

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acute pyelonephritis (APN) is a urologic disease that is commonly encountered in emergency departments and results in a significant number of hospital admissions.1 The annual incidence rate of APN was reported as 15 to 17 cases per 10,000 individuals in the USA.2 A Korean study reported that the annual incidence rate of APN per 10,000 individuals has been increasing every year.3
The clinical symptoms of APN range from costovertebral tenderness, voiding difficulties, and fever to a life-threatening condition or even death.4 Uncomplicated APN is defined as APN that occurs in a normal genitourinary tract. On the other hand, complicated APN is defined as APN accompanied by infections in patients with genitourinary tract abnormalities.5 The prognosis of complicated APN is considerably worse than that of uncomplicated APN, with mortality rates of 6% to 10%. Therefore, APN with obstructive uropathy usually requires emergency drainage of the upper urinary tract with percutaneous nephrostomy (PCN) or retrograde double J stenting.6 Risk factors associated with high-mortality in patients with complicated APN include immunosuppression, advanced age, healthcare-associated infection, obstructive uropathy, thrombocytopenia, serum albumin level, high C-reactive protein (CRP) levels, and bacteremia.789
Sepsis is defined as a systemic inflammatory response syndrome in the presence of suspected infection.10 Moreover, sepsis is the strongest independent risk factor for septic shock and mortality in patients with APN.11 Septic shock is defined as a subset of sepsis, which is characterized by profound circulatory, cellular, and metabolic abnormalities and is associated with a greater risk of mortality than that with sepsis alone.12 Patients with septic shock commonly require vasopressor administration to maintain a mean arterial pressure of 65 mmHg or higher and a serum lactate level greater than 2 mmol/L in the absence of hypovolemia.12
Studies focusing on the risk factors associated with septic shock and complicated APN are rare. The aim of this study was to analyze the risk factors associated with sepsis and septic shock with cases of obstructive urolithiasis in our institution for 11 years.
METHODS
The medical records of patients who visited the Department of Urology, Kyung Hee University School of Medicine, from December 2006 to July 2017 for APN with obstructive urolithiasis were reviewed. APN was defined as the presence of more than 5 white blood cells/high-power field, an isolated bacterial count of more than 104 colony-forming units in the urine specimen, high-grade fever of more than 38°C, and other related symptoms.9 The patient's age, sex, underlying comorbidities (including diabetes mellitus, hypertension, ischemic heart disease, and stroke), history of urolithiasis and urinary tract infection (UTI), urinary stone size and location, and type of drainage were recorded. We also evaluated the results of blood and urine cultures before initiating antibiotic treatment. Laboratory examinations including blood leukocyte count, blood thrombocyte count at the nadir, CRP, serum creatinine, and total bilirubin level were performed prior to drainage.
Emergency drainage for the decompression of hydronephrosis was performed for severe cases (e.g., poor performance status, marked elevation in leukocyte count, and CRP level). Retrograde double J stenting or PCN was performed according to the urologist's preference. Retrograde double J stenting was performed under fluoroscopic guidance using a rigid cystoscope under local anesthesia. A 6-French polyurethane double J stent was used. PCN was performed after ultrasound-guided renal puncture under local anesthesia. Guidewire insertion, fascial dilation, and 7-French pigtail catheter placement were performed using fluoroscopy.
The diagnosis of sepsis was made according to the criteria for systemic inflammatory response syndrome, which included two or more of the following conditions: body temperature greater than 38°C or less than 36°C; heart rate greater than 90 beats per minute; tachypnea, presenting as a respiratory rate of greater than 20 breaths per minute or hyperventilation, as indicated by a partial CO2 pressure of less than 32 mmHg; and a leukocyte cell count greater than 12,000/mm3 or less than 4,000/mm3, or immature neutrophils greater than 10%.1314 Septic shock was defined as sepsis with a systolic blood pressure of less than 90 mmHg despite adequate fluid replacement or vasopressor administration for at least 1 hour.1516 We identified risk factors for septic shock by comparing patients whose condition did or did not progress to septic shock.
Data were analyzed using SPSS, version 18.0 (IBM Co., Armonk, NY, USA). Proportion comparisons for categorical variables were performed using χ2 tests. The P value and relative ratio were calculated for risk factors. P values < 0.05 were considered statistically significant. Moreover, multivariate model analysis was performed to determine the progression of complicated APN to sepsis and septic shock.
RESULTS
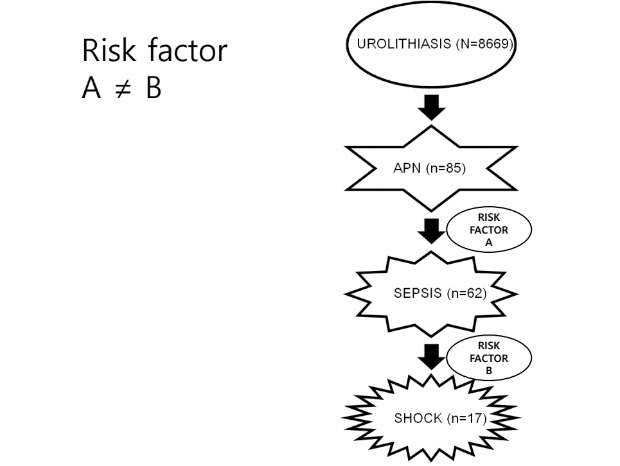
A total of 85 patients were treated for complicated APN associated with ureteral stone at our department during the 11-year period. The median age was 56.9 years and 65 (76.5%) events occurred in women. Thirty-two (37.6%) patients had a previous history of stone or UTI. All patients required hospitalization except for those who refused treatment. At initial diagnosis, 62 (72.9%) patients met the criteria for sepsis and 17 (27.4%) patients from among them had septic shock. Forty urine (47.1%) and twenty-five (29.4%) blood culture samples showed positive results on routine examination. Consistently, the most common pathogen was Escherichia coli, and Proteus mirabilis was the second most common cause. Furthermore, the incidence of ESBL(−) E.coli was dominant than that of ESBL(+) E.coli in each group. There was no significant difference among them.
Tables 1 and 2 summarize the clinical characteristics of the patients who were divided based on the presence of sepsis and septic shock. Patients who experienced sepsis exhibited a greater tendency of having a history of genitourinary stones (35.5% vs. 8.7%; P = 0.015), higher leukocyte count (1.30 × 103/µL vs. 0.86 × 103/µL; P < 0.001), higher CRP levels (9.14 mg/dL vs. 4.53 mg/dL; P = 0.006) and lower albumin levels (3.99 g/dL vs. 4.12 g/dL; P = 0.038). Urologists preferred PCN (56.5% vs. 30.4%; P = 0.033) over ureteral stenting in septic conditions.
Table 1
Baseline comparative data of patients with complicated acute pyelonephritis depending on the presence of sepsis
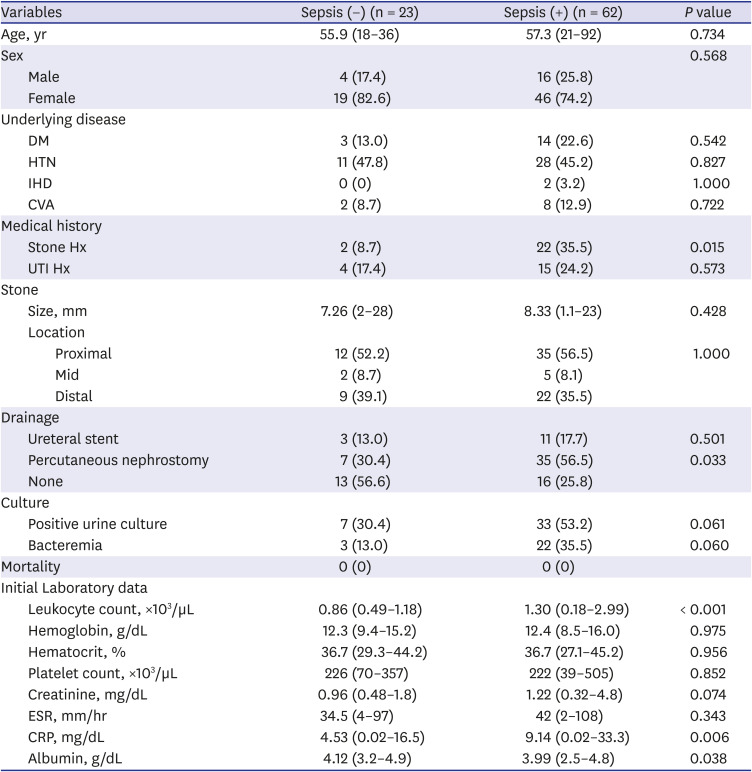
Table 2
Subgroup analysis of sepsis in patients with complicated acute pyelonephritis according to the presence of septic shock
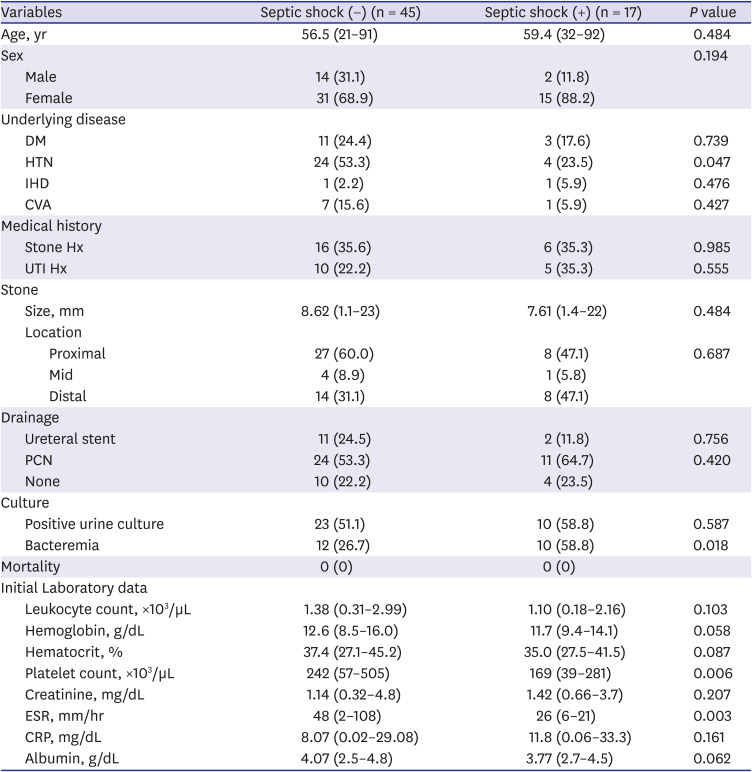
Data are presented as median (interquartile range) or number (%).
DM = diabetes mellitus, HTN = hypertension, IHD = ischemic heart disease, CVA = cerebrovascular accident, Hx = history, UTI = urinary tract infection, PCN = percutaneous nephrostomy, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein.
The incidence of positive blood culture (58.8% vs. 26.7%; P = 0.018), low platelet count (169 k/µL vs. 242 k/µL; P = 0.006) and high blood urea nitrogen (BUN) (23.2 mg/dL vs. 17.6 mg/dL; P = 0.016) were significantly higher in the septic shock than that in the non-septic shock group. In addition, a lower incidence of comorbid hypertension (23.5% vs. 53.3%; P = 0.047) and lower erythrocyte sedimentation rate (ESR) (26 vs. 48; P = 0.003) were observed in the septic shock group.
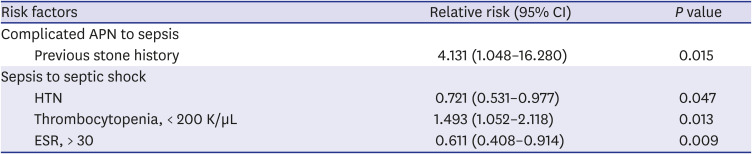
Previous history of genitourinary stone (relative risk [RR], 5.775; confidence interval [CI], 1.237–26.962; P = 0.015) and abnormal leukocyte count (< 4,000/mm3 or < 10,000/mm3; RR, 5.391; CI, 1.925–15.092; P = 0.001) were significant factors that indicated the presence of sepsis. On the other hand, thrombocytopenia (< 200 K/µL; RR, 4.350; CI, 1.299–14.569; P = 0.013), abnormal BUN (< 8 or > 20; RR, 3.825; CI, 1.170–12.510; P = 0.022) and positive blood culture (RR, 3.929; CI, 1.219–12.661; P = 0.018) were associated with more catastrophic conditions, i.e., septic shock. Underlying hypertension (RR, 0.269; CI, 0.076–0.953; P = 0.047) and high ESR (> 30; RR, 0.144; CI, 0.033–0.622; P = 0.009) had protective effects on the progression to septic shock (Table 3).
Table 3
The distinct indicators suggesting the progression of complicated APN to sepsis and septic shock
DISCUSSION
Urosepsis, which is defined as sepsis caused by urogenital tract infection, accounts for 20%–30% of all septic conditions.1718 Obstructive diseases of the upper urinary tract, such as urinary stones, stenosis or tumors, are the main cause of urosepsis.17 Older individuals, patients with diabetes, immunocompromised patients, transplant recipients, and patients with acquired immunodeficiency syndrome exhibit reduced host defense immunity. Moreover, local factors, such as urolithiasis, obstructive uropathy, congenital uropathy, neurogenic bladder disorders, and endoscopic procedure, can affect the severity of urosepsis. Lee et al.7 analyzed the risk factors associated with septic shock in patients with bacteremic APN who were admitted to the department of urology. The overall mortality rate was 6.7%, but the mortality rate of 54 patients who initially presented with shock was 25.9%. Multiple logistic regression analyses revealed that the presence of urinary tract obstruction (odds ratio [OR], 4.391), healthcare-associated infection (OR, 3.491), and liver cirrhosis (OR, 4.609) were independent risk factors responsible for the incidence of septic shock.
Obstructive uropathy of the upper urinary tract that is complicated with infection requires decompression of the renal collecting system with ureteral stenting or PCN. Rapid decompression procedures such as PCN or retrograde double J stent insertion reduce intrarenal pressure and improve renal perfusion. Borofsky et al.19 reported that 1,712 patients with ureteral calculi and sepsis were from the 2007 to 2009 Nationwide Inpatient Sample. Of the patients with urosepsis, 78% underwent surgical decompression. Mortality was higher in patients who were not treated with surgical decompression (19.2% vs. 8.82%). The lack of surgical decompression was independently associated with an increased OR of mortality even after adjusting for patient demographics, comorbidities, and geographic region of treatment (OR, 2.6). They concluded that the absence of surgical decompression was associated with higher odds of mortality in patients with sepsis and ureteral calculi.
The diagnosis of uroseptic shock is made when a patient with severe urosepsis presents with acute circulatory failure characterized by persistent arterial hypotension (systolic arterial pressure below 90 mmHg, mean arterial pressure < 60 mmHg, or reduction in systolic blood pressure > 40 mmHg compared to the baseline), despite adequate volume resuscitation.20
Several researchers have published studies that focused on determining the risk factors associated with uroseptic shock.9212223 Tambo et al.9 assessed the risk factors for septic shock with obstructive APN associated with upper urinary tract calculi. Multivariate analysis revealed that reduction in platelet count and serum albumin levels were independent risk factors for septic shock. Moreover, Kamei et al.22 reviewed the records of 48 patients who underwent emergency drainage of the upper urinary tract for sepsis associated with acute obstructive pyelonephritis. Multivariate logistic regression analysis identified that thrombocytopenia and positive blood culture were independent risk factors for septic shock. Platelets and neutrophils are involved in the pathogenesis of urosepsis and work in conjunction to contribute to the inflammatory response. Studies have demonstrated that platelets and neutrophils are recruited to the microvasculature of lung and liver, leading to the production of neutrophil extracellular traps in sepsis.23 Various factors can be responsible for low serum albumin levels, including increased protein catabolism and decreased hepatic synthesis, which can result in extravasation into the extravascular space because of increased vascular permeability during the inflammatory process. Bossink et al.24 reported that low serum albumin levels were one of the predictive factors for shock development (as per univariate analysis). Similar to the previous studies, our study showed that previous history of stones and abnormal leukocyte count were significant factors indicating the presence of sepsis. Moreover, thrombocytopenia, abnormal BUN levels, and positive blood culture were proven to be associated with urosepsis. Furthermore, we discovered that underlying hypertension and high ESR had protective effects on the progression to septic shock.
The present study has some limitations, despite these interesting findings. First, this was a retrospective study; therefore, some inflammatory markers such as procalcitonin, serum amyloid A, and cytokines were not investigated, and the collected data might have been missed, which could have affected the results of the study. Moreover, the treatment process was not the same for all patients. The timing of the examination and treatment, which could be related to the risk factors for uroseptic shock, such as urine culture, prescription of antibiotics, and timing or method of drainage, were not the same for all patients. Furthermore, the physician who first met the patient was responsible for the choice of empirical antibiotics. Finally, the sample size was small because this investigation was a single-center study was conducted with the patients from a single institution. Therefore, future multi-center studies are needed to validate the results of this study.
In conclusion, the risk factors associated with the progression from APN to sepsis differ from those associated with the progression from sepsis to septic shock. Several factors should be considered while selecting treatment options, depending on the severity of complicated APN with ureteral stone. The condition should be managed with aggressive treatment and close observation, especially in the presence of risk factors.
 XML Download
XML Download