

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Malignant lymphoma accounts for around 10% of all childhood cancers. Hodgkin's lymphoma (HL) constitutes 10%–20% of these cases and occurs less commonly than non-Hodgkin's lymphoma (NHL). HL has a high cure rate, with a survival rate of around 90%, which has resulted in an increased occurrence of complications such as secondary cancers and endocrine disorders in long-term survivors.123
HL affects approximately 2.9/100,000 and 2.3/100,000 male and female, respectively, and accounts for 1,070 deaths annually in the United States.4 It is the most common cancer diagnosis in patients between the ages of 15 and 24 years, and > 40% of newly diagnosed HL patients are between the ages of 15 and 34 years in the United States.2 In Korea, HL affects approximately 0.8/100,000 male and 0.4/100,000 female and accounts for about 50 deaths annually.5 In 2016, 312 new patients were diagnosed with HL in Korea, of which 69 (22%) were < 25 years of age. The 5-year relative survival rate for HL diagnosed during 2011–2015 was 83.0%.6
In the 1960s, high-dose radiotherapy (35–45 Gy), administered for the treatment of HL, was responsible for the development of various complications and was therefore replaced by the combination mechlorethamine, vincristine, procarbazine hydrochloride, and prednisone (MOPP) treatment regimen.7 Several combination therapies have since been developed to limit toxicity and increase treatment effectiveness. Subsequent HL treatments including combination chemotherapeutic regimens such as MOPP, doxorubicin, bleomycin, vinblastine, dacarbazine (ABVD), and other alkylating agents (excluding mechlorethamine) were devised to minimize long-term complications while maintaining the therapeutic effect. Moreover, new combination therapies have been developed with the addition of cyclophosphamide, or replacement with etoposide, to reduce the required dose of radiation.
Considering the high cure rate of HL, recent treatment trends are progressing toward reducing long-term complications in cancer survivors while maintaining survival outcomes. Recent studies have utilized bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, prednisone (BEACOPP) combination therapy and brentuximab therapy for advanced HL.2489 Moreover, immune checkpoint therapy is being introduced as salvage treatment in patients with refractory and relapsed HL.1810
There have been many studies on treatment outcomes and prognostic factors in adult HL, and many guidelines have been developed.111213 Few studies have been conducted with children and young adults.1415 The Korean Pediatric Hematology and Oncology Group (KPHOG) was launched in 2014 in the Korean Society of Pediatric Hematology-Oncology to promote multicenter research and to contribute to the development of pediatric hematology oncology. The lymphoma committee of the KPHOG first aimed to identify epidemiologic features, therapeutic outcomes, prognostic factors, and late complications of HL in children, adolescents, and young adults in Korea through this multicenter, retrospective study.
METHODS
Patient enrollment
The study protocol was approved by the lymphoma committee of the KPHOG. We performed a retrospective study of patients diagnosed with HL between January 2007 and August 2016 in Korea. Eligibility criteria were age < 25 years and patients with newly diagnosed, biopsy-proven HL. We collated records of 263 patients from 22 participating institutions for the retrospective analysis. Of these, 16, 14, and 9 patients were found to have incomplete data, an undetermined histopathological subtype, and incorrect diagnoses, respectively, thus excluding them from the study. Therefore, a total of 224 patient-records were finally analyzed (Supplementary Fig. 1).
Staging of HL
Staging of HL was performed using bone marrow biopsies and imaging modalities including contrast-enhanced computed tomography (CT) scanning, positron emission tomography (PET)-CT, or PET-magnetic resonance imaging (MRI). B-symptoms of HL used for prognostic assessment, included weight loss > 10%, unexplained recurrent fever > 38°, or drenching night sweats. The bulky disease was defined as the presence of a mediastinal mass with a diameter greater than one-third of the thoracic diameter on an upright anteroposterior chest radiograph or the detection of an extra-mediastinal, nodal aggregate measuring > 6 cm in the longest transverse diameter on axial CT, PET-CT, or PET-MRI. Patients were staged using the Ann Arbor staging system.16 The low-risk group included those patients found to have Ann Arbor stage IA or IIA disease, i.e., a non-bulky disease without extra-nodal involvement. The intermediate-risk group included Ann Arbor stage IB, IAE, IIB, IIAE, IIIA, IVA patients with/without a bulky disease, and those with IA/IIA stage HL with bulky disease. The high-risk group included Ann Arbor stage III or IV patients with positive B-symptoms. The limited stage was defined as stage I or II disease without B-symptoms or bulky disease. All other disease presentations were considered as advanced HL.
Treatment
After a definitive diagnosis of HL, patients received chemotherapy, radiotherapy, and/or hematopoietic stem cell transplantation (HSCT) according to each participating institution's treatment protocol. HSCT was performed in patients experiencing a relapse, refractory disease, or residual disease after completion of chemotherapy. Chemotherapeutic regimens consisted of adriamycin-bleomycin-vinblastine-dacarbazine (ABVD), cyclophosphamide, vincristine, procarbazine, prednisolone, doxorubicin, bleomycin, vinblastine (COPP-ABV), doxorubicin, bleomycin, vincristine, etoposide, prednisone, cyclophosphamide (ABVE-PC), BEACOPP, cyclophosphamide, vincristine, procarbazine, prednisone (COPP), cyclophosphamide, doxorubicin, vincristine, prednisone (CHOP), vincristine, procarbazine, prednisone, doxorubicin (OPPA), vincristine, etoposide, prednisone, doxorubicin (OEPA), vinblastine, doxorubicin, methotrexate, prednisone (VAMP), dexamethasone, etoposide, cisplatin, cytarabine (DECA), doxorubicin, bleomycin, vincristine, etoposide (DBVE), and Stanford V as per each participating institution's established treatment policy.
Statistical analysis
Demographic, clinical, and pathological data of the patient groups were compared using the χ2 test and Fisher's exact test for categorical variables. Event-free survival (EFS) and overall survival (OS) values, along with their standard errors in measurement, were estimated using the Kaplan-Meier method. OS was defined as the time interval between diagnosis and either death (from any cause) or the time of the last contact. EFS period was calculated from the date of diagnosis to either the last follow-up or the first related event including failure to achieve remission, relapse, second malignancy, or death due to any cause, whichever occurred first. A log-rank test was used to compare survival rates. Multivariate analysis for survival was performed using the Cox proportional hazards model. SPSS ver. 25.0 (IBM Inc., Armonk, NY, USA) was used for all statistical analyses. All P values were two-sided, and P < 0.05 was considered statistically significant.
RESULTS
Patient characteristics
Patient characteristics are summarized in Table 1. The study included 74, 99, and 51 children (0–12.9 years), adolescents (13–18.9 years), and young adults (19–24.9 years), respectively. The male-to-female ratio of study subjects was 1.87. A higher percentage of male patients were diagnosed at a younger age. The nodular sclerosis (NS) histopathological subtype of HL was most common (n = 128, 57%), followed by the mixed cellularity (MC) subtype (n = 57, 25.4%). NS was found more commonly in adolescents and young adults than in children. In contrast, MC occurred more frequently in patients belonging to the child age group (P = 0.012) (Fig. 1).
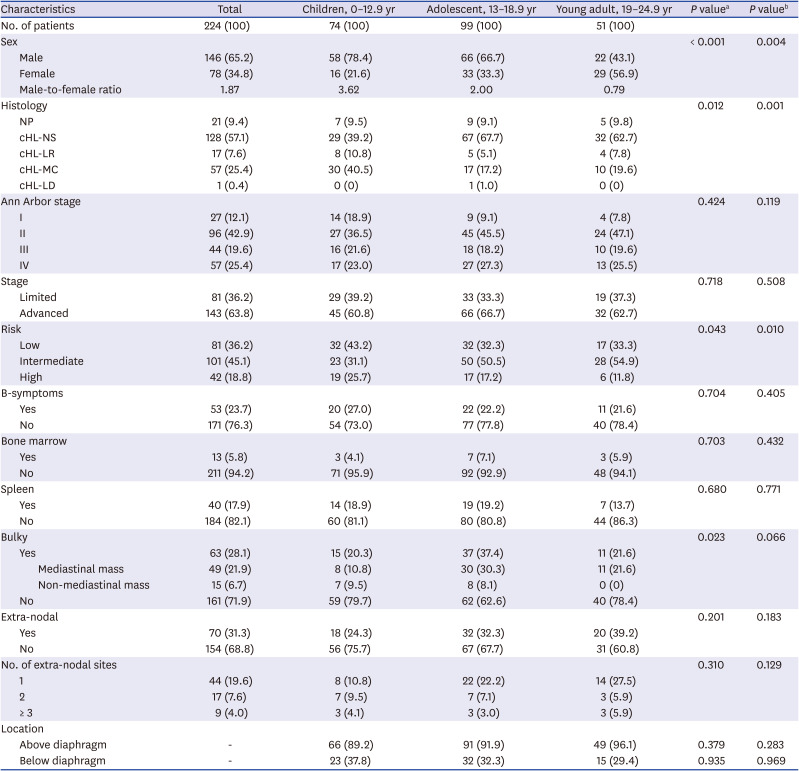
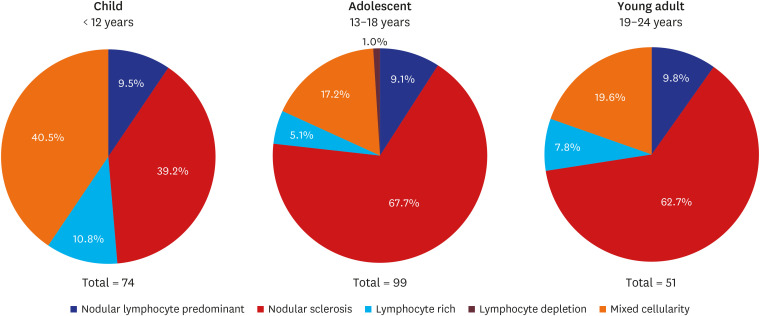
Table 1
Patient characteristics
Data are presented as number (%).
cHL = classic Hodgkin's lymphoma, NP = nodular lymphocyte predominant, NS = nodular sclerosis, LR = lymphocyte rich, MC = mixed cellularity, LD = lymphocyte depletion.
aP values were calculated among children, adolescent and young adult; bP values were calculated between children and adolescent + young adult.
![]()
Staging
According to the Ann Arbor staging system, a majority of the HL patients (96, 42.9%) were diagnosed with stage II, while stage IV was the second most (n = 57, 25.4%) common stage of diagnosis, followed by stage III (n = 44, 19.6%) and stage I (n = 27, 12.1%) (Table 1, Supplementary Tables 1 and 2). This frequency of diagnosis was the same across all age groups. In total, 81 (36.2%), 101 (45.1%), and 42 (18.8%) patients were classified into low-risk, intermediate-risk, and high-risk groups, respectively. Children were more commonly classified into the low-risk group (n = 32, 43.2%), whereas adolescents (n = 50, 50.5%) and young adults (n = 28, 54.9%) were found to commonly belong to the intermediate-risk group (P = 0.043). B-symptoms were present in 53 (23.7%) patients, while bone marrow and spleen involvement were found in 13 (5.8%) and 40 (17.9%) patients, respectively. Bulky disease, mediastinal mass, and a non-mediastinal mass of ≥ 6 cm were detected in 63 (28.1%), 49 (21.9%), and 15 (6.7%) patients, respectively. Extra-nodal involvement was observed in 70 (31.3%) patients.
Treatment
The most commonly used treatment regimen in all patients was ABVD (n = 102, 45.5%). This was followed by COPP-ABV and ABVE-PC in 65 (29.0%) and 32 (14.3%) patients, respectively. In the high-risk group, however, COPP-ABV was used more frequently than ABVD (Supplementary Table 3). In the young adult group, ABVD was most commonly used in the all-risk group (Table 2). One hundred six patients (47.3%) received radiotherapy. Thirty-nine (48.1%), 46 (45.5%), and 21 (50.0%) patients received radiation therapy in the low-, intermediate-, and high-risk groups, respectively. There was no difference in the type of radiotherapy according to age group.
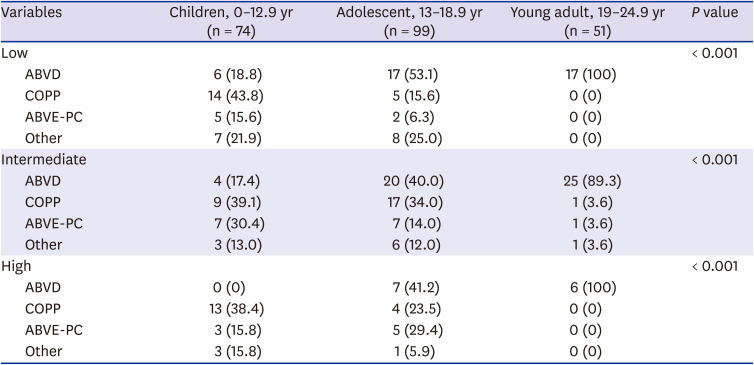
Table 2
Chemotherapy regimen used to treat Hodgkin's lymphoma according to age and risk group
Data are expressed as number (%).
ABVD = doxorubicin, bleomycin, vinblastine, dacarbazine, ABVE-PC = doxorubicin, bleomycin, vincristine, etoposide, prednisone, cyclophosphamide, COPP = cyclophosphamide, vincristine, procarbazine, prednisone.
![]()
HSCT
Out of 33 patients who underwent HSCT, three received two HSCTs and 21 (63.6%) were men. The mean age at the time of 1st HSCT was 17.1 ± 5.0 years (Table 3). The reasons for HSCT were relapse (21, 58.3%) and refractory/residual lesions (15, 41.7%). Partial response was the most common disease state at the time of HSCT. Autologous and peripheral blood were the most common donor and stem cell sources. The three patients who received two HSCTs were first transplanted with autologous stem cells, followed by a second transplant from a matched unrelated donor, matched related donor, and haploidentical donor, respectively.
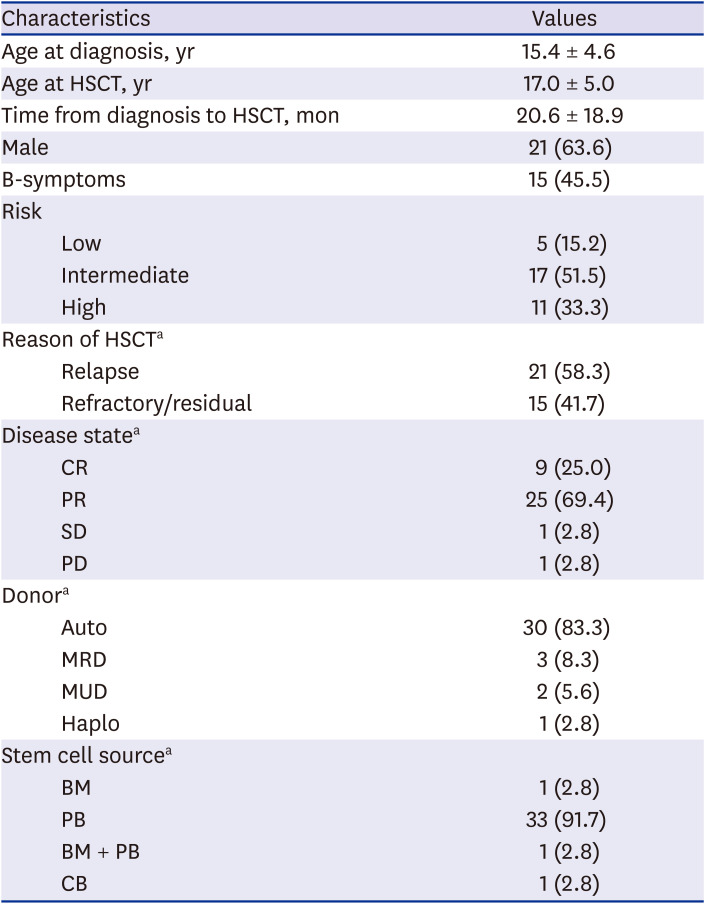
Table 3
Summary of transplantation
Data are presented as mean ± standard deviation or number (%).
HSCT = hematopoietic stem cell transplantation, CR = complete response, PR = partial response, SD = stable disease, PD = progressive disease, Auto = autologous, MRD = matched related donor, MUD = matched unrelated donor, BM = bone marrow, PB = peripheral blood, CB = cord blood.
aTwo of whom received two HSCTs.
![]()
Treatment outcome
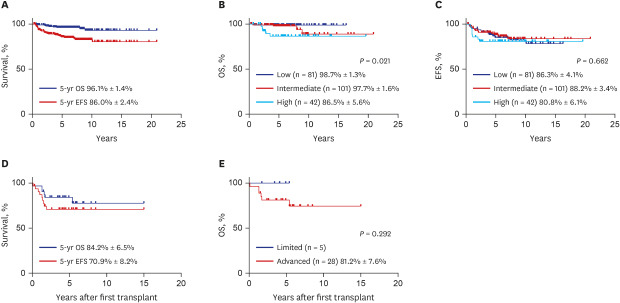
The 5-year OS and EFS rates were 96.1% ± 1.4% and 86.0% ± 2.4%, respectively (Fig. 2A). The 5-year OS rates were 98.7% ± 1.3%, 97.7% ± 1.6%, and 86.5% ± 5.6% in the low-, intermediate-, and high-risk groups, respectively (P = 0.021) (Fig. 2B). The 5-year EFS rates were 86.1% ± 4.1%, 88.2% ± 3.4%, and 82.8% ± 5.9% in the low-, intermediate-, and high-risk groups, respectively (P = 0.829) (Fig. 2C).
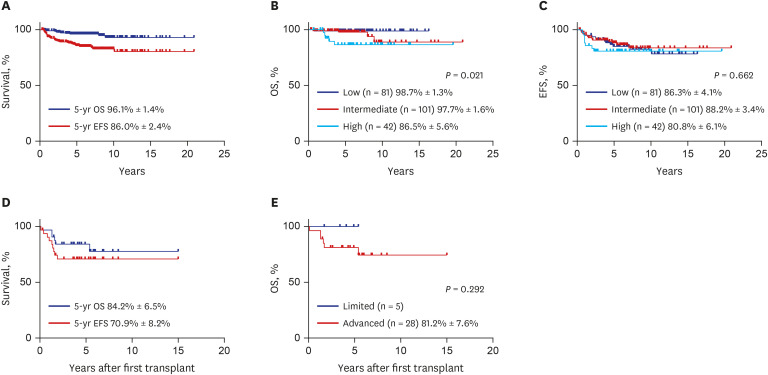
Fig. 2
Treatment outcome of study patients. (A) Five-year OS and EFS of study patients, (B) OS according to risk factors (OS, P = 0.021), (C) EFS according to risk factors (EFS, P = 0.662), (D) EFS and OS of patients treated with HSCT, (E) OS of HSCT patients according to risk factors (P = 0.268).
OS = overall survival, EFS = event-free survival, HSCT = hematopoietic stem cell transplantation.
![]()
Prognostic factor
The 5-year OS was worse in patients experiencing B-symptoms than in those without (89.5 ± 4.4 vs. 98.0 ± 1.1, P = 0.005), while the 5-year EFS rates did not differ significantly between the two groups (81.1 ± 5.4 and 87.6 ± 2.7, respectively; P = 0.172) (Table 4 and Supplementary Table 4). Patients with stage IV HL showed worse OS rates than those diagnosed with other stages (90.7 ± 4.0 vs. 98.0 ± 1.1, P = 0.009), although the corresponding difference in EFS was not significant (85.8 ± 4.6 and 86.1 ± 2.8, respectively, P = 0.858). The high-risk group demonstrated the worst OS compared to the combined OS of other two groups (86.5 ± 5.6 vs. 98.2 ± 1.0, P = 0.009), although the corresponding EFS rates did not differ significantly (80.8 ± 6.1 and 87.3 ± 2.6, respectively, P = 0.400). Factors such as age group, bulky disease, bone marrow involvement, and histopathological features did not affect the survival outcome. Patients with spleen and extra-nodal involvement showed a worse 5-year OS without impacting the EFS rate. Among laboratory findings, lactate dehydrogenase (LDH) level > 750 IU/L was the only factor showing a negative association with the 5 year-OS rates, while other laboratory results were not found to influence survival outcomes.
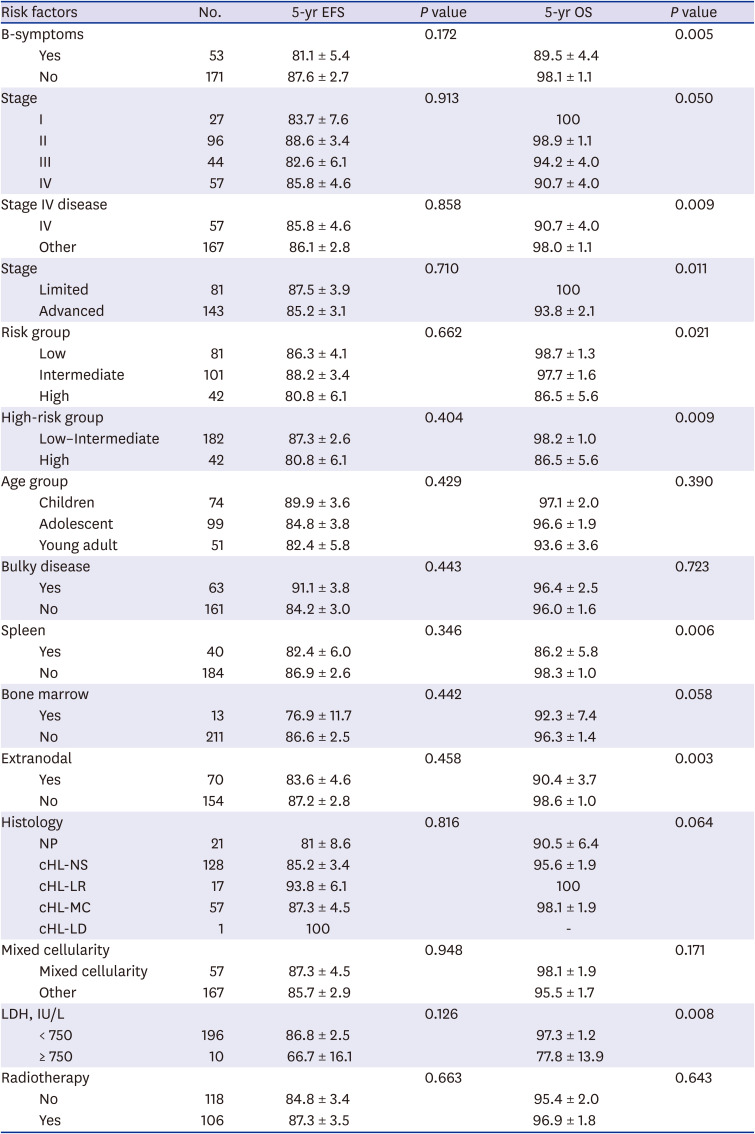
Table 4
Univariate analysis of survival
Data are presented as number or mean ± standard deviation.
LDH = lactate dehydrogenase, EFS = event-free survival, OS = overall survival, NP = nodular lymphocyte predominant, cHL = classic Hodgkin's lymphoma, NS = nodular sclerosis, LR = lymphocyte rich, MC = mixed cellularity, LD = lymphocyte depletion.
![]()
There was no difference in EFS and OS according to chemotherapy protocol. The EFS and OS rates of patients who received HSCT were 70.9% ± 8.2% and 84.2% ± 6.5%, respectively (Fig. 2D). All five patients in the limited stage who received HSCT survived. The five-year OS of 28 patients in the advanced stage who received HSCT was 81.2% ± 7.6% (P = 0.268) (Fig. 2E).
Radiotherapy did not influence either the EFS rate (84.8 ± 3.4 and 87.3 ± 3.5, respectively, P = 0.663) or the OS rate (95.4 ± 2.0 and 96.9 ± 1.8, respectively, P = 0.643) (Table 4). Furthermore, the use of radiotherapy was not found to affect EFS and OS in any of the risk groups (Table 5). In the multivariate analysis, B-symptoms and extra-nodal involvement were independent predictors of OS (Table 6). When analyzing the survival rate according to age and risk group, there was no difference in the 5-year EFS between age and risk group. The 5-year OS survival rate was significantly lower in the advanced stage of the high-risk group and the adolescent group of young adults (P = 0.006, P = 0.049) (Table 7).



Table 5
Survival rate according to risk group and RT
Data are presented as number or mean ± standard deviation.
RT = radiotherapy, EFS = event-free survival, OS = overall survival.
![]()
Table 6
Multivariate analysis for survival
| Variables | HR | 95% CI | P value |
|---|---|---|---|
| Stage IV | 1.78 | 0.35–9.17 | 0.491 |
| B-symptoms | 3.90 | 1.02–14.89 | 0.046 |
| Spleen | 2.65 | 0.74–9.46 | 0.135 |
| Extranodal | 4.65 | 1.17–18.46 | 0.029 |
| LDH, > 750 IU/L | 3.11 | 0.55–17.60 | 0.200 |
![]()
Table 7
Survival analysis according to age and risk group
![]()
Late complications
Thirty-five late complications were observed in 32 patients. Endocrine complications were the most common (n = 17), followed by 10, 6, and 2 cases of pulmonary complications, secondary malignant neoplasm (SMN), and cardiac complications, respectively. Endocrine complications included thyroid disease, osteoporosis, type 2 diabetes mellitus, and metabolic syndrome in 13, 3, 2, and 1 patient, respectively. Secondary malignancies were constituted by 4, 1, and 1 case of thyroid cancer, breast cancer, and other malignancy, respectively. Endocrine complications occurred more frequently in patients who received radiotherapy (P = 0.046, odds ratio, 2.885) (Table 8). The time taken to diagnose complications after HL diagnosis was 4.7 ± 3.0 years for SMNs, 3.7 ± 2.9 years for endocrine complications, 1.1 ± 0.4 years for cardiac complications, and 4.9 ± 3.9 years for pulmonary complications.

DISCUSSION
The present study evaluated the clinical characteristics and treatment outcomes of HL among pediatric and young adult patients in Korea. The incidence of HL in East Asia, including Japan and China, is lower than that in Western countries. Nonetheless, the distribution of HL in European and American populations showed the incidence in male patients to be double that in female patients. However, in the adolescent population, there was an equal distribution of the disease between both sexes. HL commonly affects young adults worldwide, showing a 2:1 and 3.5:1 male-to-female sex ratio in Western countries (Europe and the United States) and in Asia, respectively.917 In this study, the male-to-female sex ratio was 3.6:1 and 2:1 in children and adolescents, respectively. Conversely, the percentage of the female sex in this study was higher than that of the male sex among young adults aged > 19 years.
There are significant differences in the distribution of these subtypes by age.19 The NS type of classic HL, which is the most common subtype, constitutes 80% of cases in the adolescent and young adult population; however, it is more commonly observed in children (around 40%–50% of cases). The MC subtype is found in 30% of all HL patients and is more commonly observed in the pediatric age group. In this study, the NS subtype of HL occurred in 39.2%, 67.1%, and 62.7% of children, adolescents, and young adults, respectively. The MC subtype is found in 40.5% of all HL patients and is more commonly observed in children.
Foltz et al.3 using data from the British Columbia cancer database conducted a study of adolescents (16–21 years) and young adults (22–45 years) who underwent chemotherapy for HL as per the established treatment protocol for adults in Canada. Overall, 38%, 49%, and 13% of adolescents in the study were treated only with radiation, only with chemotherapy, or with a combination of both modalities, respectively. Five-year progression-free survival (PFS) and OS rates of adolescents were 83% and 94%, respectively. Five-year PFS and OS rates in patients with limited-stage disease were 95% and 99%, respectively, and those in patients with advanced-stage disease were 76% and 92%, respectively. In their study, adolescent and young adults achieved similar outcomes when treated using the same therapeutic protocol.3
In this study, all patients received chemotherapy, and 47.3% of patients received a combination of chemotherapy and radiotherapy. The 5-year EFS and OS rates of adolescents were 84.8% ± 3.8% and 96.6% ± 1.9%, respectively. In patients with a limited-stage disease, EFS and OS rates were 87.5% ± 3.9% and 100%, respectively. In patients with advanced-stage disease, EFS and OS rates were 85.2% ± 3.1% and 93.8% ± 2.1%, respectively. In this study, the survival rate was similar or better than that reported in the Canadian study. The differences in treatment modality and different chemotherapy protocols used in adolescents and young adults appear to have influenced the treatment outcome.
Englund et al.8 conducted a study in Sweden and Denmark of 1,072 classic HL patients who were < 24 years of age. The authors reported that EFS in Danish patients was lower than that in Swedish patients because they received radiotherapy less frequently than did Danish pediatric patients. Nevertheless, the OS was similar in both countries. Moreover, no nationality-based variation in OS was observed between pediatric and adult populations.
In our study, radiotherapy did not influence either the EFS or OS rates. The OS according to radiotherapy was similar among the three risk groups. Furthermore, EFS was slightly but non-significantly higher in the low- and intermediate-risk group patients who received radiotherapy.
To limit the cumulative exposure to alkylating agents and to reduce the required dose of radiation The Children Oncology Group (COG) conducted the AHOD0831 study of pediatric high-risk HL patients using a response-based approach.18 The 5-year EFS and OS rates were 79.1% and 95%, respectively, in children with high-risk HL. Despite the application of a reduced volume of radiation, EFS and OS rates were comparable with those observed in the recent trial study.18 In this study, the 5-year EFS and OS rates of high-risk HL were 80.8% ± 6.1% and 86.5% ± 5.6%, respectively; the use of radiotherapy did not significantly affect OS. Additionally, in this study, the OS and EFS were lower in the high-risk group than in the intermediate-risk group. After relapse, the intermediate-risk group showed improved long-term survival with salvage treatment; however, the high-risk group did not.
Moreover, COG developed the Childhood Hodgkin International Prognostic Score (CHIPS) for predicting EFS in childhood HL. They developed a predictive model for estimating EFS in pediatric/adolescent HL patients using diagnostic clinical data of 1,103 intermediate-risk HL patients treated using the COG AHOD0031 protocol. Stage IV disease, large mediastinal mass, decreased albumin level (< 3.5 g/dL), and fever were independent predictors of EFS that were each assigned 1 point on the CHIPS scale. The 4-year EFS was 93.1%, 88.5%, 77.6%, and 69.2% in patients with CHIPS of 0–3, respectively.14 Contrastingly, the current analysis revealed no significant predictor of EFS in pediatric and young adult patients with HL. However, factors including B-symptoms, stage IV disease, high-risk patients, spleen and extra-nodal involvement, and levels of LDH ≥ 750 IU/L were found to be predictors of poor OS. In the multivariate analysis, B-symptoms and extra-nodal involvement were found to be independent predictors of OS.
With respect to the histologic types of HL, the proportion of NS was comparatively low and that of MC was comparatively high in children versus the other age groups. Further, with respect to staging, the proportion of stage I was comparatively high in children versus those in the other age groups. It is possible that the inclusion of a high proportion of MCs and stage I patients in the children group affected OS and EFS in children. However, the difference was not statistically significant because the overall treatment outcome for HL was good.
An analytical study by Kahn et al.,19 conducted from 2002 to 2012, used pooled, individual-level data from 1,605 patients (aged < 1–21 years) enrolled in phase III trials for the treatment of patients with low-risk (AHOD0431 protocol), intermediate-risk (AHOD0031 protocol), and high-risk (AHOD0831 protocol) HL. At the median follow-up of 6.9 years, the cumulative relapse incidence was 17%, while the 5-year EFS and OS rates were 83% ± 1.2% and 97% ± 1.0%, respectively. In the current study, the 5-year EFS and OS rates were 86.0% ± 2.4% and 96.1% ± 1.4%, respectively, which were comparable to those of the large-scale study, despite the application of different treatment protocols by different institutions.
High-dose chemotherapy and autologous stem cell transplantation can salvage 40%–70% of patients with relapsed or refractory HL. Achieving complete hematologic remission before transplantation has a good effect on prognosis.2021 The ideal timing and order of treatment administration are yet to be determined.22 In our study, 34 (15.2%) patients received HSCT for relapsed or residual disease after completion of frontline therapy. The OS rate of patients who received HSCT was 84.4% ± 6.4%, which was better than that observed in previous adult HL studies.2324 The OS rate was also better in the low-risk group.
There is a recognized “cost of cure” due to the occurrence of late toxicities associated with treatment and long-term psychosocial sequelae in adolescents and young adults with HL. Although there have been efforts to reduce the dosage of radiation or altogether eliminate its application, those who receive this treatment modality are at risk of developing a variety of late toxicities, most notably SMN and cardiovascular disease.2526 The risk of cancer, specifically breast, lung, and gastrointestinal malignancies, is directly related to the radiation dosage.2728 The development of a second malignancy is the leading cause of death among long-term HL survivors.26 Patients not receiving radiotherapy may also be at increased risk of developing secondary malignancies such as leukemia, due to exposure to chemotherapeutic treatment. While chemotherapeutic regimens such as ABVD do not appear to increase the risk of leukemia, more intensive regimens such as BEACOPP, are thought to be leukemogenic.29 The current findings indicate that radiation appeared to increase the occurrence of endocrine complications and that patients receiving radiation are at an increased risk of developing a second malignancy.
Endocrine problems commonly experienced in HL survivors include thyroid dysfunction, decreased bone mineral density, and gonadal dysfunction, which are highly influenced by alkylating agents and radiotherapy.3031 Furthermore, fertility preservation and reproductive health are significant concerns in adolescents and young adults with HL.32 However, we found no reported cases of this complication in our study, although this outcome may have been underdiagnosed.
In order to prevent late complications such as thyroid dysfunction, cardiotoxicity, pulmonary toxicity, and SMN due to radiation, it is necessary to reduce the volume of normal tissue exposed to radiation through the tailored application of radiotherapy and the introduction of new techniques such as IMRT or proton therapy. Alkylating agents and anthracycline cumulative dose reduction through the introduction of novel agents could be another way to achieve this. In addition, early detection through survivorship screening program is important.33
Collaborative multinational and multicenter efforts have led to significant improvements in pediatric HL treatment.1518 The goal of HL treatment research should be to develop therapies that minimize treatment toxicity while maximizing the cure rate. Recently, novel monoclonal antibodies such as brentuximab and anti-PD1 agents have been shown to increase complete remission rates and reduce myelotoxicity.10 Therefore, efforts have been made to add them to conventional chemotherapeutic regimens.
The main limitation of this study is that children under 18 years of age were surveyed through a nationwide multicenter study; however, not all young adult patients (19–24.9 years old) were enrolled because not all institutions participated in our study. Therefore, more careful consideration should be given to understanding the therapeutic results and characteristics of young adults. In addition, as HL has a low incidence and high rate of cure, late complications are getting increased attention and are important in survivors. This retrospective study could have been more informative if outcomes of HL were evaluated over 20 years instead of 10 years. Therefore, a follow-up study over a longer duration with the patients included in this study would provide more insights.
In children and young adults, it is important to maintain a good balance between cure rate and prevention of long-term toxicity, as this will have a sizable impact on their lives in the future. In addition to the development of a unified nationwide protocol for the management of HL, studies are needed concerning the appropriate introduction of new drugs such as brentuximab vedotin, and immunotherapy.
 XML Download
XML Download