). There was considerable heterogeneity across the studies (I2 = 94%, P < 0.01).
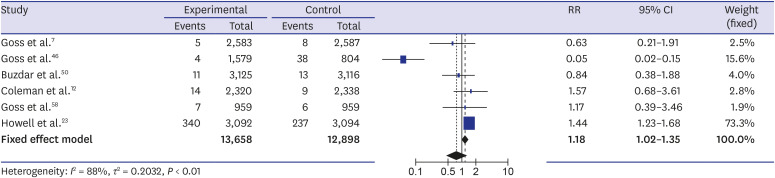
Incidence of osteoporotic hip fractures
The analysis of six studies involving a total of 26,556 (13,658 cases and 12,898 controls) patients showed that the incidence of hip fractures was higher in AI users than that in non-users. The pooled estimate of the crude RR for osteoporotic hip fractures was 1.18 (95% CI, 1.02–1.35; P < 0.001) (Fig. 3). There was considerable heterogeneity across the studies (I2 = 88%; P < 0.01).
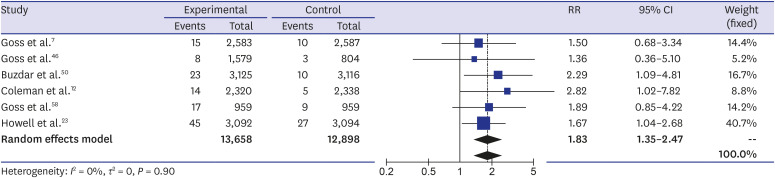
Incidence of osteoporotic vertebral fractures
The analysis of these six studies involving 26,556 (13,658 cases and 12,898 controls) patients showed that the incidence of vertebral fractures was higher in AI users than that in non-users. The pooled estimate of the crude RR for osteoporotic vertebral fractures was 1.83 (95% CI, 1.35–2.47; P < 0.001) (Fig. 4). There was limited heterogeneity across the studies (I2 = 0%, P = 0.90).
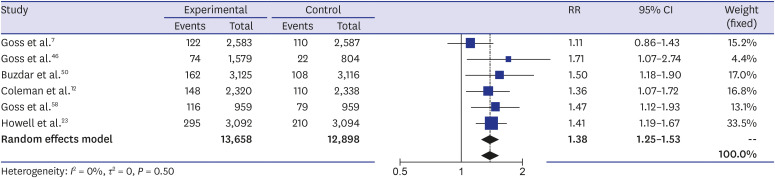
Incidence of osteoporotic non-vertebral fractures
The analysis of these six studies involving 26,556 (13,658 cases and 12,898 controls) patients showed that the incidence of non-vertebral fractures was higher in AI users than that in non-users. The pooled estimate of the crude RR for osteoporotic non-vertebral fractures was 1.38 (95% CI, 1.25–1.53; P < 0.001) (Fig. 5). There was low evidence of heterogeneity across the studies (I2 = 0%, P = 0.50).
Quality assessment and publication bias
The study quality assessment of the included randomized clinical trials by the Cochrane Risk-of-Bias Tool is shown in the Supplementary Table 2. The Begg's funnel plot was symmetrical, and the P values for bias were not significant for all outcomes (Supplementary Fig. 1).
DISCUSSION
This meta-analysis examined whether AI treatment is associated with an increased risk of osteoporotic fractures in patients with breast cancer who are treated with AIs differs depending on the location. It compared the reported occurrence of osteoporotic fractures between breast cancer patients using AIs and those not using AIs. The results show that the risk is highest for vertebral fractures. This complies with the results of previous studies that showed that postmenopausal breast cancer patients with AIs treatment are at increased fracture risk, and patients taking AIs had a particularly high-risk of vertebral fractures.2324
Estrogen deficiency results in an increased number of multicellular bone units and enhanced bone turnover.25 The effects of estrogen deficiency on bone remodeling are primarily mediated through osteoclasts, with greater effects on trabecular than on cortical bone.26 Vertebrae are largely composed of trabecular bone, which is metabolically active and consequently rapidly affected by estrogen deficiency. Therefore, vertebral fractures are the most common osteoporotic fractured in the general population.27 In the United States, about 700,000 vertebral compression fractures are reported each year, which is two times the number of hip fractures.28 Our meta-analysis showed that the risk of vertebral fractures increases compared with hip and non-vertebral fractures in breast cancer patients treated with AIs.
Hip fractures as severe complications of osteoporosis commonly occur in the eighth decade of life, and the average mortality rate within one year is 20%.29 However, a recent study showed that hip fractures in breast cancer survivors treated with AIs occur at an earlier age, result in clinically more relevant functional decline, and happen at a higher BMD than in women with postmenopausal osteoporosis.30 Lee et al.11 also reported that AI treatment in early postmenopausal women with HR-positive breast cancer is associated with a deterioration of proximal hip BMD and geometry, reducing bone strength. In this meta-analysis, we found an increase in hip fractures similar to that study. Hip fractures in younger patients contribute to a deterioration in the functional status and loss of quality of life that leads to a higher socioeconomic burden than fractures in elderly patients.
Non-vertebral fractures are more frequently related to trauma and cause higher mortality rates and costs than vertebral fractures. The incidence of non-vertebral fractures increases rapidly in postmenopausal women.31 In our study, the cause of non-vertebral fractures could not be identified, but the second high-risk was found in women receiving AIs treatment.
Furthermore, the increasing use of extended AI treatment in patients at higher risk of long-term recurrence may be associated with a further increased fracture risk in the relatively young. It is important to identify these high-risk patients and to prevent bone loss in breast cancer patients taking AIs.
Some guidelines on bone health have been published for patients with breast cancer.3233 Recently, seven international societies issued a joined position statement that provides different strategies using a stepwise algorithm.34 The statement suggests that the risk of fractures in women on AIs is comparable to the use of glucocorticoids and recommends a baseline BMD assessment and evaluation of risk factors. Each patient considered for AI treatment should be assessed for their individual fracture risk when treatment is initiated, and this risk should be re-evaluated in adequate intervals.
Pharmacological intervention is recommended for women with a T-score ≤ −2, those with a T-score < −1.5 who have one additional risk factor, and those with at least two clinical risk factors for fractures. It should be combined with vitamin D supplementation and adequate calcium intake. If anti-resorptive treatment is indicated, either denosumab or bisphosphonates are suggested as the first-line treatment to reduce AI-induced bone loss. The treatment of osteoporosis in breast cancer patients should be continued at least until the adjuvant treatment is complete, or even longer in those patients with the highest baseline risk of fracture.35
The strength of our meta-analysis was that we analyzed osteoporotic fractures according to their location. Vertebral fractures occurred more frequently in AI users than in those not using them. However, there were several limitations. First, our study is a literature-based meta-analysis. Thus, we could not evaluate comorbidities and the intake of other medications. Second, because the data were extracted from reports with various follow-up durations, we could not analyze the time that elapses until the occurrence of the first osteoporotic fracture. Third, the inclusion criteria for the studies were different. Some patients received two- or three-year treatment with AIs, while others received AIs for five years before tamoxifen therapy, making the patients included in the meta-analysis a heterogeneous population in this aspect. Regardless, this study establishes the basis for the development of osteoporosis and fracture management in breast cancer patients receiving AI treatment. Fourth, the overall fracture incidence rates in this study were highly variable between studies. Therefore, care must be taken when interpreting the results.
In conclusion, our meta-analysis of osteoporotic fractures under AI treatment of breast cancer confirmed that osteoporotic fractures become more frequent with therapy. In particular, AIs may increase the risk of fractures in breast cancer patients based on the analyzed studies, which were low heterogeneity. Therefore, breast cancer patients using AIs need active fracture prevention and supplemental treatment. Furthermore, larger-scale, high-quality studies reporting the effects of AI treatment on BMD are needed in the future to more accurately determine the influence of AI treatment on osteoporotic fracture risk in breast cancer patients.
 XML Download
XML Download