

 PDF
PDF Citation
Citation Print
Print



Introduction
Aortic dissection (AD) is one of the most catastrophic diseases and is associated with high morbidity and mortality.123 Several epidemiological studies investigating nationwide populations have shown that the incidence rate of AD was 2.5–10.0 per 100,000 person-years and has increased over time.14567 While multicenter studies mainly based on the population of North American or European countries have been consistently published,3891011 cohort studies based on the population of a single country are relatively rare,124 and studies conducted in Asian countries are even rarer.12 Moreover, previous publications from North America and Europe have some limitations regarding the accurate classification of the types of AD and identifying trends in the treatment and mortality rates on a nationwide scale.124 The national healthcare system in Korea is a single-payer system and has the advantage that most of the Korean population is obligatorily registered in the national medical insurance system. Thus, it is possible to conduct a cohort study on a nationwide scale and collect specific medical data based on certain diagnostic and unmissed interventional codes. Therefore, we aimed to analyze the annual trends in the incidence and mortality rates of thoracic AD classified into subgroups by treatment modalities based on the national Korea claims database.
METHODS
Data sources
We used the health claims data of the National Health Insurance Service (NHIS) in Korea (NHIS-2019-1-260). The NHIS is a nationwide health insurance service that covers 97% of the 50 million people in Korea, and its database contains demographic information, diagnoses, endovascular or surgical interventions, and death records. The International Classification of Diseases, Tenth Revision (ICD-10) codes were used to identify the diagnoses. To protect personal information, all personally identifiable information was removed from the NHIS database, and an anonymous code was used for each patient.
Study design and patient selection
We conducted a population-based retrospective cohort study. The data of AD patients have been available since January 2002. From January 2005 to December 2016, adult patients (≥ 18 years old) who received a diagnosis of thoracic or thoracoabdominal AD (ICD-10: I710) were included. The date of the first admission with an AD diagnosis was defined as the index date. Because the first hospitalization was included in our study, 619 patients who died in the emergency room or during transfer to a different hospital were excluded. Patients who had a history of visiting a hospital for AD between January 2002 and the index date were excluded. To validate the diagnostic code, we reviewed the medical records of 113 patients who were first admitted with the I710 code at one tertiary center (Hanyang University Seoul Hospital) from January 2011 to July 2019. The results showed a positive predictive value of 98.23% (111/113).
Following a previously reported study,2 we classified the AD patients into the following four cohorts in accordance with the procedure codes: type A surgical repair (TASR), type B surgical repair (TBSR), thoracic endovascular aortic repair (TEVAR), and medical management (MM). A patient with TASR was defined as a patient admitted with an AD diagnosis and coded for surgery of the ascending aorta (O2031) or aortic arch (O2032). A patient with TBSR was defined as a hospitalized AD patient coded for surgery of the descending aorta (O2033). A patient with TEVAR was defined as a patient admitted with an AD diagnosis and coded for TEVAR (M6611). The patients who met the criteria for both TEVAR and TASR or TBSR were classified as TEVAR only if the procedure code for TEVAR preceded the codes for TASR or TBSR; otherwise, these patients were classified as TASR or TBSR. MM was defined as the remaining AD patients who did not undergo any surgery and were not coded for TASR, TBSR, or TEVAR.
Patient demographics
The comorbidities of the AD patients were investigated using diagnostic codes obtained from the database during the three years prior to the index date. Hypertension, diabetes mellitus, chronic kidney disease, acute myocardial infarction, peripheral vascular disease, stroke, chronic obstructive pulmonary disease (COPD), connective tissue disorder, and congestive heart failure were included as comorbidities. The diagnostic codes used to investigate the comorbidities are shown in Supplementary Table 1.
Outcomes
The outcomes of this study were the incidence and mortality rates of AD. The annual and overall incidence rates of AD during the period from 2005 to 2016 were obtained. The annual incidence rate was calculated by dividing the number of newly developed AD patients by the mid-year population (on July 1) (≥ 18 years old) each year. To calculate the overall incidence rate, the median of the mid-year population during the study period was used. The population was collected from the Korea Statistical Information Service (http://kosis.kr, accessed August 8, 2019).
The annual mortality rates based on the year of the index date and the total mortality rate based on the overall period were determined. In-hospital mortality was indicated when the death date was prior to the end date of hospitalization. Follow-up ended in December 2018 or on the date of a patient's death, whichever occurred first. The number of incident cases was the denominator, the number of patients who died was the numerator, and the proportions of in-hospital, 30-day, 1-year, and 3-year mortality were determined.
Statistical analysis
The categorical variables are presented as numbers and proportions. All continuous variables were found to be non-normally distributed by the Anderson–Darling test and are expressed as the medians with interquartile ranges (IQRs). The incidence rate per 100,000 was determined, and the 95% confidence interval (CI) was calculated based on the Poisson distribution.13 The mortality rate per 100 people was obtained, and the 95% CI was calculated using the normal approximation of a binomial distribution with Yates' continuity correction. A linear regression analysis was used to calculate the p-value to identify the trends in the incidence and mortality rates. The annual percent change (APC) during the study period was calculated to measure the trends in the incidence and mortality rates. The APC was calculated using the following equation:

A chi-square test was applied to the categorical variables to compare the monthly and seasonal numbers of AD patients.
Age, sex, and comorbidities were identified as factors associated with in-hospital mortality among the AD patients. A stepwise-selected multivariable logistic regression analysis was used to calculate the odds ratio (OR) and 95% CI of in-hospital mortality. A minimum of 10 outcome events per predictor variable (EPV) is widely used as a lower limit for developing predictive models that predict binary outcomes.14 Following this rule, we performed a multivariable logistic regression analysis but omitted the variables with an EPV less than 10. All statistical analyses were conducted using SAS version 9.4 software (SAS Institute, Cary, NC, USA) and R 3.5.2 software (http://www.R-project.org). Statistical significance was determined using two-sided tests with significance indicated by a P value less than 0.05.
Results
Characteristics of the study population
In total, 20,900 patients (≥ 18 years) were admitted for the first time with an AD diagnosis in Korea from January 2005 to December 2016. Among these patients, 2,335 patients who visited a hospital for AD between January 2002 and the index date were excluded (Fig. 1). In total, 18,565 admissions for AD were finally included in this study (TASR, n = 4,319 [23.3%]; TBSR, n = 186 [1.0%]; TEVAR, n = 697 [3.8%]; MM, n = 13,363 [72.0%]). The baseline characteristics of the study population are presented in Table 1. The median age was 67.0 years (IQR, 54.0–76.0). The cohort of AD patients was predominantly male (54.3%). Hypertension (63.5%) and diabetes mellitus (23.9%) were the most common comorbidities. The median length of hospitalization was 10.0 (IQR, 4.0–18.0) days. Of a total of 18,565 patients, 15,584 patients were treated at the first hospital where they received their diagnosis, and 2,981 patients were treated at another hospital to which they were transferred. Among these patients, 2,870 patients were transferred once within one day from the index date, and 111 patients were transferred more than once.
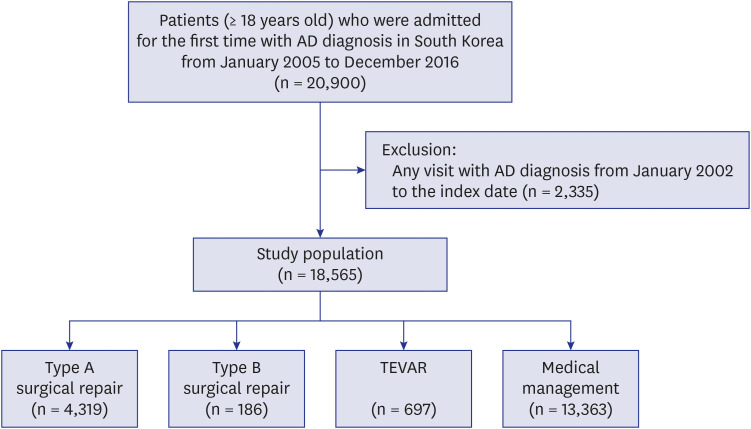
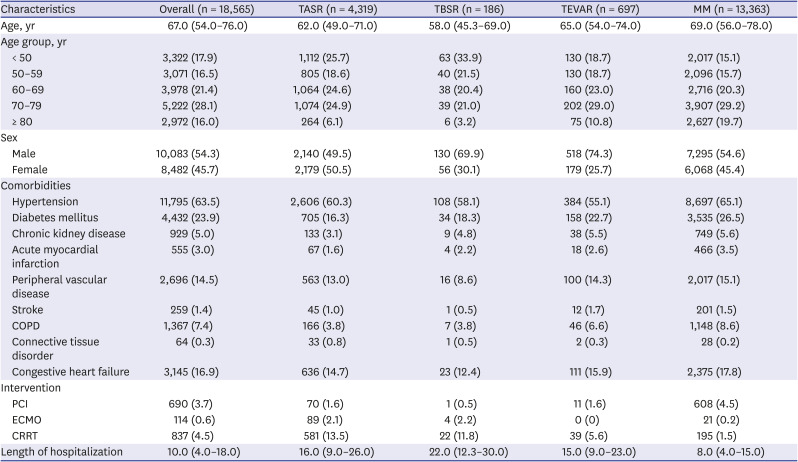
Fig. 1
Flow diagram of the cohort.
AD = aortic dissection, TEVAR = thoracic endovascular aortic repair.
![]()
Table 1
Characteristics of the patients diagnosed with thoracic aortic dissection in Korea (2005–2016)
Data are presented as median (interquartile range) or number (%).
TASR = type A surgical repair, TBSR = type B surgical repair, TEVAR = thoracic endovascular aortic repair, MM = medical management, COPD = chronic obstructive pulmonary disease, PCI = percutaneous coronary intervention, ECMO = extracorporeal membrane oxygenation, CRRT = continuous renal replacement therapy.
![]()
Incidence of AD
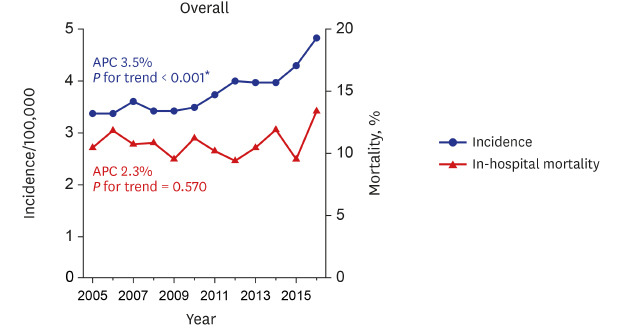
The overall incidence rate of AD during the study period (2005–2016) was 3.76 per 100,000 person-years (95% CI, 3.71–3.81). The frequencies and incidence rates are presented in Table 2. The incidence rate of AD has significantly increased from 2005 to 2016 (3.29 to 4.82 per 100,000 person-years; P for trend < 0.001), and the APC was 3.5%. In particular, the incidence rates of TASR (0.50 to 1.30 per 100,000 person-years; APC 9.1%; P for trend < 0.001) and TEVAR (0.02 to 0.26 per 100,000 person-years; APC 26.3%; P for trend < 0.001) significantly increased during the study period (Fig. 2). The monthly and seasonal incidence rates are presented in Fig. 3. According to the seasonal trend, the number of patients was the highest in the winter and lowest in the summer (P < 0.001).
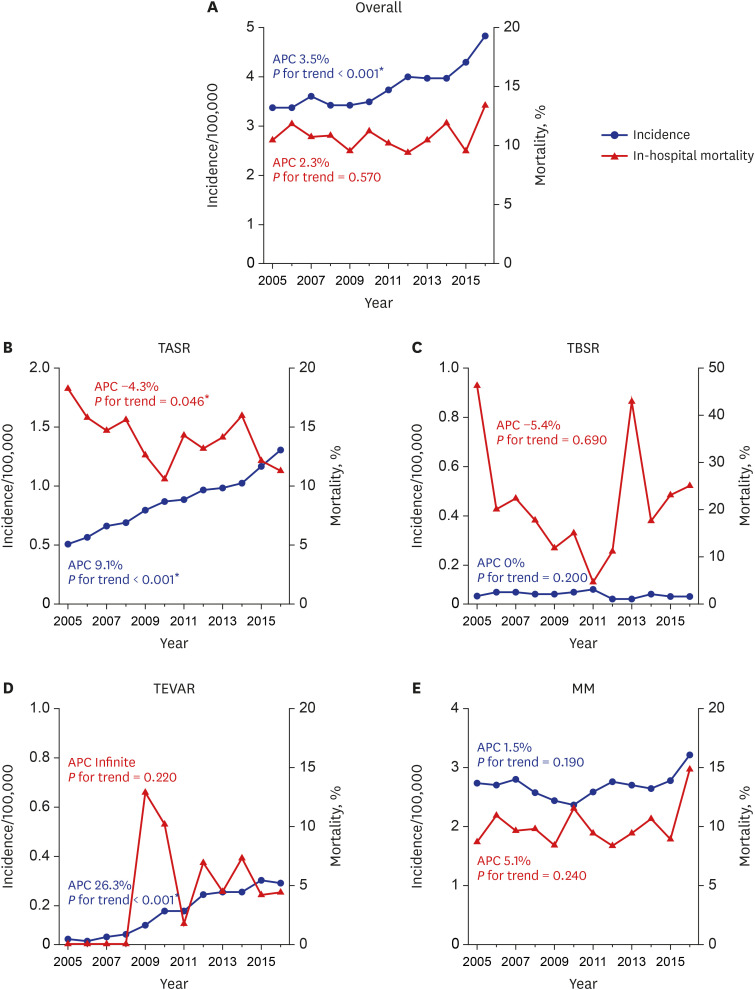
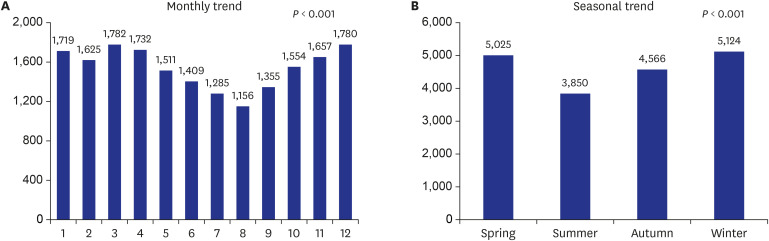
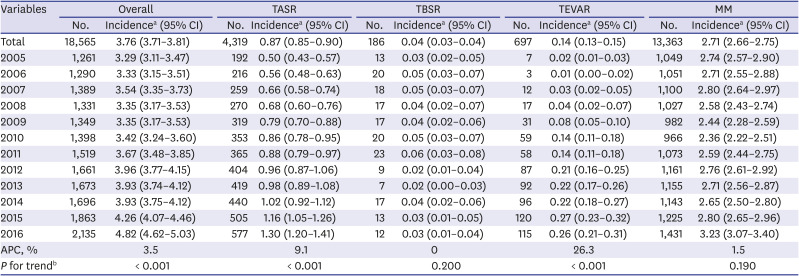
Fig. 2
Incidence and in-hospital mortality rates of thoracic aortic dissection patients in Korea from 2005 to 2016.
TASR = type A surgical repair, TBSR = type B surgical repair, TEVAR = thoracic endovascular aortic repair, MM = medical management, APC = annual percent change.
*Statistically significant (P value < 0.05).
![]()
Fig. 3
Monthly and seasonal numbers of AD patients from 2005 to 2016. (A) Monthly trend in the number of AD patients. (B) Seasonal trend in the number of AD patients.
AD = aortic dissection.
![]()
Table 2
Frequencies and incidence rates of thoracic aortic dissection in Korea from 2005 to 2016
TASR = type A surgical repair, TBSR = type B surgical repair, TEVAR = thoracic endovascular aortic repair, MM = medical management, CI = confidence interval, APC = annual percent change.
aThe incidence rate is presented per 100,000 person-years; bThe P values of the trends were calculated by a linear regression analysis.
![]()
Clinical outcomes
The in-hospital mortality rate in the patients with AD is presented in Table 3. The in-hospital mortality of AD was 10.84% (95% CI, 10.40–11.30) among all patients and 13.57% (95% CI, 12.57–14.63) among those in the TASR group. The TBSR group had the highest overall in-hospital mortality rate of 19.35% (95% CI, 14.09–25.92). During the study period, in-hospital mortality in the TASR subgroup significantly decreased from 18.23% in 2005 to 11.27% in 2016 (APC −4.3%; P for trend = 0.046) despite the consistency of the overall AD mortality rate of all patients (Fig. 2). The treatment outcome of TASR according to the hospital volume is also shown in Fig. 4. Surgical treatment for type A AD was conducted at 84 centers during the study period in our country. Among these treatments, operations for type A AD were performed in 10 centers with an average of 20 or more per year. Nine of these 10 centers had a survival rate to hospital discharge exceeding 88%. The 30-day mortality rate of TASR showed a decreasing tendency from 19.27% in 2005 to 11.96% in 2016, but the difference was not significant (APC −4.2%; P for trend = 0.091) (Supplementary Table 2).
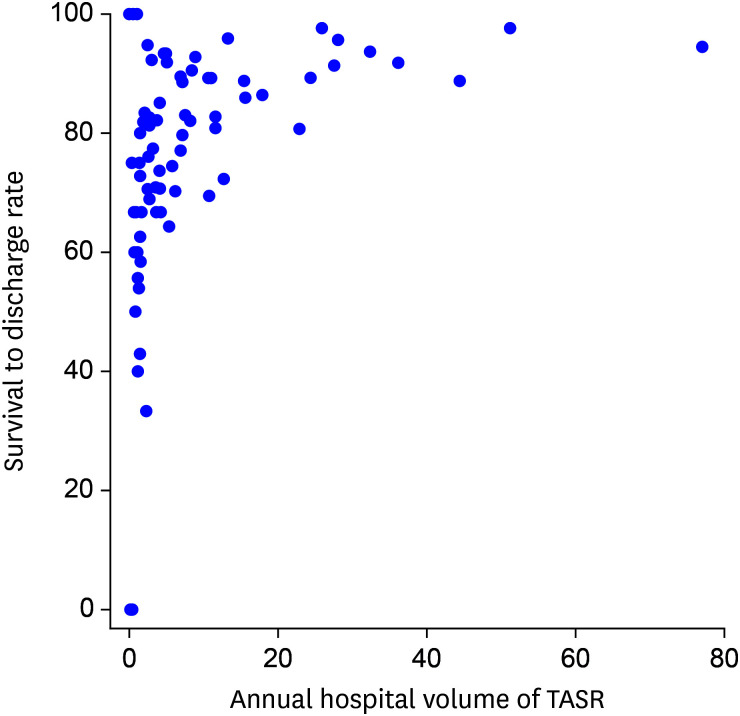
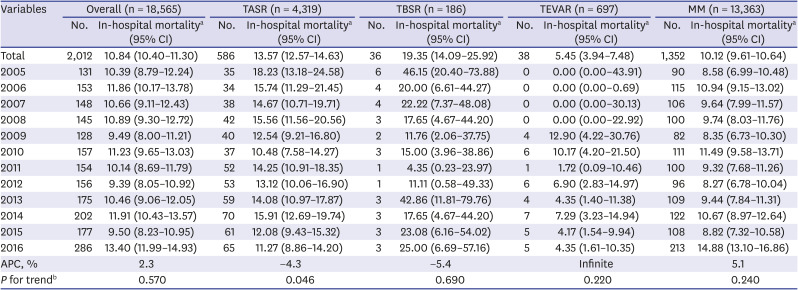
Fig. 4
Survival to discharge rate of surgical treatment for type A aortic dissection according to the hospital volume.
TASR = type A surgical repair.
![]()
Table 3
In-hospital mortality of the patients with thoracic aortic dissection in Korea from 2005 to 2016
TASR = type A surgical repair, TBSR = type B surgical repair, TEVAR = thoracic endovascular aortic repair, MM = medical management, CI = confidence interval, APC = annual percent change.
aThe in-hospital mortality is presented as % (95% CI); bThe P values of the trends were calculated by a linear regression analysis.
![]()
The one- and three-year mortality rates are also presented in Supplementary Table 2. The one-year TASR mortality rate showed a nonsignificant decreasing tendency from 24.48% in 2005 to 18.02% in 2016 (APC −2.7%; P for trend = 0.053). The three-year mortality rate of the whole cohort was 29.18% (95% CI, 28.53–29.84).
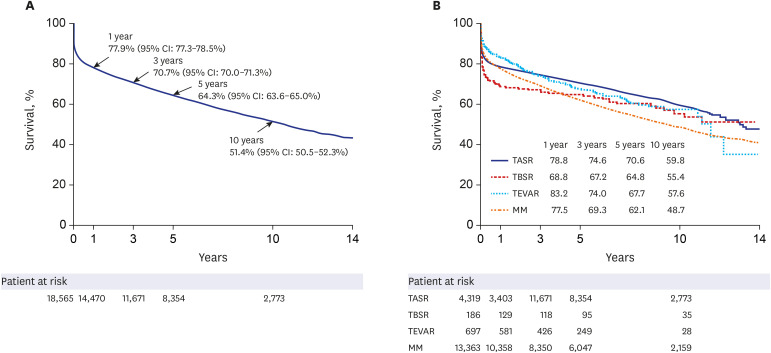
The 5-year and 10-year survival rates of all AD patients were 64.27% (95% CI, 63.56-64.99) and 51.37% (95% CI, 50.49–52.27), respectively (Fig. 5A). The 5-year and 10-year survival rates of the patients undergoing TASR were 70.63% (95% CI, 69.24–72.05) and 59.75% (95% CI, 57.88–61.69), respectively (Fig. 5B).
Multivariable analysis of risk factors
The independent risk factors for in-hospital mortality in the overall cohort and each subgroup were analyzed (Table 4). An older age was associated with higher in-hospital mortality among all patients and all subgroups. The female sex and hypertension were associated with higher in-hospital mortality among all patients and the MM subgroup. Chronic kidney disease was associated with higher in-hospital mortality among all patients and the TASR and MM subgroups.
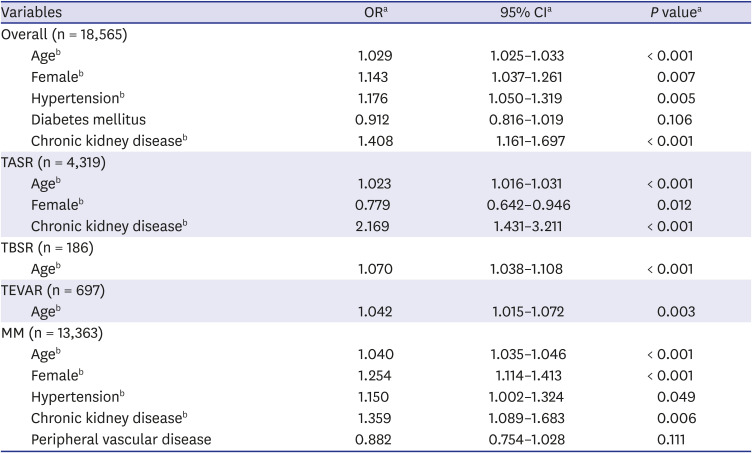
Table 4
Multivariable analysis of the factors associated with the in-hospital mortality rate of the patients with thoracic aortic dissection
OR = odds ratio, CI = confidence interval, TASR = type A surgical repair, TBSR = type B surgical repair, TEVAR = thoracic endovascular aortic repair, MM = medical management.
aORs, 95% CIs, and P values were calculated by a stepwise logistic regression analysis; bStatistically significant values (P < 0.05).
![]()
Discussion
AD is an acute condition with an extremely high morbidity rate, and quantifying its true incidence remains difficult. This study defined and classified the true incidence of thoracic AD using nationwide data from Korea. Among 18,565 patients who were newly diagnosed with AD from January 2005 to December 2016, the incidence rate of AD was 3.76 per 100,000 person-years. The annual incidence rate gradually increased during the study period. The overall in-hospital mortality rate was 10.84% and remained consistent during the study period, whereas the TASR in-hospital mortality rate significantly decreased. An older age, the female sex, hypertension, and chronic kidney disease were independent risk factors for in-hospital mortality.
This study, which involved a large retrospective population-based analysis of AD, is comparable to other previous contemporary studies.1245 In a rare previous Asian nationwide population-based study, Yeh et al.12 demonstrated that the annual incidence rate of AD was 5.6 per 100,000 person-years, and that the average annual incidence of patients treated surgically for type A AD was 1.44 per 100,000 person-years in Taiwan. Additionally, in a recent German multi-institutional retrospective study, Wundram et al.15 demonstrated that the emergency department incidence of acute type A AD was 5.24 per 100,000 person-years. However, this group only investigated the prevalence rate and did not address the treatment outcomes. Additionally, since the prevalence rate was calculated using the emergency department incidence rate as the denominator rather than the population-based incidence rate,15 it is believed that the number could be higher. In a recent study investigating the surgical outcomes of type A acute AD based on the Japan Cardiovascular Surgery Database, Abe and colleagues demonstrated that the annual incidence rate of surgery for acute type A AD was approximately 1.16 per 100,000 person-years.16 The incidence rates of overall AD and TASR in our study were 3.76 and 0.87 per 100,000 person-years, and these results revealed the lower incidence compared with that in studies in other countries.121516 In our study, all hospitalizations through the emergency room were included. However, we did not include patients who died in the emergency room or during transport to a different hospital because the date of the first admission with an AD diagnosis was defined as the index date. In total, 619 people were excluded during the study period, which could represent a limitation leading to an underestimation of the incidence rate. If included, the incidence rate was slightly higher at 3.89/100,000/year. However, since most patients with AD are hospitalized, we significantly confirmed the outcome by epidemiology and the treatment method by focusing on AD patients who were hospitalized.
In our results, the incidence rate of AD exhibited an increasing trend, and the APC was 3.5%. In particular, the incidence rates of TASR and TEVAR significantly increased over time in our study, which may be due to the development of the emergency transport system because living AD patients can be transferred to a hospital more rapidly.17 Additionally, the increase in the TEVAR group may be ascribed to the increasing trend in endovascular interventions.21819
In this study, the patients with thoracic AD were predominantly in their 60s and 70s. This distribution is similar to that reported in previous publications.124 In previous studies, the male-to-female ratio was approximately 2:1,124 however, the sex ratio in the current study was 54.3:45.7. This male-to-female ratio is comparable to that reported in a previously published study based on the Korean multi-center registry of acute aortic syndrome.20
Due to the limitations of the diagnostic coding system regarding the classification of types A and B, in this study, AD was classified into TASR, TBSR, TEVAR, and MM as described in a previously published study.2 McClure and colleagues stated that if a patient was alive at the time of discharge after medical treatment, the patient was classified as having type B AD. If a patient died during hospital admission, they assessed the records of the Office of the Registrar General – Death Database to identify the primary cause of death and classify the patient as having type A or B AD.1 However, in some cases, if a patient was diagnosed with acute retrograde type A AD with retrograde extension from an intimal tear in the descending aorta into the ascending aorta, he (or she) could survive and be alive at discharge with a favorable prognosis,21 and it is thought that there is a risk of misclassification.
According to our results, the in-hospital mortality rates of all patients and those in the TASR, TBSR, TEVAR and MM subgroups were 10.84%, 13.57%, 19.35%, 5.45% and 10.12%, respectively. These findings are comparable to the results reported in a previous study in which Zimmerman and colleagues demonstrated mortality trends in hospitalized AD patients in the general United States population (2003–2012).2
Despite the observed increasing trend in AD, the mortality rate did not increase, which is comparable to the findings of previous studies.2713 Our findings demonstrate that the in-hospital mortality rate in the TASR subgroup significantly decreased over time. This result is comparable to a recent study investigating the surgical outcomes of type A acute AD based on the Japan Cardiovascular Surgery Database. In this previous study, the overall operative mortality rate was 9.5% and showed a decreasing trend.16
We investigated the treatment outcome of TASR according to the hospital volume (Fig. 4), and nine of 10 centers with an average of 20 surgeries or more per year had a survival rate to hospital discharge exceeding 88%. This finding does not imply that the hospital volume and the outcome of TASR are directly proportional but rather suggests that a center with a volume of an average of 20 surgeries or more per year has acceptable outcomes.
Although the 30-day and 1-year mortality rates of the TASR subgroup did not significantly decrease, the overall trend was decreasing. Our findings suggest that advances in surgical skills, including standardized cannulation methods, neuroprotective techniques, a formalized series of main procedures, pre- and postoperative management and the establishment of a multidisciplinary team, may be major factors contributing to the improved outcomes.22
According to our results, the 30-day mortality rates of all patients and those in the TASR, TBSR, TEVAR and MM subgroups were 13.02%, 15.07%, 20.43%, 8.18% and 12.51%, respectively. In this study, the median length of hospitalization of all patients was 10.0 days, and the 30-day mortality rates of all patients and those in the TASR subgroup were higher than the in-hospital mortality rates. The median hospital stay in our study was longer than the hospitalization of 16 days in the International Registry of Acute Aortic Dissection study.3 Close observation of AD patients may be necessary after hospital discharge to improve early outcomes. In a recent study based on the nationwide Japanese Registry of All Cardiac and Vascular Disease database, Yamaguchi and colleagues demonstrated that the median hospital stay among patients who survived was 28 days in type A AD and 22 days in type B AD due to rehabilitation and nursing care during the same hospitalization period.2324
The 1-year survival rates of the TBSR and TEVAR subgroups were 68.8% and 83.2%, respectively. After a certain period, the survival rates of the TBSR and TEVAR subgroups became similar. The Kaplan-Meier curve of TEVAR is steeper than that of TBSR after the first year. Patients with type B AD undergoing surgical repair are at a high risk of morbidity and mortality during the acute phase because of catastrophic conditions, such as aortic rupture or impending rupture. Additionally, TEVAR carries a risk of the need for reintervention during long-term follow-up.1819
An older age was the most important factor predicting in-hospital mortality in all treatment groups, including the whole population. Obviously, age can affect treatment due to the patient’s general condition or underlying diseases. The female sex, hypertension and chronic kidney disease were other risk factors for in-hospital mortality.
Our study has several limitations. First, as mentioned above, it was impossible to stratify the study cohort into type A or B AD due to the limitations of the coding system. Therefore, the patients were classified into the TASR, TBSR, TEVAR and MM subgroups as previously described.2 Second, our database reflects the incidence of AD in hospitalized patients, and accurately defining the incidence of AD is difficult because of its high early mortality rate and the common problem of missed diagnoses due to death outside of the hospital or before arrival at the hospital.456 These limitations might lead to the underestimation of the incidence of AD. Autopsies of deceased patients suspected of having died from AD could help determine a more accurate incidence rate, but practical and ethical difficulties exist. Third, it is impossible to determine the exact date of surgical or endovascular intervention. If we know the date of the surgical or endovascular intervention, it may be possible to determine whether an emergency occurred; however, this analysis is impossible due to the nature of the nationwide health insurance claims from the NHIS.
In conclusion, the incidence rate of AD was 3.76 per 100,000 person-years, with an increasing tendency in Korea. The incidence rates of TASR and TEVAR significantly increased over time. The patients with thoracic AD were predominantly in their 60s and 70s. The male-to-female ratio was 54.3:45.7, which slightly differs from the sex ratios reported in previous studies. The in-hospital mortality rates of all patients and the TASR subgroup were 10.84% and 13.57%, respectively, which are noninferior to the outcomes reported in previous studies from other countries, and the in-hospital mortality rate in the TASR subgroup decreased over the course of the decade. An older age, the female sex, hypertension, and chronic kidney disease were significant predictive factors for in-hospital mortality.
 XML Download
XML Download