

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Palliative care focuses on improving the quality of life of seriously ill patients and their families through symptom management, communication, and patient autonomy.1 Although palliative care has focused initially on patients with terminal cancer, studies have indicated that the patient population that may benefit from palliative care is considerably larger.1 Many randomized controlled trials and case-control studies of palliative care interventions have reported that palliative care leads to reductions in patients' symptoms and health-care utilization, along with improvements in quality of life and family satisfaction; such findings have been reported for a wide spectrum of populations, including patients with advanced cancer, neurologic disease, and end-organ failure,23 as well as older adults with multiple coexisting conditions and frailty.45 However, despite the fact that international guidelines recommend palliative care approaches for several different serious illnesses,67891011 the palliative needs of patients with serious illnesses other than cancer are often unmet.2
Many previous studies have explored, for a range of serious illnesses, the barriers associated with the provision of palliative care to patients.121314 Their findings showed that one of the main challenges in this regard is a lack of discussion regarding prognosis and life expectancy.15161718 A realistic sense of prognosis can help patients plan and make informed care-related decisions as they approach the end of their lives.1920 Routine discussion of prognosis is further supported by physicians' ethical obligation to respect patient autonomy and provide complete and truthful disclosure.21
This study examines people's attitudes toward prognostic disclosure in the context of serious illnesses other than cancer. To the best of our knowledge, this question has not been researched previously. To investigate this issue, we sought to quantify the proportions of physicians and the general public who would support prognostic disclosure if they or a family member were terminally ill. We also investigated factors these populations considered crucial for disclosing prognosis, and reasons for not disclosing prognosis. The aim of this study is to compare physicians' and the general public's attitudes toward prognostic disclosure, focusing on a range of serious illnesses, including end-organ failure, acquired immune deficiency syndrome (AIDS), stroke, Parkinson's disease, dementia, and incurable genetic or neurologic diseases.
METHODS
Participants and procedures
Data were collected in July–October 2016. Details of the study design have been published previously.22
General public
To examine the opinions of the general public, we used a probability-proportional-to-size technique which is widely used and recommended for obtaining a national representative sample. We recruited a sample of 1,000 respondents from all 17 administrative divisions in Korea, who were 20–70 years of age. Professional interviewers administered to them a structured questionnaire. 1,005 members of the general public participated.
Physicians
We invited physicians from 12 secondary and tertiary hospitals and the Korean Medical Association to participate in the online survey. Of the 3,100 doctors who were sent the questionnaire via e-mail, 928 responded (response rate: 29.9%). Regarding specialty, internal medicine was the most represented (27.2%), followed by family medicine (10.0%). Regarding position, most participants were faculty members (39.5%), followed by residents and fellows. To enhance the generalizability of the findings, we weighted observations from physicians according to age and sex distribution of the physician population using Korean Medical Association statistics.23
Materials
Opinion on the disclosing of terminal status
Respondents' opinions regarding disclosing terminal status were queried for two situations: 1) if the respondent was the patient, and 2) if the respondent's family member was the patient. For both cases, the question was: “Do you think that, if you were (or ‘a family member was,’ for the second situation) terminally ill, you (they) should be informed of your (his/her) status?” The respondent could reply “yes” or “no.” The following definition of the term “terminally ill” was provided with the survey questions: Despite active treatment, the doctor expects that the patient will die from a progressive condition within several months.
Factors to consider regarding terminal status disclosure
Next, we asked respondents “what do you think is the most important factor to consider when disclosing a patient's ‘terminal status’?” Here, respondents could choose only one from a list of seven factors: 1) life expectancy and other treatment options, 2) the accuracy of the terminal prognosis, 3) the patient's right to know his/her condition, 4) potential patient frustration and discouragement, 5) associated socio-economic burden, 6) facilitating patient-centered planning for end-of-life care, and 7) the patient's opportunity to complete their life.
Reasons for not disclosing terminal status
Those who stated that they were not in favor of disclosure were asked to provide a reason for their decision. Here, they were asked to choose just one reason from a list of five or, if none of the five were applicable, to enter their own reason (only one response was allowed). The five presented reasons were: 1) the patient may lose hope, 2) disclosure would have no beneficial effect, 3) the patient may refuse necessary treatment, 4) disclosure would create a psychological burden, such as anxiety or depression, 5) previous experience of an adverse event after a patient was informed of their terminal status.
Propensity-score weighting
We used propensity-score weighting to address potential sources of confounding between the respondent groups and the outcomes. Potential sources of confounding included demographic factors, socioeconomic status, and whether respondents had a serious illness and/or experience of providing care for a seriously ill patient. This approach facilitated a comparison between the general-public group and the physician group, which were consequently balanced in terms of the above-stated factors. We used logistic regression to create a propensity score for being in the physician group, adjusting for the variables provided in Table 1. For physicians, we computed the inverse of the propensity score, while for the general public, we computed the inverse of one minus the propensity score. Using these weights, a propensity-weighted sample was created. Weights were then trimmed to improve precision.24 Standardized differences were used to assess the covariate balance between the physician group and the general-public group; meaningful imbalances were defined by an absolute standardized difference of −0.15 to 0.15.25 Unless otherwise specified, we present propensity-weighted analyses. All analysis results without propensity weighting are included in the Supplementary Tables 1-6.
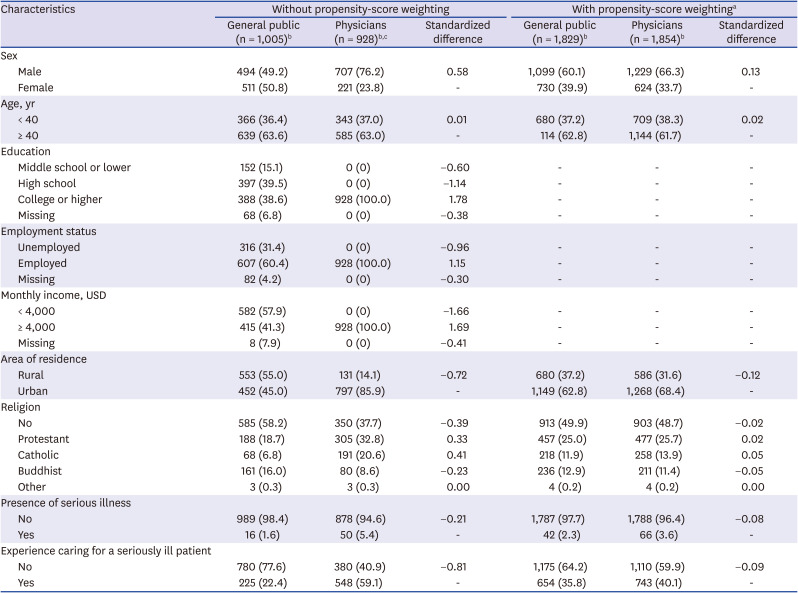
Table 1
Participants' characteristics
Data are presented as number (%).
aPropensity-score adjusted for sex, age, area of residence, religion (Protestant, Catholic, Buddhist, and other), presence of serious illness, and experience caring for a seriously ill patient; bWeighted frequencies are rounded to whole numbers; therefore, group composites may not equal the total; CFrequencies are weighted according to age and sex distribution of the physician population using Korean Medical Association statistics.
![]()
Statistical analysis
To compare preference to not disclose terminal status to patients between the general public and physicians, adjusted proportions and adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were calculated using logistic regression. Through cross-tabulation analysis, we sought to identify the primary factors to consider when disclosing terminal status, as well as the main reason for not disclosing terminal status. We used SPSS statistical software version 23.0 (SPSS Inc., Chicago, IL, USA) for all analyses and calculated two-sided P values.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. E-1612-102-815). Written Informed consent was obtained from all subjects upon their enrollment in the study. We conducted the study in accordance with the principles of the Declaration of Helsinki.
RESULTS
Sample characteristics
The questionnaire was completed by 1,005 members of the general public and 928 physicians. Table 1 presents the characteristics of both groups of respondents. The general-public group contained a higher percentage of women than did the physician group, and was more likely to be less educated, unemployed, have a lower income, live in a rural area, and to have no religion. In addition, the general- public group was less likely to have a serious illness or experience caring for a seriously ill patient. Prior to propensity-score weighting, standardized differences for baseline covariates ranged from −1.66 to 1.78. However, after propensity-score weighting, standardized differences for baseline covariates ranged from −0.12 to 0.13, indicating improved covariate balance between the general-public and physician groups.
Preference for disclosing prognosis
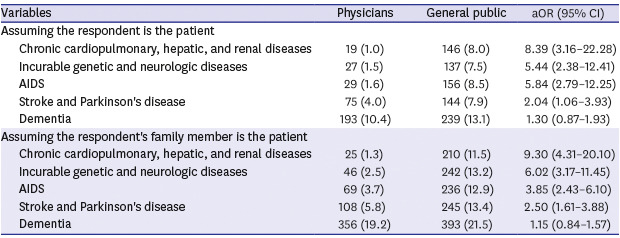
Table 2 shows, for each disease examined, preference for not disclosing prognosis, adjusted for propensity score (Supplementary Table 1). For the situation in which the respondent is the patient, most physicians (adjusted proportions – end-organ failure: 99.0%; incurable genetic or neurologic disease: 98.5%; AIDS: 98.4%; stroke or Parkinson's disease: 96.0%; and dementia: 89.6%) and members of the general public (end-organ failure: 92.0%; incurable genetic or neurologic disease: 92.5%; AIDS: 91.5%; stroke or Parkinson's disease: 92.1%; and dementia: 86.9%) wanted to be informed if they had a terminal prognosis. The general-public group was more likely than the physician group to favor not disclosing prognosis for end-organ failure, incurable genetic or neurologic disease, AIDS, and stroke or Parkinson's disease (adjusted odds ratio [aOR], 8.39; 95% CI, 3.16–22.28; aOR, 5.44; 95% CI, 2.38–12.41; aOR, 5.84; 95% CI, 2.79–12.25; and aOR, 2.04; 95% CI, 1.06–3.93, respectively).
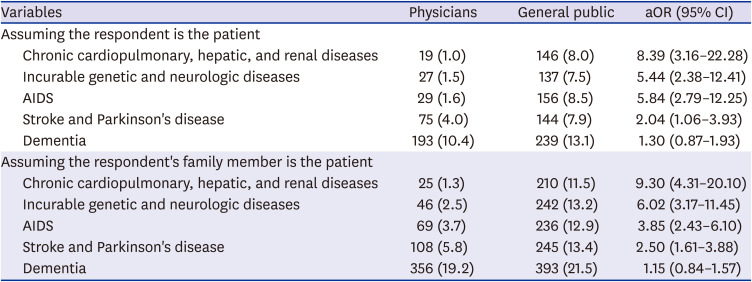
Table 2
Comparison of preference for not disclosing prognosis between physicians and the general publica
Values are presented as number (%).
aOR = adjusted odds ratio, 95% CI = 95% confidence interval, AIDS = acquired immune deficiency syndrome.
aPropensity-score adjusted for sex, age, area of residence, religion (protestant, catholic, buddhist, and other), presence of serious illness, experience caring for a seriously ill patient.
![]()
Similarly, for the situation in which the respondent's family member is the patient, most physicians (adjusted proportions – end-organ failure: 98.7%; incurable genetic or neurologic disease: 97.5%; AIDS: 96.3%; stroke or Parkinson's disease: 94.2%; and dementia: 80.8%) and members of the general public (end-organ failure: 88.5%; incurable genetic or neurologic disease: 86.8%; AIDS: 87.1%; stroke or Parkinson's disease: 86.6%; and dementia: 78.5%) wanted their family members to be informed if they had a terminal prognosis. The general-public group was again more likely than the physician group to prefer not disclosing prognosis for end-organ failure, incurable genetic or neurologic disease, AIDS, and stroke or Parkinson's disease (aOR, 9.30; 95% CI, 4.31–20.10; aOR, 6.02; 95% CI, 3.17–11.45; aOR, 3.85; 95% CI, 2.43–6.10; and aOR, 2.50; 95% CI, 1.61–3.88, respectively). In both situations, there were no significant differences between the two groups regarding the preference for not disclosing prognosis of dementia.
Main factors to consider when disclosing terminal status
Table 3 shows, for both groups, perceived importance of factors to consider when deciding whether to disclose a prognosis. For physicians (31.4%) and the general public (31.9%), the primary factor to consider was the “patient's right to know his/her exact condition.” “Life expectancy and other treatment options” were more important for physicians (29.8%) than for the general public (14.2%), and “Potential patient frustration and discouragement” were more important factors for the general public (13.6%) than for the physicians (5.6%) (Supplementary Table 2).
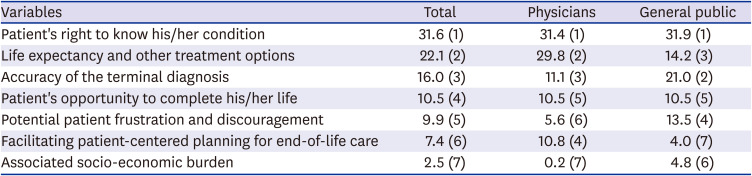
Table 3
Factors to consider when disclosing prognosisa
Values are presented as % (rank).
aPropensity-score adjusted for sex, age, area of residence, religion (protestant, catholic, buddhist, and other), presence of serious illness, experience caring for a seriously ill patient.
![]()
Reasons for not disclosing terminal status
Table 4 lists the groups' attitudes towards reasons for not disclosing a prognosis. For the general public, “psychological burden, such as anxiety and depression” was the primary reason not to disclose a prognosis (35.8%), while for the physicians “disclosure would have no beneficial effect” was most common (42.4%). Additionally, “the patient may lose hope” (24.6% and 7.8%, respectively) and “the patient may refuse necessary treatment” (13.2% and 4.3%, respectively) were more important reasons for the general public than for the physicians (Supplementary Table 3).

Table 4
Reasons for not disclosing prognosisa
Values are presented as % (rank).
aPropensity-score adjusted for sex, age, area of residence, religion (protestant, catholic, buddhist, and other), presence of serious illness, experience caring for a seriously ill patient.
![]()
DISCUSSION
To the best of our knowledge, this is the first study to compare, between physicians and the general public, attitude toward prognostic disclosure of terminal status in serious illnesses other than cancer. Our most important finding is that most of the physicians and the members of the general public we examined favored disclosure of terminal prognosis to a patient, regardless of whether the patient was the respondent themselves or a family member. This finding provides, for terminal illnesses in general, not just cancer, persuasive data supporting patient autonomy and patients' right to be told the truth about their health condition. This is especially significant for health-care professionals who may choose to withhold information about a terminal illness because they believe that the patient would prefer to remain unaware.
In our previous studies conducted in 2004 and 2010 with cancer patients and their families in Korea, 96% (2004) and 79% (2010) of cancer patients and 77% (2004) and 70% (2010) of their caregivers preferred that patients be informed of their terminal status.2627 Moreover, the Ministry of Health and Welfare of Korea surveyed 88 patients with serious illnesses and 226 caregivers in 2013 and, though results for each illness were not reported, found that 97% of respondents wanted a discussion with their doctor about their condition and available treatment options.28 In the current study, the proportions of the general public who wanted a prognostic disclosure for each serious illness were from 92.5% to 78.5%, which are similar to those in previous studies.
Some members of the general public, however, favored protecting patients from the knowledge of their terminal status. The general public was more likely to prefer not disclosing terminal prognosis of serious illnesses to the patient than physicians. The main reason for not disclosing prognosis was potential psychological distress for patients, such as anxiety, depression, or losing hope. However, compared to the previous study regarding prognostic disclosure to children with serious illness, the extent of discordance between physicians and the general public was much smaller.29 The employed or Catholic general public were more likely than those who were unemployed or have no religious beliefs to prefer disclosing terminal prognosis. Gender, age, education level, income, area of residence, and having other religious beliefs were not associated with disclosure preferences (Supplementary Table 4).
The general public's preference for nondisclosure was higher when their family member was the patient compared to when they were the patient (Supplementary Table 5). This conforms with our previous findings regarding cancer that indicated caregivers are less likely to feel that patients should be informed of their terminal status than patients; further, 46.6% of the patients who were against disclosure felt that it would cause psychological and emotional burden.2627 In fact, earlier studies reported that, in some patients with advanced cancer, accurate prognostic awareness is related to worse quality of life and mood.3031 However, more adaptive coping strategies among patients have been shown to buffer this relationship.31 Moreover, prognostic disclosure by physicians, coupled with high-quality information and communication, increases patients' peace of mind, trust, and hope.32
Another important finding in the present study was diagnosis-related differences in the preference for prognostic disclosure. Physicians were less likely to prefer disclosing prognosis of dementia, Parkinson's disease or stroke, and AIDS than end-organ failure (aOR, 17.08; 95% CI, 8.20 to 35.60; aOR, 4.44; 95% CI, 2.18 to 9.91; and aOR, 2.76; 95% CI, 1.49 to 5.10, respectively) (Supplementary Table 6). The majority of physicians who opposed disclosure felt that such disclosure would have no beneficial effect. Previous studies have reported that misperceptions, a lack of awareness, and improper attitudes among the public and health-care professionals can interfere with the provision of care.1233 Specifically regarding dementia, the most-cited barrier is a lack of awareness that advanced dementia is a terminal condition.12333435 Other barriers include the belief that palliative care has no meaningful effect for dementia.36 Increasing the public's and health-care professionals' awareness about nature and dying process of dementia, and available services could facilitate the provision of palliative care in advanced dementia.34
Our findings may also reflect the difficulty physicians experience when trying to communicate with patients who have cognitive or communicative impairments due to chronic progressive neurologic diseases such as dementia,37 Parkinson's disease,38 and other neuromuscular diseases.39 Patients may wish to maintain a sense of autonomy by making decisions regarding their future care while their cognition remains intact.40 Anticipating the loss of decision-making capacity, clinicians should discuss prognoses and care plans with patients and families or surrogate decision-makers at an early stage.41 Earlier discussions can help to ensure that the care provided is consistent with patients' preferences, and can also have a beneficial effect on clinical outcomes, including improving quality of life, avoiding aggressive medical care when the patient is near death, and referring patients to hospices at an earlier stage.42
The unpredictable disease course and difficult prognostication of the diseases considered may also have influenced our findings. Knowledge of typical illness trajectories and access to prognostic tools provide clinicians with a framework for discussions regarding prognosis43; however, for many diseases the courses are more complex and unpredictable than those for cancer.13151844 Further, outcome estimation tools in acute illnesses have not been established for end-of-life treatment decisions, so physicians may not be able to predict quality of life, which is subjective but important to patients and families at the end-of-life.11 Future research should examine the suitability of existing prognostic tools for different serious illnesses in the context of end-of-life decision-making. Prognostic uncertainty is unavoidable; nevertheless, most patients and families still prefer that their physicians discuss a prognosis, even if they cannot be certain they are correct, as more information will help them make appropriate decisions regarding treatment and care plans.45
In 2017, for several non-cancer serious illnesses including AIDS, chronic obstructive pulmonary disease, and liver cirrhosis, national hospice and palliative care service has started in Korea. According to the report of the Korean ministry of health and welfare in 2019, only 16 patients among 7,730 patients who died from these conditions used the service in 2017.46 Appropriate prognostic disclosure would be the first step to shared decision-making on treatment choices and creating an advance care plan. At least for these illnesses, there is an urgent need to revise the guidelines to provide recommendations on discussing prognosis and care plans. Moreover, the development of a competency-building program for early prognostic discussion might be helpful for all professionals who care for patients with serious illnesses.
Our study has several limitations. First, the response rate of physicians was low (29.9%). Although we weighted observations from physicians according to the age and sex distribution of the physician population using Korean Medical Association statistics, we cannot exclude the possibility that the nonparticipating physicians would have responded differently. Second, patients with each serious illness and their caregivers were not included in the current study. The patients' or caregivers' opinions on prognostic disclosure might have been different from the general public's opinions that have been presented in our study. Third, the study was conducted in Korea and, as a result, may not be generalizable to other cultures. Last, causal relationships are uncertain in this cross-sectional study, and hidden confounders may have influenced associations.
In conclusion, for various serious illnesses, most physicians and the general public agree that disclosure of a terminal prognosis respects patient autonomy. Yet, more than 10% of the respondents from the general public did not want to provide prognostic disclosure if their family members were patients. They expressed concern about the psychological distress it may cause the patient. The low response rate of physicians might limit the generalizability of the results. Further research is needed to identify the best means of and timing for communicating prognoses and care plans for each serious illness.
 XML Download
XML Download