

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Mental illness is an important risk factor for suicide. Patients with mental illnesses are at three- to twelve-fold greater risk of suicide than the general population.1 In general, psychotic disorder, bipolar disorder, and major depressive disorder are classified as severe mental illnesses (SMI) as they are associated with more severe symptoms and higher risk of suicide compared to other mental illnesses.2 The risk factors for suicide in schizophrenia include sociodemographic factors (age and sex) and clinical factors (depressive symptoms, active hallucinations and delusions, substance abuse).3 Suicide in bipolar disorder is influenced by early onset of the illness, polarity of current episode, episode severity, history of suicide attempts, family history of suicide, and comorbidities.45 For major depressive disorder, both young and elderly patients, male patients, and those who are comorbid with anxiety disorder, substance misuse, or somatic disease are at higher risk of suicide.6 Substance abuse,7 personality disorder, and chronic pain8 are among the most frequent psychiatric comorbidities in suicidal patients, including those who are diagnosed with non-SMI.91011
Suicide is one of the major public health issues in Korea. The one-year incidence of suicide among the general population in Korea was 26.6 cases per 100,000 people in 2018,12 the highest among member countries of the Organization for Economic Co-operation and Development (OECD)—more than twice the OECD average of 11.2.13 Suicide is the fourth most common cause of death in Korea,14 and deaths through self-harm have increased from 2002 to 2015.15 Evidence suggests that suicide in Korea is closely related to mental illness.161718 According to nationwide statistics on the causes of suicide in 2018,19 31.6% of suicide deaths were caused by psychiatric problems. In addition, as per a previous study on suicide attempters visiting an emergency room (ER), psychiatric problems constituted the main cause of suicidal behavior for 62.2% of the suicide attempters.16 Another study on patients referring to the ER due to suicidal attempts revealed that patients with schizophrenia and anxiety/somatoform disorders engaged in more serious suicide attempts compared to patients with other psychiatric disorders, which were closely related to suicide completion.20
The purpose of this study was to compare the risk of suicide of mentally ill people compared to the general population. To the best of our knowledge, although there have been many studies on suicide, no study has yet examined suicide among all psychiatric patients including inpatients, outpatients and those visiting ER in Korea. We hypothesized that differences exist among psychiatric diagnoses and that there are modifying factors such as comorbidities, age, and sex.
METHODS
Participants
All patients who visited the psychiatric outpatient clinic, were hospitalized, or visited emergency departments at least three times at Seoul National University Hospital (SNUH) between March 1, 2003 and December 31, 2017 were recruited in this study. Patients' demographic characteristics at the first visit, date and diagnosis at the latter, and their follow-up data were collected from electronic medical records (EMR) of the hospital. Electronic medical system was implemented in SNUH in 2003, and subsequent medical information could be extracted into processed Excel files through SUPREME (https://supreme.snuh.org), a server that integrates and stores EMR data, and provides patient information that satisfies when a researcher enters conditions. According to the counting system of the hospital administration department, when a patient was hospitalized directly from the emergency department, but discharged on the same day due to withdrawal of consent, the number of visits was counted as two, although no medical care has been given. Thus, to assure the comparability of the data across the sample, only patients who visited thrice or more were included.
We integrated the hospital data extracted as above with the nationwide death data from Statistics Korea. Mortality information reported before December 31, 2017 was extracted from the National Statistical Database through the personal information security team of the hospital. The data were merged with the EMR, excluding social security numbers, in order to protect the participants' personal information. Participants were divided into two groups: suicidal deaths vs. survivors or non-suicidal deaths. The cause of death was assigned following the International Classification of Diseases 10th revision (ICD-10).21 Cases of which the cause of death was coded X60–X84 or Y87.0 were included in suicidal deaths group, as in previous research.2223 Cases without data reporting their death or of which the cause of death was not X60–X84 or Y87.0 were classified in the comparator group, i.e., survivors or non-suicidal deaths.
Diagnosis
The diagnosis used for this study was the patients' main diagnoses after the first visit, as recorded in the EMR. Based on ICD-10, the following eight psychiatric diagnoses groups were considered: psychotic disorder, schizophrenia, schizotypal, and delusional disorders (F20–F29); bipolar disorder, manic episode, or bipolar affective disorder (F30 or F31); depressive disorder, depressive episode, recurrent depressive disorder, or persistent mood (affective) disorders (F32, F33, or F34); unspecified mood disorder or unspecified mood (affective) disorder (F39); anxiety disorder and neurotic, stress-related, and somatoform disorders (F40–F48); sleep disorders or nonorganic sleep disorders (F51 or G47); organic (including symptomatic) mental disorders (F00–F09); and substance-related disorder and mental and behavioral disorders due to psychoactive substance use (F10–F19). In this study, patients were classified as having “other” psychiatric problems when their main diagnosis was not psychiatric illness, but have received psychiatric treatment.
We considered all diagnoses attributed to the patients during the follow-up period and defined comorbidity. The comorbidities considered in this study were personality disorder and pain. Based on their ICD-10 codes, the two categories are as follows: personality disorder (specific or mixed/other) (F60 or F61); and pain, headache, malaise and fatigue, fibromyalgia, complex regional pain syndrome (CRPS) I, and CRPS II (multiple site or upper limb) (R51, R52, R53, M797, M890, G5780, G5881, or G564).
Statistical analysis
Participants were divided into suicidal deaths group vs. survivors or non-suicidal deaths group, and baseline demographic and clinical characteristics of the two groups were compared. The average follow-up duration of all participants was calculated and the mean values of the two groups were compared through t-test. The χ2 test was used to compare the observed difference in the nominal variables between groups, such as age group at first visit, sex, diagnosis, and comorbid personality disorder and pain. The distribution of these characteristics of patients by diagnosis was also investigated regardless of suicide outcome.
We calculated the standardized mortality ratio (SMR) of suicide for comparison with the general population, and the hazard ratio (HR) to compare the risk of suicide by diagnosis within participants. The SMR of suicide was defined as the ratio of the observed suicide deaths to the expected suicide deaths among the participants. The number of expected suicide deaths in the participants was calculated by multiplying person-years at risk and year-, sex- and age group-specific suicide death rates in the Korean population, where age groups were 0, 1–4, 5–9, 10–14, …, 85–89, 90+.24 Person-years at risk was computed based on each participant's follow-up period. Diagnosis-specific SMR was calculated in the same way as the ratio of the number of observed and expected suicides for each diagnosis.
The Cox proportional hazards model was used to investigate the HR of suicidal death for each diagnosis. The age considered in the survival analysis was the age at the first visit. The observation period was from the first visit to death, in case the participants died during the study period. The observation period for the survivors was from the year of the first visit to the end of the study in 2017. As a supplementary analysis, changes in HRs according to four factors in each diagnosis were investigated: age, sex, comorbid of personality disorder, and pain. Within each diagnosis, survival analysis was performed using the Cox proportional hazards model. For convenience, comparison was made between patients younger or older than the mean age of the sample, 47.91 years. All statistical analyses were performed using SPSS version 25.0 for Windows (SPSS Inc., Chicago, IL, USA). P value < 0.05 was considered statistically significant.
RESULTS
Baseline demographic and clinical characteristics of patients
From March 1, 2003 to December 31, 2017, 67,869 patients visited psychiatric outpatient clinic, were hospitalized in a psychiatric ward, or received psychiatric consultation at emergency department at SNUH, and 41,289 patients did at least three times. Among patients who visited at least thrice, 597 (1.4%) died by suicide (Fig. 1). The mean follow-up period of the study participants was 7.7 years, and the mean follow-up period of survivors or non-suicidal deaths group and suicidal deaths group was 7.7 years and 4.2 years, respectively (t = 23.85, P value < 0.001).
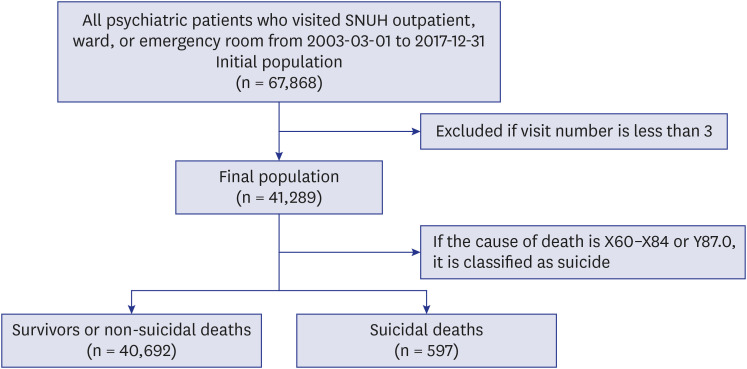
Fig. 1
Flowchart showing the process in which participants are divided into two groups. All psychiatric patients who visited Seoul National University Hospital outpatient, ward, or emergency room from 2003-03-01 to 2017-12-31 were totally 67,868. From them, those who visited less than 3 times were excluded. The National Statistical data was matched, and among the patients with death information, the patient with cause of death code X60–X84 or Y87.0 was classified as a suicidal deaths, otherwise a survivor of suicidal death. Finally, there were 40,692 survivors or non-suicidal deaths, and 597 suicidal death.
![]()
As shown in Table 1, the two groups showed statistically significant differences in age, sex, diagnosis at the first visit, and comorbidity of personality disorder. Both groups had the highest rates of suicide in their twenties—25.6% in the suicidal deaths group, and 17.9% in the survivors or non-suicidal deaths group. Male sex was statistically more frequent in the suicidal deaths group compared to the comparator, 53.8% vs. 44.1%. By diagnosis, the highest frequency diagnosis in the suicidal deaths group was psychotic disorder (31.3%), and depressive disorder for the survivors or non-suicidal deaths group (23.6%). As for comorbidity, the proportion of patients with a personality disorder was higher in the suicidal deaths group, though that of patients with chronic pain was similar in both groups.
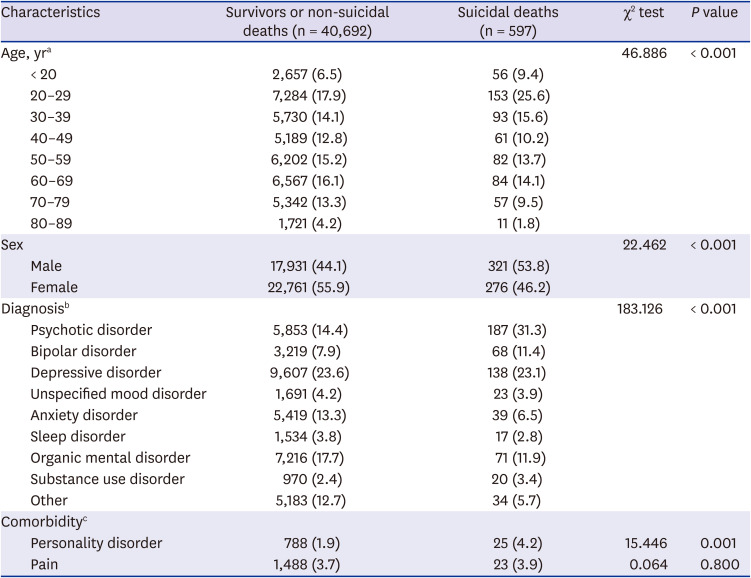
Table 1
Baseline demographic and clinical characteristics of patients
Values are presented as number (%).
ICD-10 = International Classification of Diseases 10th revision.
aFirst visit age; bDiagnosis was classified based on the ICD-10 coding system; psychotic disorder (F20–F29), bipolar disorder (F30 or F31), depressive disorder (F32, F33, or F34), unspecified mood disorder (F39), anxiety disorder (F40–F48), sleep disorder (F51 or G47), organic mental disorder (F00–F09), and substance-related disorder (F10–F19); cComorbidity is a subdiagnosis and follows the ICD-10 coding system; personality disorder (F60 or F61), and pain (R51, R52, R53, M797, M890, G5780, G5881, or G564).
![]()
Table 2 shows the distribution of sex, age at first visit, and comorbidity for each diagnosis. Bipolar disorder had the highest frequency of being comorbid with personality disorders (5.7%). Among patients with unspecified mood disorder, 6.2% were diagnosed with chronic pain, which is the highest proportion among all diagnoses. In the case of substance-related disorder, the ratio of male sex was the highest (72.9%). Patients with psychotic disorder and bipolar disorder first visited at earlier age, whereas most patients with organic mental disorder and sleep disorder tended to make their first visit after reaching middle age. Depressive disorder was evenly distributed across all age groups.
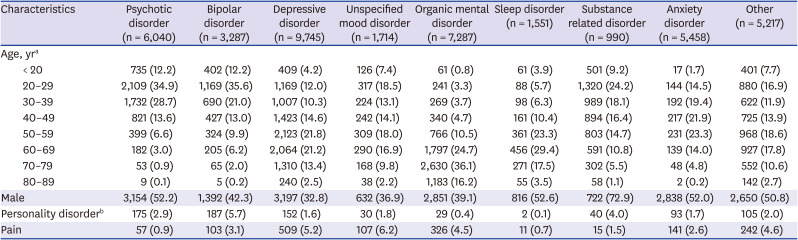
Table 2
Baseline demographic and clinical characteristics of patients according to psychiatric diagnosis
Values are presented as number (%). The baseline characteristics were counted for each diagnosis regardless of suicide, and the percentage in the diagnosis was calculated.
aFirst visit age; bComorbidity is a subdiagnosis and follows the International Classification of Diseases 10th revision coding system; personality disorder (F60 or F61), and pain (R51, R52, R53, M797, M890, G5780, G5881, or G564).
![]()
Standardized mortality rates of suicide for each diagnosis
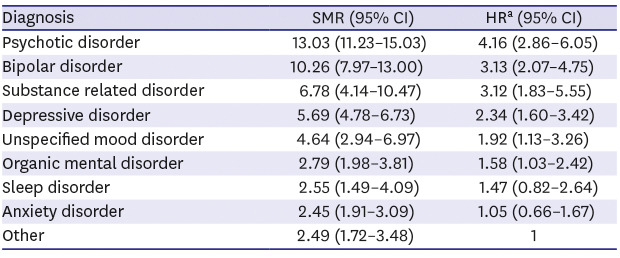
The observed mortality rate of suicide among the subjects was 5.13-fold higher than the expected rate of the general population (SMR, 5.13; 95% confidence interval [CI], 4.73–5.56). The calculated diagnosis-specific SMRs of suicide were 13.03 (95% CI, 11.23–15.03) for psychotic disorder, 10.26 (95% CI, 7.97–13.00) for bipolar disorder, and 5.69 (95% CI, 4.78–6.73) for depressive disorder. Substance-related disorder, anxiety disorder, and sleep disorder also showed higher suicide rates compared to the general population, their SMR being 6.78 (95% CI, 4.14–10.47), 2.45 (95% CI, 1.91–3.09), and 2.55 (95% CI, 1.49–4.09) respectively, although these disorders are not listed among the SMIs. Organic mental disorders and others revealed SMRs of suicide of 2.79 (95% CI, 1.98–3.81) and 2.49 (95% CI, 1.72–3.48), respectively (Table 3).
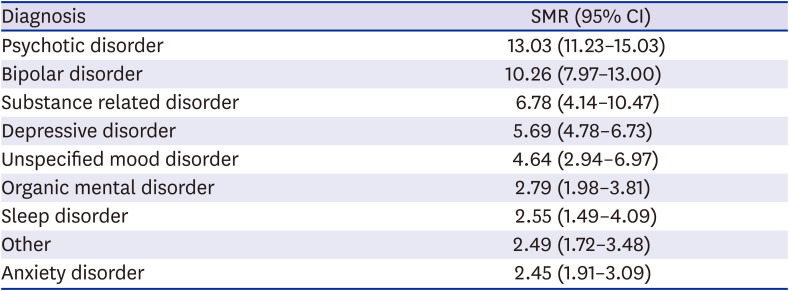
Table 3
Diagnosis-specific standardized mortality rates of suicide
SMRs of suicide were defined as the number of suicidal deaths observed in the participants/number of expected deaths by suicide.
SMR = standardized mortality ratio, CI = confidence interval.
![]()
Survival analysis using Cox-proportional hazards model
Psychotic disorder had the highest HR of 4.16 (95% CI, 2.86–6.05). The HRs of bipolar disorder, depressive disorder, and unspecified mood disorder were 3.12 (95% CI, 1.83–5.55), 2.34 (95% CI, 1.60–3.42), and 1.92 (95% CI, 1.13–3.26), respectively. Although the order of greater suicide risk among psychiatric diagnoses were similar when compared with SMRs or HRs for most diagnoses, HR of substance-related disorder (3.12; 95% CI, 1.83–5.55) was high, similar to that of bipolar disorder (3.13; 95% CI, 2.07–4.75) (Table 4). HR of organic mental disorder was found to be 1.58 (95% CI, 1.03–2.42). The Kaplan-Meier plot is shown in Fig. 2.
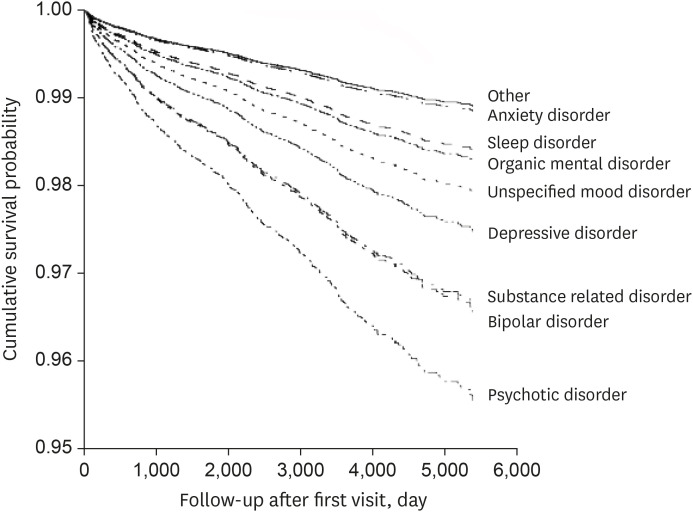
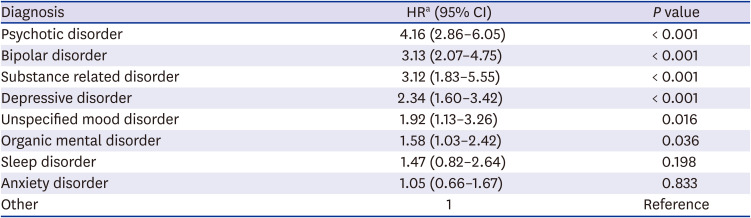
Fig. 2
Diagnosis-specific survivor curves for 14 years of follow-up. Fig. 2 is a survival analysis graph visualized the contents of Table 4. The diagnosis with the highest HR was psychotic disorder and psychotic disorder has the lowest survival rate. The next highest HR diagnosis was substance-related disorder and bipolar disorder. The diagnosis with the lowest risk of suicide was the group without a psychiatric diagnosis as the main diagnosis.
HR = hazard ratio.
![]()
Table 4
Comparison of diagnosis-specific HRs of suicide
The reference is the anxiety disorder and the ratio is adjusted by age, sex, and comorbidity of personality disorder, pain.
HR = hazard ratio, CI = confidence interval.
aHR is calculated for each diagnosis using the Cox proportional hazard model.
![]()
HRs of suicide according to risk factors
Supplementary Table 1 describes HRs according to combination of risk factors in each diagnosis. Patients with psychotic disorder and bipolar disorder had greater suicide rates when combined with personality disorder (HR, 1.74; 95% CI, 1.16–2.60 and HR, 2.34; 95% CI, 1.10–4.99, respectively). Pain significantly increased the risk of suicide in organic mental disorder (HR, 2.38; 95% CI, 1.16–4.86). Suicide risk for psychotic disorder increased at younger age whereas, for bipolar disorder, suicide risk increased at older age.
DISCUSSION
This study evaluated the risk of suicide in psychiatric patients, comparing with the general population and among different psychiatric diagnoses. Compared to the general population, the risk of suicide in psychiatric patients was 5.13-fold higher. Based on patient's diagnosis, psychotic disorder had the highest risk of suicide, followed by bipolar disorder, substance-related disorder, and depressive disorder.
In this study, standardized suicide mortality ratio was 5.13 for all psychiatric patients, 13.03 for those with a psychotic disorder, and 10.26 for bipolar disorder. Previous studies have reported 10- to 30-fold greater risk of suicide in bipolar disorder compared to the general population,6252627 It is also suggested that the risk of suicide increases by 20–30 folds, when the age, sex, and severity of symptoms are corrected.28 However, in a London study29 that did not correct for disease severity, the bipolar cohort had an SMR of 9.77. This paper argues that the risk of suicide in bipolar disorder is exaggerated in some of the studies. In fact, risks of suicide in bipolar disorder reported in studies varied in a wide range according to a recent systematic review.5
SMR for suicide in schizophrenia also differed depending on the country and the study method. In a Swedish study,30 male patients with schizophrenia had an SMR of 15.7, while female patients had an SMR of 19.7. Another 10-year follow-up study in France31 reported similar numbers: the SMR of male schizophrenia patients was 15.8 and of female patients was 17.7. However, in a Taiwanese study using 12-year data,32 the SMR for suicide in schizophrenia patients was as high as 31.3. The study attributes its dissimilar results to their differences in follow-up periods and standard treatments. Literature suggests that differences between the characteristics of the patient groups included in the study, the characteristics of institution, treatment methods, and patient recruitment period may affect SMRs, and that direct comparison between the SMRs calculated in these studies can be difficult.33 Nevertheless, the finding of which patients with psychotic disorder are at higher risk of suicide compared to those with bipolar disorder is similar in most of previous diagnosis-specific SMRs studies,293031 which has important implications.
Previous studies suggest that patients with psychotic disorder have a high suicide rate because they use more fatal methods of suicide.34 Lack of insight may also result in poor adherence to medication and contribute to increased risk of suicide.35 Indeed, although mental illness is a strong risk factor for suicide, proactive management and appropriate treatment may reduce the risk.36
Organic mental disorder and sleep disorder had higher risk of suicide than anxiety disorder. Organic mental disorders, including dementia, increase the risk of suicide among older people over the age of 70.37 It is suggested that risk of suicidal behavior is increased if treatment does not improve the cognitive abilities in depressed patients with early Alzheimer's dementia.38 Sleep disorder also independently increases the risk of suicide.39 However, in case of anxiety disorder, only post-traumatic stress disorder is a risk factor for suicide40 while other studies even suggest that anxiety may reduce suicidal behavior or impulsivity.41 Increased risk of suicide when pain8 or personality disorder coexists591142 is consistent with previous studies.
Similar to our findings, risk of suicide was increased at early age in psychotic disorder, while at older age in bipolar disorder.243 A small Israeli study44 reported that the risk of suicide in elderly bipolar disorder was high, yet bipolar patients are considered to be at high risk of suicide during their youth.5 As this study considered the age of the first visit, it is difficult to distinguish whether patients have received treatment before their visit and to therefore conclude that these results are for patients who have started treatment after middle age. Nonetheless, there is a possibility of high risk of suicide in elderly bipolar disorder, and further study is needed.
A limitation of this study is the study sample may not represent the study population in Korea, as it was conducted in a single medical institution. Additionally, the age used for analysis in the study is not the age of onset, but the age recorded at the initial visit to the hospital. Therefore, the possibilities of receiving treatment at another hospital before coming to this hospital, and the first visit occurring long after previous onset were not considered. Other sociodemographic factors such as living alone, being divorced, early trauma, and exposure to suicide were not considered in the study.
However, the study has several strengths. This is a 14-year longitudinal study using a large sample size data, which were extracted using the recently developed SUPREME system. Moreover, to our knowledge, this is the first study that investigates the risk of suicide among Korean psychiatric patients compared to the general population. It is also meaningful to state that our study presents both SMRs and HRs, which are considered to be representative values with external and internal validity, by comparing with the general population and between diagnosis within the patient group.
This study found that people with mental illness are at 5.13-fold higher risk of suicide than the general population, and those with a psychotic disorder have the highest risk of suicide, greater than those with bipolar disorder. The risk of suicide can vary depending on age and sex, psychiatric diagnosis, and coexistence of personality disorder or pain. Thus, it is important to assess patients' risk by examining their situations. Such findings should be considered in making health policies for suicide prevention plans for Korean psychiatric patients.
 XML Download
XML Download