

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since its first isolation from Actinoplanes teichomyceticus in 1970s, teicoplanin has become one of the widely used glycopeptides along with vancomycin for treating gram-positive bacterial infections.1 Compared to vancomycin, teicoplanin has several advantages, including a lower incidence of adverse events like nephrotoxicity and longer half-life, allowing once-daily bolus injection.234
In general, optimal trough plasma levels of teicoplanin for treatment have been considered to be at least 10 μg/mL, although trough levels of 20–60 μg/ml are permissive for severe staphylococcal infections including endocarditis and bone-and-joint infection.5 Trough levels over 60 μg/mL are known to be associated with adverse effects such as nephrotoxicity.67
Despite its wide use in various clinical settings, data on teicoplanin trough level in pediatric patients are limited. The aim of this study was to demonstrate the therapeutic drug level monitoring of teicoplanin in Korean pediatric patients including ones with impaired renal function, and its treatment effect for gram-positive bacteremia.
METHODS
Data source and patient selection
Trough levels of teicoplanin in pediatric inpatients 18 years old or younger at Samsung Medical Center, Sungkyunkwan University School of Medicine between September 2014 and April 2018 were collected. Medical records were retrospectively reviewed to collect clinical information. Distribution and characteristics of trough levels in patients with decreased renal function and those with bacteremia were also assessed. Patients who were included in this study were 18 years old or younger who received teicoplanin for at least 4 doses and had available exam data of trough levels. Process of data exclusion is described in Supplementary Fig. 1.
The authors defined decreased renal function as estimated glomerular filtration rate (eGFR) less than 70 mL/min/body surface area (BSA),8 which was calculated with modified Schwartz equation (K × height in centimeter/plasma creatinine [mg/dL], K = 0.413).
Within bacteremia population, patients were regarded to be at defervescence if body temperature lower than 37.5°C was achieved for at least 48 hours.
Administration and drug level monitoring of teicoplanin
Teicoplanin was administered intravenously. Study population received teicoplanin at a loading dose of 10 mg/kg/dose at 12 hours' interval, three times in a row. Maintenance dose was commenced at a dose of 10 mg/kg/dose 24 hours after the last loading dose. The maximal dose of administered teicoplanin was 400 mg. Trough levels of teicoplanin were measured with liquid chromatography-tandem mass spectrometry method at the Department of Laboratory Medicine and Genetics of the Samsung Medical Center. Detailed information on standard materials used, preparations of calibrators, quality controls, instrumental condition, and method validation were described in a previous study.9
Steady state sample was defined as the one collected after the fourth or fifth dose of teicoplanin. Drug levels were measured within seven days from the initial dose after reaching steady state in this study. Each of the episodes were considered to be separate if a duration between the last dose of previous teicoplanin and the first dose of restart is 5 days or more.
Statistical analysis
Descriptive data are expressed as median and ranges. The χ2 test and Mann-Whitney U test were used to compare categorical and continuous variables, respectively. Differences in the achievement of target trough level (≥ 10 μg/mL) were evaluated for statistical significance with logistic regression models. Patient age, sex, body weight, serum creatinine, eGFR, interval between initial dose and 1st steady state exam, loading and maintenance doses were included as covariates. Analyses were done with IBM SPSS Statistics, version 25 (SPSS Inc., Chicago, IL, USA). Statistical significance was defined by a two-sided P value < 0.05.
RESULTS
Patient characteristics
A total of 187 trough levels were collected from 143 patients (Table 1), including 74 (51.7%) males. The median age of all patients was 6.2 years (range, 0.09–17.7 years). Hematologic and oncologic diseases were the most common underlying diseases (n = 119, 83.2%), followed by gastroenterologic and hepatologic disease (n = 6, 4.2%), primary immunodeficiencies (n = 5, 3.5%), neurologic disease, and cardiologic diseases (n = 3, 2.1% respectively). The most common reason of teicoplanin use was empiric treatment for prolonged neutropenic fever in hematologic and oncologic disease (n = 143, 75.5%).
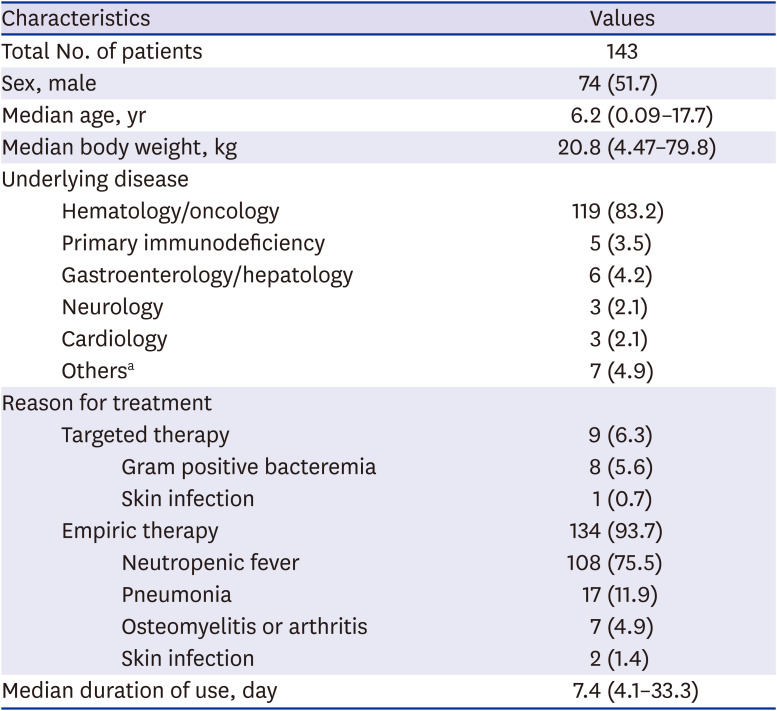
Table 1
Patients' characteristics
Values are presented as number (%) or median (range).
aChronic kidney disease (n = 1), chronic pneumonitis of infancy (n = 1), lymphangioma (n = 3), myopathy (n = 1), infantile myofibromatosis (n = 1).
![]()
Teicoplanin trough levels
Among 187 measured trough levels, 180 were first-measured-values. The median value of 1st measured trough levels was 16.2 μg/mL (range, 2.3–100 μg/mL). Interval between initial teicoplanin injection and 1st trough level ranged from 47.6 hours to 179.3 hours and median was 96.5 hours. Data were divided into two groups based on trough levels: trough level < 10 μg/mL (n = 44, 24.4%) and trough level ≥ 10 μg/mL (n = 136, 75.6%). There were 77 data (42.8%) of which trough levels were between ≥ 10 μg/mL to < 20 μg/mL and 55 data (30.6%) for ≥ 20 μg/mL to < 60 μg/mL. Four trough levels (2.2%) were over 60 μg/mL which is generally considered as toxic level. Characteristics of these patients are described in Supplementary Table 1. Patients whose steady state trough level was less than 10 μg/mL tended to be younger, have lower body weight, have longer interval between the 1st injection and trough level measurement, and have better kidney function (Table 2). Patients were also divided into two groups based on age: patients < 6 years old (infants and young children) vs. patients ≥ 6 years old (school-aged children and adolescents). Although trough levels in both groups were within optimal therapeutic range, lower steady state levels were observed in the younger age group (median: 13.5 vs. 18.0 μg/ml, P = 0.038). In a logistic regression model, patients whose trough levels were within target range tended to have higher body weight, shorter interval between initial injection and trough level measurement, lower eGFR, higher maintenance dose (Supplementary Table 2).
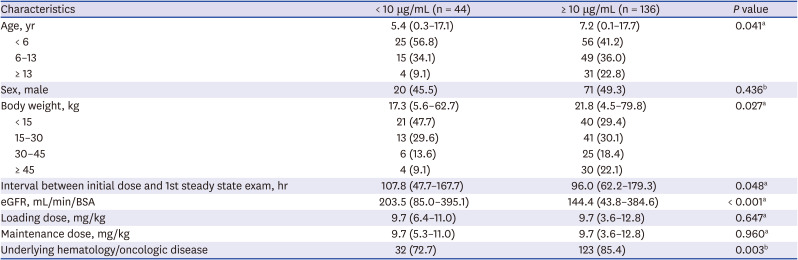
Table 2
Comparison of characteristics by teicoplanin trough levels
Values are presented as number (%) or median (range).
eGFR = estimated glomerular filtration rate, BSA = body surface area.
aMann-Whitney U test; bχ2 test.
![]()
Patients with decreased renal function vs. normal renal function
Eight patients had decreased renal function (median eGFR: 62.6 mL/min/BSA, range: 43.8–66.5 mL/min/BSA). Of these patients, four received renal replacement therapy including one patient who had received both peritoneal dialysis and continuous renal replacement therapy (Table 3).
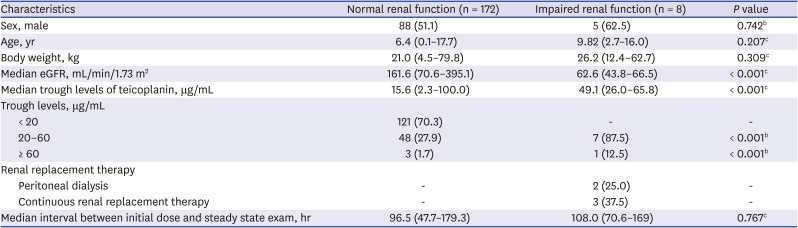
Table 3
Normal vs. impaired renal functiona
Values are presented as number (%) or median (range).
eGFR = estimated glomerular filtration rate.
aeGFR less than 70 mL/min/1.73 m2; bχ2 test; cMann-Whitney U test.
![]()
Median trough levels at steady-state were significantly higher in this group with decreased renal function than in patients with normal renal function (median trough level: 49.1 vs. 15.6 μg/mL, P < 0.001) (Fig. 1). All trough levels at steady-state in these patients were over 20 μg/mL. One patient showed trough level over 60 μg/mL. Compared to patients with normal renal function, patients with decreased renal function showed no statistical differences in loading dose, maintenance dose, or interval between the initial dose and measurement of trough level.
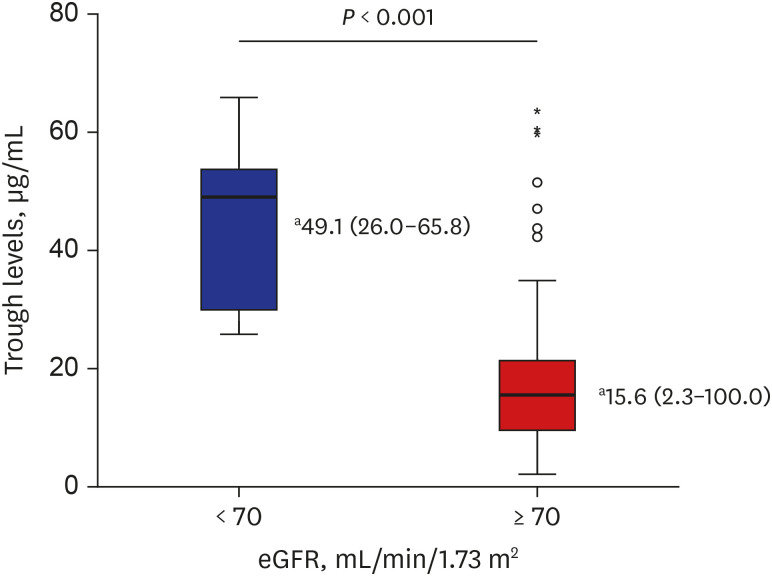
Fig. 1
Steady state trough levels: decreased vs. normal renal function.
Differences in steady state trough levels between patients with decreased renal function and those with normal renal function. Decreased renal function was defined as eGFR less than 70 mL/min/BSA, calculated with modified Schwartz equation.
BSA = body surface area, eGFR = estimated glomerular filtration rate.
aMedian (range).
![]()
Patients with gram positive bacteremia
Eight patients had gram-positive bacteremia in the study population (Table 4). All patients with gram-positive bacteremia had normal renal function (median eGFR: 147.7 mL/min/BSA, range, 98.0–209.0 mL/min/BSA). Median trough level at steady-state was 11.2 μg/mL (range, 8.2–19.3 μg/mL). Three patients failed to reach optimal trough level even at steady-state after five to seven doses of teicoplanin. Staphylococcus aureus was the most common pathogen (n = 4, 50%), followed by Viridans streptococci (n = 2, 25%) and Enterococcus gallinarum (n = 1) or coagulase negative staphylococci (n = 1). These eight isolates were sensitive to teicoplanin (n = 6) or vancomycin (n = 7).
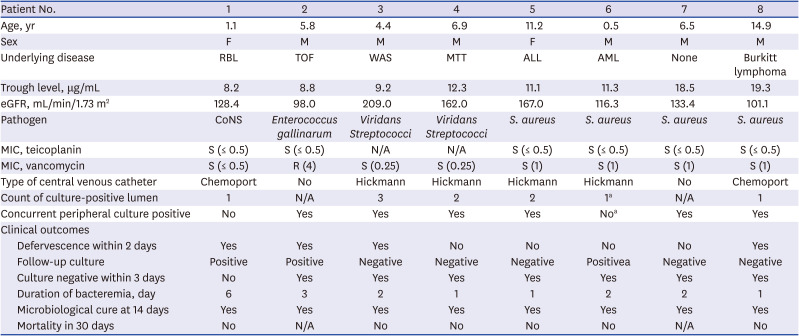
Table 4
Patients with gram positive bacteremia
RBL = retinoblastoma, TOF = tetralogy of Fallot, WAS = Wiskott-Aldrich syndrome, MTT = malignant triton tumor, ALL = acute lymphoblastic leukemia, AML = acute myelogenous leukemia, eGFR = estimated glomerular filtration rate, CoNS = coagulase-negative Staphylococci, S. aureus = Staphylococcus aureus, MIC = minimal inhibitory concentration, S = sensitive, R = resistant, N/A = not available.
aFrom follow-up blood culture performed within 24 hours, organism was reported in two central lumens with peripheral blood culture concurrently.
![]()
In seven patients (except patient 1), blood culture became negative within three days from the initial blood culture. All the patients reached microbiological cure within 14 days. Defervescence was achieved within a median of 4.5 days (range, 2–13 days). In three patients who did not reach target trough level (patient number: 1, 2, and 3), bacteremia resolved by 14 days, although patient 1 had persistent bacteremia for 3 days.
Four patients had changes in their initial antibiotic agents during treatment. Two patients had change of teicoplanin to vancomycin. One patient (patient 6) had this change of antibiotics because he developed S. aureus bacteremia while he was receiving teicoplanin as an empirical therapy for neutropenic fever. One patient (number 5) started teicoplanin when she developed S. aureus bacteremia. She received teicoplanin for 5 days. After that, she had vancomycin for continuation. Two patients (patient number: 2 and 7) had change of vancomycin to teicoplanin due to adverse reaction to vancomycin (drug rash and drug fever, respectively) and achieved cure for the bacteremia.
DISCUSSION
This study provides information on the pharmacokinetics of teicopalnin in pediatric patients with decreased renal function. In addition, in a subset of patients with gram-positive bacteremia, teicoplanin showed favorable treatment effect. Although the number is low, this observation would be helpful for physicians in the field when prescribing teicoplanin in high-risk pediatric patients with a wide range of age, variable renal functions, and serious invasive bacterial infection.
Pharmacokinetics of teicoplanin has been steadily studied in various clinical settings, including adult patients,510111213 pediatric patients,14151617181920 and patients with hematologic malignancies.2122232425 A number of studies on the pharmacokinetics of teicoplanin have shown a common problem that the therapeutic range of trough level is not achieved early and occasionally not reached even at steady state. To overcome this problem, the need of loading dose has been suggested.3526 Chae et al.27 have demonstrated that the proportion of trough levels achieving ≥ 10 mg/L is only 20% (days 3–5) or 38% (days 6–8) in the standard dose group. Nah et al.12 have reported that patients with sub-optimal (< 10 mg/L) plasma teicoplanin concentrations constituted nearly half of their total study population. The majority of these patients received the recommended loading dose (three doses of 400 mg administered every 12 hours). Kim et al.11 have reported that a high loading dose regimen (≥ 9 mg/kg) was associated with adverse events during treatment. To weigh the balance between optimal treatment efficacy and increased risk of adverse events, therapeutic drug monitoring is necessary in these critically ill patients who require teicoplanin treatment.6121327
This issue becomes more complicated in pediatric settings due to a higher clearance in younger children which leads to age-related differences in serum teicoplanin levels. In early studies, Reed et al.17 enrolled twelve infants and children and Sanchez et al.18 recruited twenty-one critically ill children and measure teicoplanin drug levels. They did not observe any statistical differences in mean serum concentration or pharmacokinetic characteristics among different age groups. Strenger et al.19 performed a large-scale study and analyzed 1,357 samples in 280 patients and reported that toddlers (1.0–5.9 years) had significantly lower trough levels of teicoplanin, with a 2-fold higher risk of suboptimal level (< 10 mg/L). We also observed an age-related difference in trough levels at steady state when comparing two age groups (< 6 vs. ≥ 6 years old) with lower steady state levels found in the younger age group.
Another important issue described in this study is trough level distribution in patients with impaired renal function. Since the therapeutic efficacy of teicoplanin is not inferior to vancomycin with lesser renal toxicity, teicoplanin is preferred in patients with decreased renal function.2829 Previous studies were mostly confined to adult population with various settings of renal replacement therapy since the early era of teicoplanin.3031323334 In those studies, adult patients with renal failure tended to have prolonged half-life and reduced total body clearance of teicoplanin, while volume of distribution varied. Lam et al.35 have suggested a nomogram for dosage adjustment in adults with varying degrees of renal failure. Pharmacokinetics studies of teicoplanin in pediatric patients with impaired renal function have been performed. However, most of them had a focus on the population pharmacokinetics model.1516 Moreover, in some pediatric studies, patients with impaired renal function were intentionally excluded.1720 Sanchez et al.18 included only one patient with a moderate alteration in renal function and failed to observe any difference in drug concentration. Our study included eight patients with decreased renal function. Steady state median trough levels were significantly higher in patients with eGFR less than 70 mL/min/BSA.
There are a couple of studies in which teicoplanin was used as a definite therapy for patients with gram-positive bacteremia. Dufort et al.14 reported that 76.2% (n = 16/21) of their pediatric subjects had gram-positive infection including eight bacteremia cases. However, their focus was on pharmacokinetic issue. They did not mention microbiological or clinical cure in their results. One prospective pediatric study reported teicoplanin treatment in 20 patients with gram-positive bacterial infection (13 S. epidermidis bacteremia, two E. fecium bacteremia, two methicillin-resistant S. aureus [MRSA] bacteremia, three MRSA pneumonia).36 All patients with gram-positive infection were cured. No relapse was noted in their study. In our study, eight patients had bacteremia due to gram-positive organisms. All eight patients were microbiologically cured at day 14 without any mortality. It was concerning that one patient developed breakthrough bacteremia while on teicoplanin therapy. However, two patients with gram-positive bacteremia finished their treatment course with teicoplanin when they developed adverse reaction to vancomycin. Overall, outcomes were favorable in seven of eight patients with bacteremia. Therefore, usefulness of teicoplanin should not be ignored and teicoplanin can be considered as a possible option for gram-positive bacteremia.
Our study has some limitations. First, this was a retrospective study that included only the first steady state levels. Details on dose modification and changes in serial trough levels were not analyzed in all patients. In addition, not all patients had albumin levels measured at the same time when the drug levels were measured. Second, this study did not analyze adverse events or safety in a systematic way. Third, because a small number of patients were enrolled, our observation on the treatment effect of teicoplanin in patients with gram-positive bacteremia needs to be interpreted with caution.
In conclusion, this study provides additive information on the therapeutic drug level monitoring of teicoplanin in children with impaired renal function and some treatment effect in patients with gram-positive bacteremia. Careful monitoring for steady state trough levels of teicoplanin is needed to determine the best dosing regimen to achieve optimal therapeutic levels for infants and young children.
 XML Download
XML Download