

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Asthma is a multifactorial chronic lung disease characterized by airflow obstruction and airway inflammation. Asthma is an extremely heterogeneous condition and can be classified into different subgroups, phenotypes, and endotypes.12 Asthma can be broadly divided into eosinophilic or non-eosinophilic, based on airway and peripheral blood immune cellular profiles.12
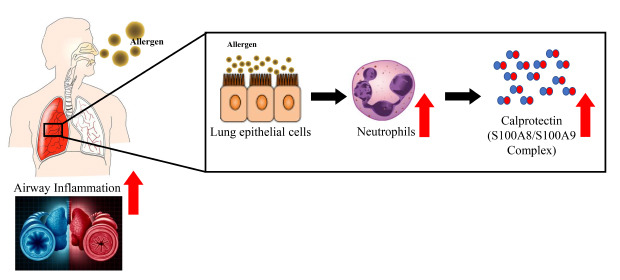
Calprotectin is a 36.5 kDa calcium- and zinc-binding protein and is the major cytosolic protein in neutrophil granulocytes.3 Fecal calprotectin levels have been proposed as a marker for the diagnosis and follow-up examination of various bowel diseases.345 Calprotectin is a heterodimeric complex consisting of S100A8 and S100A9, and has been associated with several inflammatory diseases, including inflammatory bowel disease, arthritis, psoriasis, and pulmonary infection.16 S100 proteins comprise a group of damage-associated molecular pattern molecules that bind and activate Toll-like receptor 4 (TLR4) and receptor for advanced glycation end-products (RAGE)1; S100-mediated TLR4 and RAGE activation has been implicated in a mice model of asthma.78 S100A8 and S100A9 are secreted from neutrophils and macrophages, yet their role in inflammatory immune responses remains elusive.
Pre-clinical and clinical studies have indicated an association between calprotectin and asthma. Importantly, S100A8 and S100A9 are upregulated in individuals with asthma compared with healthy individuals, and high levels of S100A8/S100A9 have been associated with more severe, uncontrolled disease phenotypes.9101112 S100A9 levels have been shown to correlate with the percentage of neutrophils in the sputum,12 suggesting that S100A9 may initiate and amplify neutrophilic inflammation in patients with uncontrolled, severe asthma. Exogenous treatment of S100A8 and S100A9 reduced Th2-mediated responses after allergic airway inflammation11314; however, a recent study using neutralizing antibodies against S100A8 and S100A9 did not prevent asthma in mice.15 The aim of this study was to assess calprotectin expression levels in a mouse model of asthma and to examine the association between calprotectin levels and clinicopathological characteristics in patients with asthma.
METHODS
Animals
All six-week-old female BALB/c mice received a total 10 μg of Aspergillus fumigatus crude antigen (Greer Laboratories, Lenoir, NC, USA) dissolved in 0.2 mL of incomplete Freund's adjuvant (Sigma-Aldrich, St. Louis, MO, USA). Half of this preparation was then deposited in the peritoneal cavity, and the remainder was delivered subcutaneously. Two weeks later, mice received 20 μg of A. fumigatus antigen dissolved in normal saline via the intranasal route. To induce allergic fungal asthma, A. fumigatus-sensitized mice received the intranasal route 20 μg of A. fumigatus antigen dissolved in normal saline after the third intranasal challenge (Fig. 1A).16 Airway responsiveness was measured, bronchoalveolar lavage fluid (BALF) was collected, and lung tissue was processed for protein and hematoxylin and eosin (H&E) stain, periodic acid-Schiff (PAS) and immunohistochemical (IHC) staining.17
Fig. 1
AHR and inflammation in Aspergillus fumigatus sensitization/challenge-mice. (A) A. fumigatus sensitization and challenge protocol. (B) AHR was more increased in A. fumigatus-mice compared to control mice. (C) Total and differential cell count in BALF. BALF was collected on 25 day. Total and differential cell count was increased in A. fumigatus sensitization and challenge mice compared to control mice.
AHR = airway hyperresponsiveness, BALF = bronchoalveolar lavage fluid, I.P. = intraperitoneal, I.N. = intranasal, BAL = bronchoalveolar lavage.
*P < 0.05, A. fumigatus vs. Sham.

Western blotting
Protein extracts of mouse lung tissue were collected as previously described.17 Proteins were separated by 10% sodium dodecyl-sulfate polyacrylamide gel electrophoresis and transferred onto polyvinylidene fluoride membranes (Millipore, Burlington, MA, USA). The membranes were blocked in Tris-buffered saline containing 5% skimmed milk and 0.1% Tween-20 for 1 hour at room temperature before incubating with the rabbit anti-calprotectin antibody (1:500; MyBioSource, San Diego, CA, USA) and S100A8 antibody (1:1,000; Abnova, Taipei, Taiwan), S100A9 antibody (1:1,000; Abcam, Cambridge, UK) overnight at 4°C. The membranes were then incubated with an horseradish peroxidase-conjugated secondary antibody for 1 hour at room temperature. Detection was performed using the enhanced chemiluminescence plus Western Blot Detection System (ATTO Corporation, Tokyo, Japan) on X-ray film. The relative protein abundance normalized to β-actin was determined by quantitative densitometry (Sigma-Aldrich).
IHC analysis
Mouse lung formalin-fixed paraffin-embedded sections were subjected to H&E and IHC staining. Calprotectin levels in the mouse lung following A. fumigatus sensitization and challenge were assessed by IHC using an anti-calprotectin antibody.
Patients
All patients had a clinical diagnosis of asthma from the Bucheon Hospital of Soonchunhyang University, which was a clinical diagnosis of asthma according to Global Initiative for Asthma guidelines.18 The biospecimens and clinical data were provided by the biobank of Soonchunhyang University Bucheon Hospital, which is a member of the Korea Biobank Network. Blood sampling for calprotectin was collected at diagnosis before the administration of asthma medications and exacerbation state.17
The clinical characteristics of patients and healthy individuals are presented in Table 1.
Table 1
Clinical characteristics in control subjects and patients with asthma
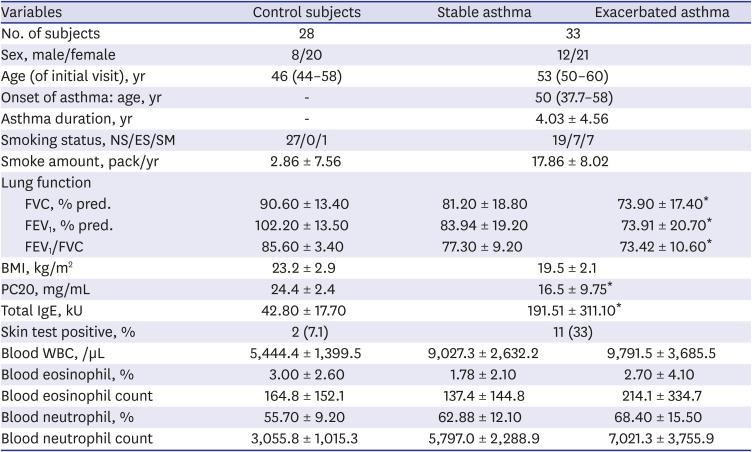
Data expressed as mean ± standard deviation, median (interquartile range) or number (%).
BMI = body mass index, ES = ex-smoker, FEV1 = forced expiratory volume in one second, FVC = forced vital capacity, NS = non-smoker, SM = smoker, % pred. = % predicted, PC20 = the concentration of methacholine required to decrease the forced expiratory volume in one second by 20%, IgE = immunoglobulin E, WBC = white blood cell.
*P < 0.01 compared with control subjects.
Enzyme-linked immunosorbent assays (ELISAs)
Calprotectin levels in serum samples from patients with asthma were determined by ELISA (Hycult Biotech, Wayne, PA, USA). The serum was incubated at room temperature in the ELISA plate followed by the addition of the tracer antibody and a streptavidin-peroxidase-conjugated secondary antibody. TMB solution and stop solution were added, and optical absorbance at 450 nm was read on a microplate reader. The minimum detection limit was set to 1.6 ng/mL for calprotectin according to the manufacturer's recommendations.
Ethics statement
The procedures used and the care of animals were approved by the Institutional Animal Care and Use Committee in Soonchunhyang University (approval No. 2015-06). This study was approved by the Institutional Review Board of Soonchunhyang University Hospital (approval No. SCHBC 2017-12-013-003).
RESULTS
A. fumigatus sensitization/challenge induced airway hyperresponsiveness (AHR) in mice
A. fumigatus-sensitized/challenged mice had higher AHR and numbers of inflammatory cells in BALF compared with control mice (Fig. 1).
Increased airway inflammation and goblet cell hyperplasia in the lungs of A. fumigatus-sensitized/challenged mice
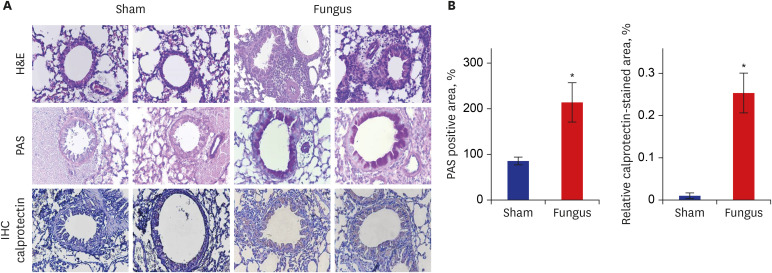
Histological examination revealed that the lungs of A. fumigatus-sensitized/challenged mice had numerous focal areas with inflammatory cell infiltrates, as well as peribronchial and intraluminal areas of exudation (Fig. 2A). Moreover, PAS staining showed that A. fumigatus sensitization/challenge resulted in mucosal gland hyperplasia (Fig. 2).
Fig. 2
H&E staining, PAS and IHC staining of mouse lung paraffin sections. (A) Top panel: H&E-stained lung tissue contained more inflammatory cell infiltrations in Aspergillus fumigatus-sensitization/challenge mice than control mice. Middle panel: PAS-stained airways contained increased goblet cells in the A. fumigatus-sensitization/challenge mice. Lower panel: IHC-stained lung tissue contained increased calprotectin in A. fumigatus sensitization/challenge mice. (B) The quantitation of goblet cells counts in mouse lung. (C) The quantitation of calprotectin in mouse lung.
H&E = hematoxylin and eosin, PAS = periodic acid-Schiff, IHC = immunohistochemical.
*P < 0.05, Fungus vs. Sham.
Elevated calprotectin expression in the lungs of A. fumigatus-sensitized/challenged mice
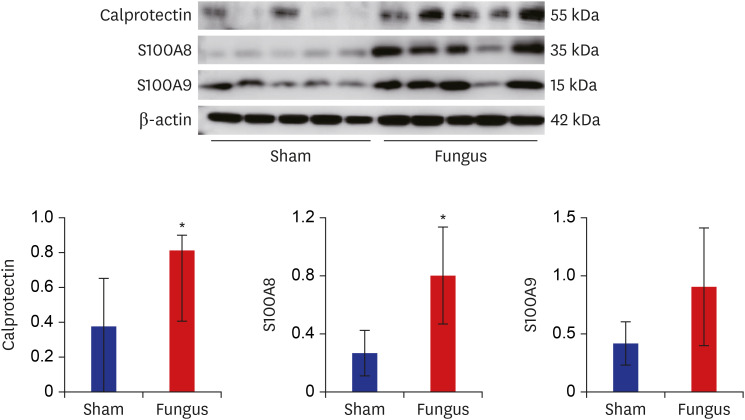
IHC staining demonstrated that the levels of calprotectin were increased in the lungs of A. fumigatus-sensitized/challenged mice compared with control mice (Fig. 2). Additionally, western blotting using protein lysates from the lungs of mice showed that A. fumigatus sensitization/challenge resulted in increased calprotectin, S100A8, and S100A9 protein levels (Fig. 3).
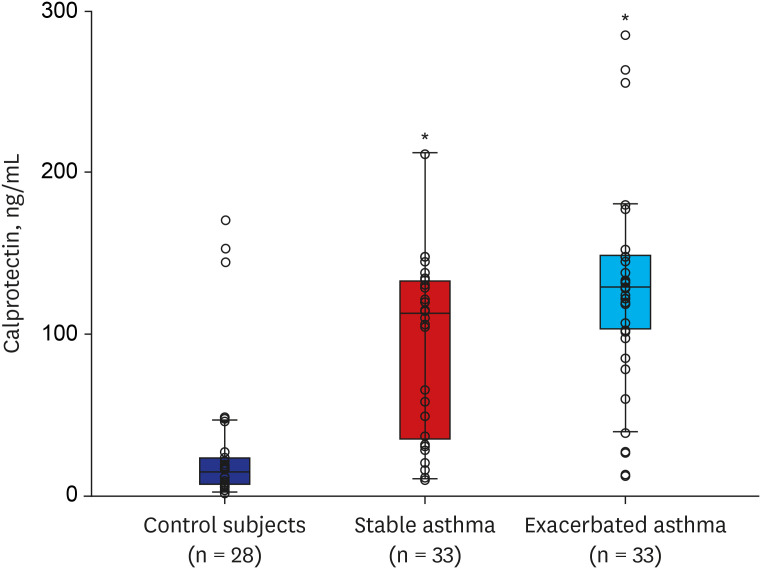
Increased calprotectin levels in the serum of patients with asthma
Thirty-three patients with asthma (mean age, 53 years) and 28 healthy individuals (mean age, 46 years) were recruited, the clinical characteristics of whom are shown in Table 1. The initial percent-predicted forced expiratory volume in one second (FEV1) and forced vital capacity (FVC), as well as the FEV1/FVC ratio, were lower in patients with asthma compared with healthy individuals. Total immunoglobulin E (IgE) and eosinophil blood count were also higher in patients with asthma, while body mass index (BMI) did not differ significantly between the two groups. The duration of asthma was 4.03 ± 4.56 years. Percent-predicted FEV1, percent-predicted FVC, and FEV1/FVC were lower in patients with asthma exacerbations compared with patients with stable asthma, while neutrophil blood count was higher. The serum levels of calprotectin were higher in patients with asthma compared with healthy individuals (Fig. 4).
Calprotectin levels were associated with the clinicopathological characteristics of patients with asthma
Calprotectin levels significantly associated with FEV1/FVC (r = −0.215, P = 0.043), smoking (r = 0.413, P = 0.017), BMI (r = −0.445, P = 0.000), and blood neutrophil proportion (r = 0.300, P = 0.004), and Log PC20 (r = −0.385, P = 0.011) in patients with asthma. Moreover, S100A8, S100A9, and calprotectin expression was increased in human bronchial epithelial cells and mice lungs (Fig. 5).
Fig. 5
Relationship of calprotectin with WBC, smoke amount, neutrophil proportion, BMI, FEV1%pred. FEV1/FVC, and Log PC20.
WBC = white blood cell, BMI = body mass index, FEV1 = forced expiratory volume in one second, FVC = forced vital capacity, %pred. = % predicted, PC20 = the concentration of methacholine required to decrease the forced expiratory volume in one second by 20%.

DISCUSSION
In this study, calprotectin levels were increased in serum from patients with asthma, and correlated with lung function, smoking amount, and blood neutrophil proportion in patients with asthma, suggesting that calprotectin could potentially be used as a biomarker for asthma.
Asthma is known to cause eosinophilic inflammation as well as IgE-mediated mast cell activation. Therefore the inhibition of airway inflammation by inhaled corticosteroids is the cornerstone of asthma therapy.19 However some patients with severe asthma demonstrated airway neutrophilia despite inhaled corticosteroid treatment.2021 Those patients respond poorly to corticosteroid treatment.22
The increase in neutrophil counts in the sputum of adults with asthma20 and in that of children with acute asthma exacerbations was reported.23 However there is controversy whether solely the presence of eosinophils or neutrophils can be used as a binary disease classifier as there may be overlap between these two phenotypes.
Calprotectin, the heterodimeric protein complex composed of S100A8 and S100A9, is a major calcium-and zinc-binding protein in the cytosol of neutrophils, monocytes, and keratinocytes.24
S100A8 and S100A9 have been associated with cancer metastasis, but also with various severe inflammatory diseases, including psoriasis, atopic dermatitis, atherosclerosis, neurodegenerative diseases, and diabetes.25 Extracellular S100A8 and S100A9 can induce the production and secretion of several inflammatory cytokines and chemokines.26272829303132 S100A8 and S100A9 are used as a biomarker and predictive indicator of therapeutic responsiveness in various inflammatory diseases.6 Calprotectin is primarily found in the cytosol of neutrophils, and is released upon neutrophil activation, resulting in elevated calprotectin serum levels in patients with inflammatory bowel disease, cystic fibrosis, rheumatoid arthritis, and other conditions associated with local neutrophilic inflammation.3334353637
There are a few studies that assess S100A8 and S100A9 from serum of asthmatic patients. S100A8 and S100A9 are involved in innate immune responses under the regulation of TLR4 polymorphisms in baker's asthma pathogenesis, suggesting that serum S100A8 could be a potential biomarker for predicting occupational exposure to wheat flour in bakery workers.38
High levels of fecal calprotectin have been reported in respiratory exacerbation, which may reflect a systemic exacerbation rather than solely lung. Antibiotic treatment has been shown to decrease fecal calprotectin levels, possibly due to its effects on the intestinal microbiome.16 Interestingly, a recent study has shown that interstitial lung disease is independently associated with increased fecal calprotectin levels in systemic sclerosis.39 In this study, serum calprotectin levels were higher in the serum of patients with asthma compared with healthy individuals and correlated with lung function and AHR, suggesting that calprotectin could be a useful biomarker for asthma.
Cigarette smoking and asthma interact to induce important adverse effects on clinical, prognostic and therapeutic outcomes. Prevalence rates for smoking in asthma are relatively close to those found in the general population.40 Smokers with asthma experience worse asthma control than nonsmokers with asthma.40 Mechanisms for the adverse effects of smoking in asthma include altered airway inflammation and corticosteroid insensitivity. Smoking worsens asthma symptoms and morbidity and promotes neutrophilic asthma.40 Cigarette smoke in asthmatic individuals also increased their sputum interleukin-8 levels in parallel to increased neutrophil percentages.41 In our study calprotectin levels correlated with smoke amount and blood neutrophil percentage in patients with asthma, suggesting that smoking increases neutrophil proportion in blood leading to calprotectin secretion. Further studies are needed to provide a more specific approach in patients with asthma with neutrophilic airway inflammation and to help in modulating the use of available conventional therapies.
Obesity42 also alters lung mechanics in asthmatics, but the impact is different for children and adults, likely due to the differential effect of obesity on the central and peripheral airway. In this study, BMI negatively correlated with calprotectin levels in contrast to lung function and AHR, suggesting that the impact of calprotectin is different for BMI and lung function.
There are limitations to this study. The most significant limitation would be the small sample size of patients with asthma. We did not select the pattern of airway inflammatory cells from sputum, and we observed calprotectin levels between stable and exacerbated state, not therapeutic response. Further studies should be considered for this point.
In conclusion, calprotectin levels were increased in the serum of patients with asthma, and correlated with lung function and AHR, smoke amount, and blood neutrophil percentage in patients with asthma. Calprotectin, S100A8, and S100A9 expression was elevated in human bronchial epithelial cells and mice lungs. Our data suggest that calprotectin could potentially be used as a biomarker for asthma.
 XML Download
XML Download