

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
SEARCH STRATEGY AND METHODS
THE CNS COMPLICATIONS AND POSSIBLE MECHANISMS OF COVID-19
Direct pathway to brain
Indirect pathway by immune and inflammatory reaction
Hypoxic brain damage by COVID-19
IMPACT OF COVID-19 ON PATIENTS WITH COGNITIVE IMPAIRMENT
Risk factors of dementia vulnerable to COVID-19
Difficulties of dementia amid COVID-19 pandemic
MCI
AD
VD
Dementia with Lewy bodies
FTD
Dire effects of COVID-19 on dementia care
STRATEGY FOR MANAGING DEMENTIA DURING THE COVID-19 PANDEMICS
General preventive measures of COVID-19 infection
Table 1
General preventive measures of COVID-19 infection

![]()
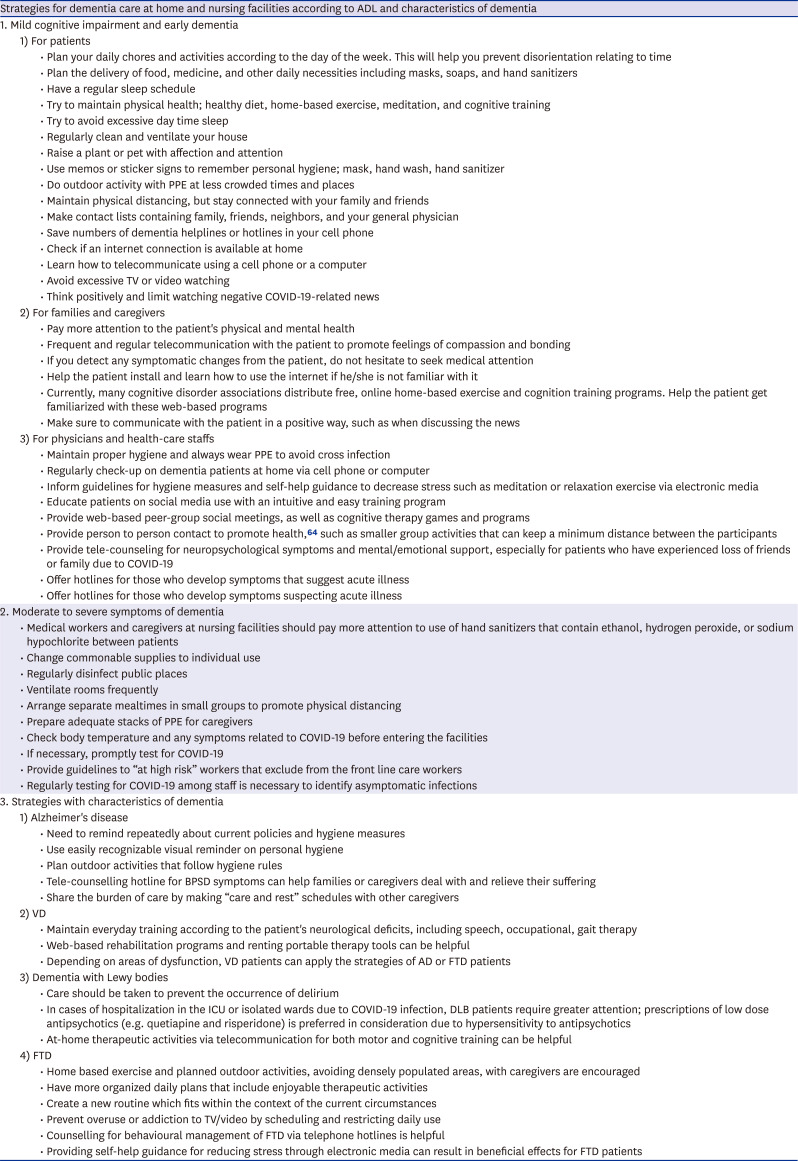
Strategies for dementia care at home and nursing facilities according to ADL and characteristics of dementia
MCI and early dementia
1) For patients
• Try to maintain in healthy condition; healthy diet, home-based exercise, meditation, and cognitive training68697071
• Plan your daily chores and activities according to the day of the week6972
• Plan the delivery of food, medicine, and other daily necessities including masks, soaps, and hand sanitizers72
• Use reminder memos or sticker signs to remember personal hygiene against infection; mask, hand wash, hand sanitizer6972
• Have a regular sleeping schedule72
• Try to avoid excessive day time sleep69
• Avoid excessive TV watching or video viewing
• Do outdoor activity with personal protective equipment (PPE) at less crowded times and places
• Keep physical distancing, but stay emotionally connected with your family and friends
• Make a list of contacts of family, friends, neighbors, and your general physicians to contact you when needed677173
• Save numbers of dementia helplines or hotlines in your cell phone71
• Check if an internet connection is available at home
• Learn how to telecommunicate using a cell phone or a computer74
• Think positively and limit watching negative COVID-19-related news6972
2) For families and caregivers
• Pay more attention to patients' physical and mental health75
• Frequent and regular telecommunication with the patient to promote feelings of compassion and bonding6772
• If you detect any symptomatic changes from the patient, do not hesitate to seek medical attention
• Help the patient install and learn how to use the internet if he/she is not familiar with it66
• Currently, many cognitive disorder associations distribute free, online home-based exercise and cognition training programs. Help the patient get familiarized with these web-based programs
• Make sure to communicate with the patient in a positive way, especially when discussing the news
3) For physicians and health-care staffs
• Maintain proper hygiene and always wear PPE to avoid cross infection76
• Perform regular health check-ups on dementia patients at home via cell phone or computer
• Inform guidelines for hygiene measures and self-help guidance to decrease stress such as meditation or relaxation exercise via electronic media64
• Educate patients how to use social media with intuitive and easy training program72
• Provide web-based peer group social meeting, cognitive therapy games and programs 72
• Provide person to person contact to promote health,64 such as smaller group activities that can keep a minimum distance between the participants
• Provide tele-counselling for neuropsychological symptoms and mental/emotional support, especially for patients who have experienced loss of friends or family due to COVID-1964
• Offer hotlines for those who develop symptoms that suggest acute illness686972
Moderate to severe symptoms of dementia
Table 2
Strategies for dementia care at home and nursing facilities according to ADL and characteristics of dementia
| Strategies for dementia care at home and nursing facilities according to ADL and characteristics of dementia | ||
|---|---|---|
| 1. Mild cognitive impairment and early dementia | ||
| 1) For patients | ||
| • Plan your daily chores and activities according to the day of the week. This will help you prevent disorientation relating to time | ||
| • Plan the delivery of food, medicine, and other daily necessities including masks, soaps, and hand sanitizers | ||
| • Have a regular sleep schedule | ||
| • Try to maintain physical health; healthy diet, home-based exercise, meditation, and cognitive training | ||
| • Try to avoid excessive day time sleep | ||
| • Regularly clean and ventilate your house | ||
| • Raise a plant or pet with affection and attention | ||
| • Use memos or sticker signs to remember personal hygiene; mask, hand wash, hand sanitizer | ||
| • Do outdoor activity with PPE at less crowded times and places | ||
| • Maintain physical distancing, but stay connected with your family and friends | ||
| • Make contact lists containing family, friends, neighbors, and your general physician | ||
| • Save numbers of dementia helplines or hotlines in your cell phone | ||
| • Check if an internet connection is available at home | ||
| • Learn how to telecommunicate using a cell phone or a computer | ||
| • Avoid excessive TV or video watching | ||
| • Think positively and limit watching negative COVID-19-related news | ||
| 2) For families and caregivers | ||
| • Pay more attention to the patient's physical and mental health | ||
| • Frequent and regular telecommunication with the patient to promote feelings of compassion and bonding | ||
| • If you detect any symptomatic changes from the patient, do not hesitate to seek medical attention | ||
| • Help the patient install and learn how to use the internet if he/she is not familiar with it | ||
| • Currently, many cognitive disorder associations distribute free, online home-based exercise and cognition training programs. Help the patient get familiarized with these web-based programs | ||
| • Make sure to communicate with the patient in a positive way, such as when discussing the news | ||
| 3) For physicians and health-care staffs | ||
| • Maintain proper hygiene and always wear PPE to avoid cross infection | ||
| • Regularly check-up on dementia patients at home via cell phone or computer | ||
| • Inform guidelines for hygiene measures and self-help guidance to decrease stress such as meditation or relaxation exercise via electronic media | ||
| • Educate patients on social media use with an intuitive and easy training program | ||
| • Provide web-based peer-group social meetings, as well as cognitive therapy games and programs | ||
| • Provide person to person contact to promote health,64 such as smaller group activities that can keep a minimum distance between the participants | ||
| • Provide tele-counseling for neuropsychological symptoms and mental/emotional support, especially for patients who have experienced loss of friends or family due to COVID-19 | ||
| • Offer hotlines for those who develop symptoms that suggest acute illness | ||
| • Offer hotlines for those who develop symptoms suspecting acute illness | ||
| 2. Moderate to severe symptoms of dementia | ||
| • Medical workers and caregivers at nursing facilities should pay more attention to use of hand sanitizers that contain ethanol, hydrogen peroxide, or sodium hypochlorite between patients | ||
| • Change commonable supplies to individual use | ||
| • Regularly disinfect public places | ||
| • Ventilate rooms frequently | ||
| • Arrange separate mealtimes in small groups to promote physical distancing | ||
| • Prepare adequate stacks of PPE for caregivers | ||
| • Check body temperature and any symptoms related to COVID-19 before entering the facilities | ||
| • If necessary, promptly test for COVID-19 | ||
| • Provide guidelines to “at high risk” workers that exclude from the front line care workers | ||
| • Regularly testing for COVID-19 among staff is necessary to identify asymptomatic infections | ||
| 3. Strategies with characteristics of dementia | ||
| 1) Alzheimer's disease | ||
| • Need to remind repeatedly about current policies and hygiene measures | ||
| • Use easily recognizable visual reminder on personal hygiene | ||
| • Plan outdoor activities that follow hygiene rules | ||
| • Tele-counselling hotline for BPSD symptoms can help families or caregivers deal with and relieve their suffering | ||
| • Share the burden of care by making “care and rest” schedules with other caregivers | ||
| 2) VD | ||
| • Maintain everyday training according to the patient's neurological deficits, including speech, occupational, gait therapy | ||
| • Web-based rehabilitation programs and renting portable therapy tools can be helpful | ||
| • Depending on areas of dysfunction, VD patients can apply the strategies of AD or FTD patients | ||
| 3) Dementia with Lewy bodies | ||
| • Care should be taken to prevent the occurrence of delirium | ||
| • In cases of hospitalization in the ICU or isolated wards due to COVID-19 infection, DLB patients require greater attention; prescriptions of low dose antipsychotics (e.g. quetiapine and risperidone) is preferred in consideration due to hypersensitivity to antipsychotics | ||
| • At-home therapeutic activities via telecommunication for both motor and cognitive training can be helpful | ||
| 4) FTD | ||
| • Home based exercise and planned outdoor activities, avoiding densely populated areas, with caregivers are encouraged | ||
| • Have more organized daily plans that include enjoyable therapeutic activities | ||
| • Create a new routine which fits within the context of the current circumstances | ||
| • Prevent overuse or addiction to TV/video by scheduling and restricting daily use | ||
| • Counselling for behavioural management of FTD via telephone hotlines is helpful | ||
| • Providing self-help guidance for reducing stress through electronic media can result in beneficial effects for FTD patients | ||
![]()
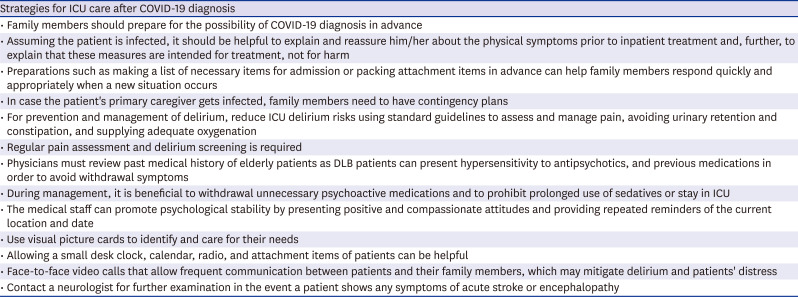
Strategies for ICU care after COVID-19 diagnosis
Table 3
Strategies for ICU care after COVID-19 diagnosis
![]()
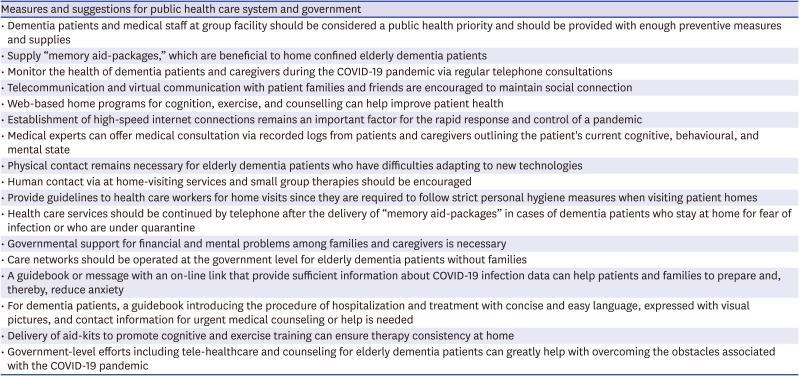
Measures and suggestions for public health care system and government
Table 4
Measures and suggestions for public health care system and government
![]()
 XML Download
XML Download