

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Antiretroviral therapy (ART) has reduced the rates of morbidity and mortality among patients with human immunodeficiency virus (HIV) infection.12 In many regions, HIV infection is now widely considered as a manageable chronic disease, with the life expectancy of HIV patients receiving ART approaching that of the general population in some settings.34 Survival after the diagnosis of HIV has also continued to improve over time since highly active antiretroviral therapy (HAART) was introduced in Korea in 1991.5 Along with increased survival, the causes of death among HIV-infected patients have also changed gradually. As a result of the dramatic reduction in mortality resulting from acquired immunodeficiency syndrome (AIDS) defining illness, the proportion of non-AIDS-related death has increased in the HAART era.6 A recently published Canadian population-based cohort study showed that non-AIDS-defining cancers are currently the leading non-AIDS-related cause of death among HIV-infected patients. A previous study conducted in Korea showed that the proportion of AIDS-related death remained higher than non-AIDS-related death between 1990 and 2011. Since then, although an increase in survival has been documented, there have not been any recently published data regarding the specific causes of death among people diagnosed with HIV in Korea. According to a study forecasting cause-specific mortality in Korea, causes of death regarding HIV and AIDS are estimated to increase from 2002 to 2030.7 However, until now, little data has been available on the causes of death in HIV patients in Korea, which could be useful information to help focus on appropriate interventions to improve the rates of morbidity and mortality of HIV patients. In addition, with the ongoing national Korean multicenter cohort research data, there is a limitation to investigate the changes in the cause of death because 73.8% of the data on causes of death are missing.8
This study aimed to evaluate the changes in the causes of death among HIV-infected patients in Korea in the era of ART according to the HIV diagnosis and death period. In addition, we aimed to elucidate the prognosis of low CD4 counts at the time of HIV diagnosis.
METHODS
Study design and population
A retrospective hospital-based cohort study was conducted to assess the causes of death among HIV-infected patients, as well as the impact of HIV patients diagnosed with low CD4 count. Kyungpook National University Hospital is a 914-bed, university-affiliated teaching hospital and provides care for HIV patients in Korea. The hospital started to treat HIV patients in 1987. This study included patients who were diagnosed with HIV between July 1984 and October 2019 at Kyungpook National University Hospital and who were 18 years old or older at the time of diagnosis were followed up through the end of October 2019. Medical records were reviewed for time of diagnosis, date of death, follow-up period, and disease causing the death. Furthermore, we reviewed the national health insurance status of HIV patients to determine the possible impact on their long-term prognosis of survival. Patients were classified according to a CD4 count less than 200 cells/mm3 or more than 200 cells/mm3 at the time of diagnosis. The survival analysis between CD4 count < 200 cells/mm3 and CD4 count ≥ 200 cells/mm3 groups were conducted to compare the effect of CD4 count on long-term mortality.
Definitions
A CD4 count less than 200 cells/mm3 was defined as the CD4 < 200 cells/mm3 group, and a CD4 count more than 200 cells/mm3 was defined as the CD4 ≥ 200 cells/mm3. The survival period was defined as the time of the first HIV diagnosis time to death. The Korean National Health Insurance is operated by the government and it covers the entire population residing within the territory of Korea except for beneficiaries of medical aid, approximately 98% of the Korean population of 48.4 million. The medical aid program (MAP) is a benefit program for the underprivileged for which eligibility is determined based on the patients' income level.9 Cause of death was defined as the main conditions that initiated the sequence of events resulting in death. Cause of death was determined by the medical records written by an infectious disease specialist who had taken care of the patient if the patient died in the study hospital. If the patient died outside of the study hospital, cause of death records were collected from the HIV/AIDS consultation center in the study hospital. The cause of death was investigated by 4 classification methods. Category 1 was classified as mainly infection and non-infection. Category 2 was classified as Pneumocystis pneumonia (PCP), tuberculosis (TB), other infections, malignancy, other non-infections, and cerebrovascular disease. Category 3 was classified as AIDS-related diseases, AIDS-non-related infection and others. Category 4 was classified as AIDS-related infection, AIDS-related malignancy, AIDS-non-related infection, AIDS-non-related malignancy, and others. Cause of death was categorized as an AIDS death if the stated cause was an AIDS-defining opportunistic infection or malignancy. AIDS-defining illness and clinical categories were defined by the 1993 Centers for Disease Control and Prevention classification criteria.10 Cause of death was classified as a non-AIDS death for patients who died of other conditions, which was further categorized into bacterial infection and sepsis, AIDS-non-related malignancy, cardiovascular disease, liver disease, pulmonary disease, gastrointestinal disease, hematological disease, or accidental cause, including injury and suicide. Other opportunistic diseases, including PCP, were diagnosed according to the criteria suggested by the Centers for Disease Control and Prevention.10 TB death includes definite, probable, or possible cases: definite if culture for Mycobacterium tuberculosis was positive, probable if clinical symptoms and signs consistent with TB were present and stain was positive for acid-fast bacilli or if there were histological findings consistent with TB, and possible if clinical and radiological signs consistent with TB were present and there was an improvement with standard anti-TB therapy. Hepatitis B virus infection was defined as positive hepatitis B virus surface antigen in the serum. Hepatitis C virus infection was defined as the presence of hepatitis C virus antibody with positive RNA in serum. Renal disease was defined as chronic kidney disease, either on hemodialysis or not. Heart disease was defined as arrhythmia, heart failure, or coronary heart disease. The World Health Organization (WHO) clinical staging system for HIV and AIDS was used for baseline assessment of patients.11
Statistical analysis
Descriptive statistics were used to characterize the cohort. Categorical variables were compared using Fisher's exact test, whereas non-categorical variables were tested with the Mann-Whitney U test. Kaplan–Meier and log rank tests for death were performed to compare survival between patients diagnosed with CD4 < 200 cells/mm3 and patients with CD4 ≥ 200 cells/mm3. We used the HIV diagnosis date as the time of entry and follow-up was censored on the death date. For cause-specific analyses, data were also censored at death data from any other cause. All tests were considered statistically significant at a P value of less than 0.05. The statistical analyses were performed using R statistics, version 4.0. (The R Foundation, https://www.r-project.org, Vienna, Austria).
RESULTS
Description of study population
Between July 1984 and May 2019, a total of 801 patients attended the study hospital. Among 801 HIV follow-up patients, there were 71 confirmed deaths at Kyungpook National University since 2000. Of these 71 HIV patients, 56 patients died at the study hospital and 15 others died outside of the hospital. Four patients who had unknown cause of death were excluded, leaving 67 patients to be included in the death cause analyses. Among the 801 patients, about 145 patients were confirmed to be lost to follow-up, and the cause of follow-up loss was being transferred to other hospitals or to their home countries for foreigners. The baseline characteristics of the 801 patients are shown in Table 1. Of the patients, 728 (90.9%) patients were male and 73 (9.1%) were female. The mean age at the time of HIV diagnosis was 36 years old. Six hundred and twenty-seven patients (78.3%) were supported by national health insurance and 174 (21.7%) were supported by MAP. By the end of 2019, 71 patients (8.9%) in the cohort had died and 730 patients (91.1%) remained alive (Table 1).
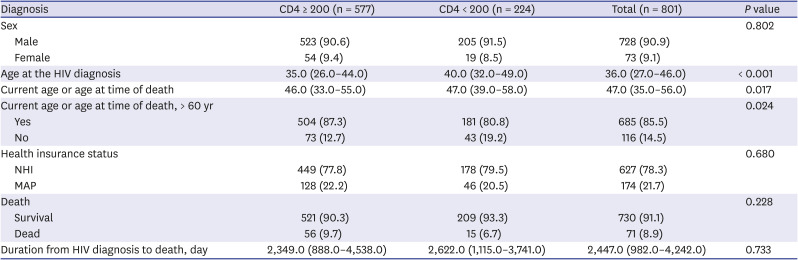
Table 1
Characteristics of 801 HIV patients according to CD4 count at the time of HIV diagnosis
Data are presented as number (%) or median (interquartile range).
HIV = human immunodeficiency virus, NHI = national health insurance, MAP = medical aid program.
![]()
These 801 patients were grouped according to their CD4 count when they were diagnosed. There were 224 patients in the CD4 < 200 cells/mm3 group and 577 patients in the CD4 ≥ 200 cells/mm3 group. There was no statistical significance in sex distribution or health insurance status between the 2 groups. The mean age at the time of diagnosis was significantly higher in the CD4 < 200 cells/mm3 group (35.0 vs. 40.0; P < 0.001). Current age or age at the time of death was also significantly higher in the CD4 < 200 cells/mm3 group (46.0 vs. 47.0; P = 0.017), whereas current age or death at 60 years or older showed lower in the CD4 < 200 cells/mm3 group (P = 0.024). Mortality was 6.7% in the CD4 < 200 cells/mm3 group and 9.7% in the CD4 ≥ 200 cells/mm3 group (P = 0.228). Median follow-up period from HIV diagnosis to death was 2,622 days in the CD4 < 200 cells/mm3 group and 2,349 days in the CD4 ≥ 200 cells/mm3 group (P = 0.733). No significant statistical difference was found between the 2 groups (Table 1). However, mortality rate (per 1,000 person-years) was 9.6 in the CD4 < 200 cells/mm3 group and 12.3 in the CD4 ≥ 200 cells/mm3 group.
Characteristics of HIV-infected patients who died according to CD4 < 200 cells/mm3 or CD4 ≥ 200 cells/mm3 at the time of HIV diagnosis showed no statistical difference in terms of sex distribution, age at the time of HIV diagnosis, age at the time of death, death at age 60 years or older, health insurance coverage status, place of death, stages of HIV infection at the time of HIV diagnosis and death, ART treatment history, or history of underlying diseases and AIDS-related diseases, except diagnosed year distribution (Supplementary Tables 1 and 2).
HIV patient prognosis based on CD4 count and health insurance status at the time of HIV diagnosis
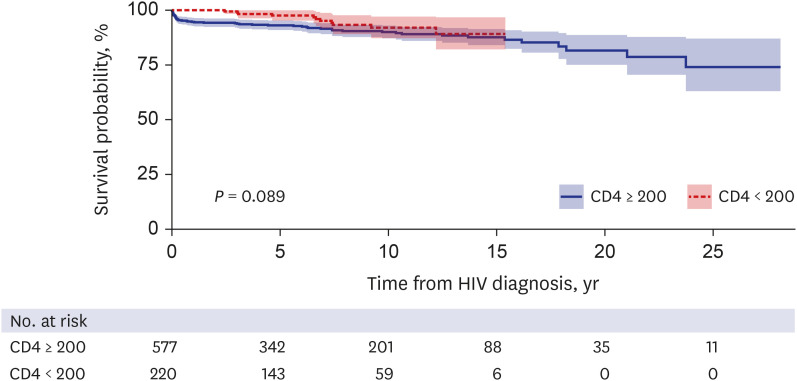
Kaplan–Meier survival analysis estimated changes in survival over time by diagnosis year CD4 count. The mortality of 71 patients, regardless of the cause of death, in the CD4 < 200 cells/mm3 group was not statistically different from the CD4 ≥ 200 cells/mm3 group (log-rank, P = 0.380) (Supplementary Fig. 1). Kaplan–Meier and log rank tests were analyzed for the 67 patients with confirmed cause of deaths and long-term survival rate analysis showed no statistical difference between the two groups (log rank, P = 0.089) (Fig. 1). However, the short-term survival rate (HIV diagnosis to death within three months) showed a higher survival rate in groups with CD4 counts less than 200 at the time of diagnosis (log-rank, P = 0.002).
Kaplan–Meier and log rank tests were conducted for the 71 death patients according to medical health care status. The mortality of the MAP group showed no statistical difference from the national health insurance group (log-rank, P = 0.054) (Supplementary Fig. 2).
Causes of death
When the causes of death were divided into infection and non-infection, as shown in category 1, 44 (65.7%) of the 67 deaths were confirmed to be the result of infection, whereas only approximately half of the total deaths (23 [32.4%]) were the result of non-infectious causes (Table 2).
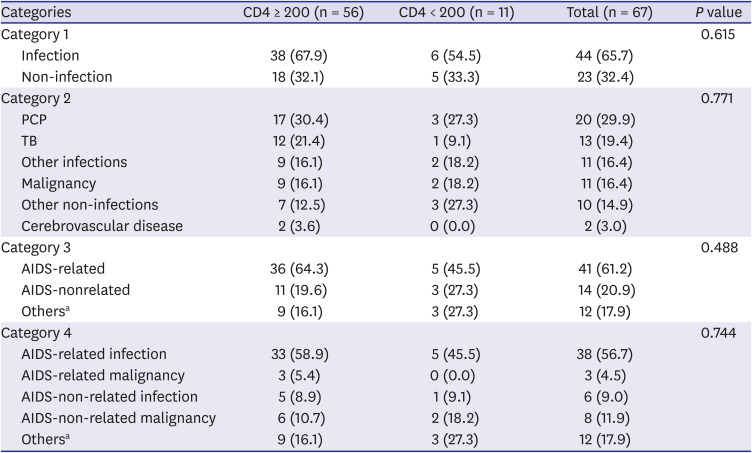
Table 2
Causes of death among human immunodeficiency virus-infected patients
Data are presented as number (%).
PCP = Pneumocystis pneumonia, TB = tuberculosis, AIDS = acquired immunodeficiency syndrome.
aOthers = liver cirrhosis 3, suicide 3, cerebrovascular disease 2, emphysema 1, pancreatitis 1, cardiovascular disease 1, burn 1.
![]()
In all patients, regardless of CD4 counts, the most common cause of death was PCP (20 patients [29.9%]), followed by TB (13 patients [19.4%]), as shown in category 2. Other infections included bacterial pneumonia (5 patients [7.5%]), sepsis (3 patients [4.5%]), cytomegalovirus infection specified as cytomegalovirus encephalitis (1 patient [1.5%]), pseudomembranous colitis (1 patient [1.5%]), and cryptococcal meningitis (1 patient [1.5%]) (Supplementary Fig. 3).
Non-infection related death was identified in 23 patients (Supplementary Fig. 4). Eleven HIV patients were determined to have malignancy-related deaths, diagnosed as liver cancer (3 patients [4.5%]), lung cancer (3 patients [4.5%]), lymphoma (2 patients [3.0%]), cerebral lymphoma (1 patient [1.5%]), leukemia (1 patient [1.5%]), and anal cancer (1 patient [1.5%]). AIDS-related malignancy accounted for 4.5% of the total deaths among HIV patients, and AIDS-non-related malignancy accounted for 11.9%. Among the 11 patients with malignancy-related death, AIDS-related malignancy death was found in 4 patients (36%) and AIDS-non-related malignancy death was found in 7 patients (64%) (Supplementary Fig. 5).
Other non-infection related death causes were identified as liver cirrhosis (3 patients [4.5%]), suicide (3 patients [4.5%]), cerebrovascular disease (2 patients [3.0%]), pancreatitis (1 patient [1.5%]), emphysema (1 patient [1.5%]), cardiovascular disease (1 patient [1.5%]), and burns (1 patient [1.5%]).
Regardless of the time of HIV diagnosis and CD4 counts, AIDS-related causes of death accounted for 41 patients (61.2%) and AIDS-non-related causes of death accounted for 26 patients (38.8%) (Table 2). The distribution of the 26 AIDS-non-related causes of death included AIDS-non-related malignancy (7 patients [26.9%]), bacterial infection and sepsis (6 patients [23%]), accidental cause (6 patients [23%]), liver disease (3 patients [11.5%]), and cardiovascular disease, pulmonary disease, gastrointestinal disease (1 patient each [3.8%]) (Supplementary Fig. 6).
The results of causes of death between CD4 < 200 cells/mm3 group and the CD4 ≥ 200 cells/mm3 group showed that infection accounted for 54.5% and 67.9%, and non-infection-related death accounted for 33.3% and 32.1%, respectively (P = 0.615). There was no statistical difference in the cause of death distribution between the 2 groups, regardless of category classification (Table 2).
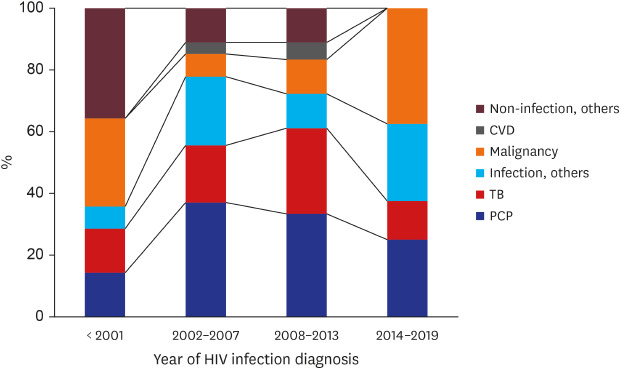
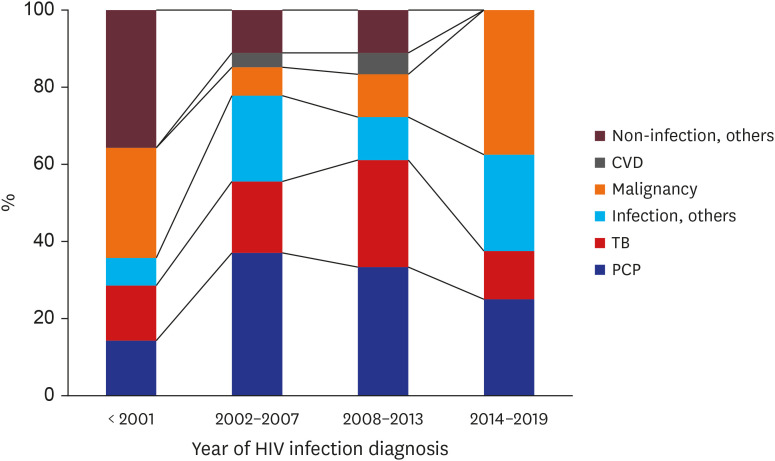
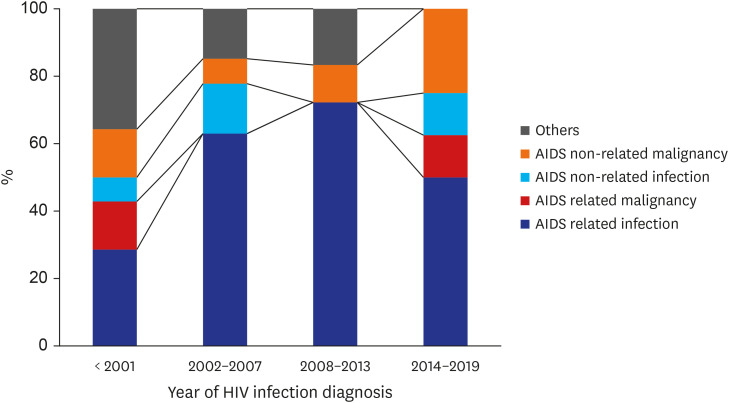
Changes in causes of death at different times of HIV diagnosis with 5-year intervals were evaluated. Significant changes over time were seen in the past 10 years. Infection-related deaths have decreased, whereas malignancy-related deaths have increased (Fig. 2). In particular, malignancy-related death has accounted for nearly 40% of the HIV patients diagnosed between 2014 and 2019. Although the PCP proportion was slightly reduced, it has continued to be the single most common cause of death among HIV patients (Fig. 2). According to AIDS-related death classification, AIDS-related deaths have decreased while AIDS-non-related deaths have increased (Fig. 3).
Among 67 death cases based on the year of death at 4-year intervals, it is noteworthy that the cause of death from malignancy has recently become the most common between 2015 and 2019 (Supplementary Fig. 7). AIDS-related deaths have decreased, whereas AIDS-non-related infection and malignancy have increased over the past 12 years. A remarkable trend in causes of death is that AIDS-related infection has decreased, while AIDS-non-related malignancy has increased between 2015 and 2019 (Supplementary Fig. 8).
DISCUSSION
In this study, we had a follow-up period of more than 20 years to monitor the changes in causes of death and the impact of low CD4 counts at the time of HIV diagnosis on death among HIV-infected patients in Korea. We elucidated that HIV patients diagnosed with CD4 < 200 cells/mm3 were not at greater risk of death compared with the CD4 ≥ 200 cells/mm3 group. Our study showed that PCP was the single most common cause of death among HIV patients in both the past and present, and that TB was the second leading cause of death from infections. These are similar to results of a previous study conducted in Korea between 1990 and 2011,6 but the frequency of these diseases has decreased in recent years. Malignant tumors have become an important cause of death in recent years, and an increasing tendency of AIDS-non-related malignancies was observed.
It is important to identify prognostic factors for survival among HIV-infected patients. Based on previous studies, CD4 cell count was suggested as the most important prognostic factor among the main risk factors for death.1213 It has been reported that CD4 cell count at the time of HIV diagnosis is the predominant prognostic factor for survival,14 and baseline CD4 counts are more relevant for AIDS-related causes of death. This observation has shown important implications for the clinical management of HIV patients.15 CD4 count at the start of ART is strongly associated with short-term survival, but its association with longer-term survival is less well characterized. A recent study conducted in North America and Europe suggested that patients with low baseline CD4 cell count only carry the burden of increased risk of death up to 5 years after ART.16 Another study conducted in China also showed that baseline CD4 count becomes a weak prognostic factor after 6 months of starting ART.17
In our study, there was no significant difference observed regarding long-term survival coming from baseline low CD4 count in this study. Though, the short-term survival rate (HIV diagnosis to death within 3 months) showed a higher survival rate in groups with CD4 counts less than 200 at the time of diagnosis. Among CD4 count < 200 cells/mm3 group patients, those who died within three months were not identified, which could be interpreted as a study limitation of the distribution of patients. This result showed that it is difficult to identify the association between the CD4 counts at the time of HIV diagnosis and short-term mortality rate, and further studies are needed to evaluate the associations.
Although our study did not include the ART status near the time of HIV diagnosis, we showed that WHO HIV stages at the time of HIV diagnosis and death were not statistically different between the CD4 < 200 cells/mm3 and CD4 ≥ 200 cells/mm3 groups.
A recently published prospective cohort study in Japan reported that late diagnosis (CD4 < 200 cells/mm3 at the first visit) was an independent risk factor for mortality among HIV patients.18 According to a previous large HIV population-based cohort study, the mortality rate was higher in patients with CD4 counts of 200 cells/mm3 or less, and a CD4 count of less than 200 is one of the factors associated with AIDS-related causes of death.19 However, in our study, the mortality rate and AIDS-related causes of death between CD4 < 200 cells/mm3 and CD4 ≥ 200 cells/mm3 groups showed no significant differences. This difference might be attributed to the fact that the previous study did not find a specific cause of death in 18.7% of patients.19
In addition, a previous study showed that socioeconomic disadvantage was strongly associated with poorer HIV treatment outcomes in settings with universal access to health care suggesting the importance of adherence to interventions and social support.20 Therefore, considering the association between socioeconomic status and drug adherence followed by compliance, we investigated the association of socioeconomic status with long term survival. We have found that a patient’s socioeconomic status did not show a statistical difference on the survival between the national health care group and MAP group, implying that other factors including the national HIV and AIDS strategy, which aimed to increase access to care, improve health outcomes and address health inequities might be playing an important role on an HIV patient's survival, as reported in a previous study.22122 Especially in Korea, there is no difference in access to hospitals based on income, as the government fully supports the cost of treating HIV patients. Even with late diagnosis, if the patients were on ART treatment, the clinical prognosis on survival could be similar, regardless of CD4 count at the time of HIV diagnosis and socioeconomic status.
HIV infection has become a chronic disease with the improvement of HIV treatment. Advances in ART, effectiveness in HIV suppression, decreased side effects, and increased ease of taking medications have contributed to these improvements.23 The introduction of combination ART also marked an important achievement toward prolonging the lifespan of HIV patients, resulting in shifting patterns in both mortality rates and leading causes of death in high-income countries.24
With more recent HIV diagnoses, HIV patients showed a tendency to die of non-infection-related causes. Among the non-infection death causes, malignancy accounted for approximately 40% of the deaths of patients diagnosed between 2014 and 2019, which is 2 times more than among cases diagnosed between 2008 and 2013.
Among HIV-infected patients, as rates of death owing to AIDS-attributable causes decreased, rates owing to non-AIDS-attributable causes also decreased, but the percentages of deaths resulting from non-HIV-attributable causes, such as heart disease and non-AIDS cancers, increased.25 It has been reported that AIDS-related deaths have decreased, whereas non-AIDS-related deaths, such as those because of non-AIDS malignancy or cardiovascular diseases, have increased among an aging cohort of HIV patients.2627
Korea is among the high-income countries, and our study also showed that AIDS-related deaths decreased, whereas non-AIDS-related deaths increased between 2015 and 2019. In New York, the percentage of deaths owing to non-AIDS-related causes increased by 32.8% (from 19.8% to 26.3%; P = 0.015) between 1999 and 2004. Among deaths owing to non-AIDS-related causes, 76% could be attributed to non-AIDS-defining types of cancer, cardiovascular disease, or substance abuse.28 A recently published Canadian population-based cohort study showed that non-AIDS-defining cancers are currently the leading non-AIDS-related cause of death in HIV-infected patients.29 Our study also showed that between the years of 2015 and 2019, AIDS-non-related disease has become an important cause of death and AIDS-non-related malignancy is currently the leading non-AIDS-related cause of death. It has been also confirmed that the incidence of malignant tumors increases with age, accounting for about 1% of those under 60 and about 4% of those over 60. The increasing number of HIV patients dying of diseases non-related to AIDS can be explained by the improvement of drugs and the improvement of patients' compliance through HIV counseling projects. Among non-AIDS-related deaths, the incidence of cerebrovascular disease was lower than expected and there was no death owing to cardiovascular disease or drug dependency in this study.
According to a study of specific causes of death in Japan between 2005 and 2016, AIDS-related malignancies accounted for 24%, non-AIDS-defining malignancies for 23%, and AIDS-defining infections accounted for 15%.18 Although the study period was somewhat different from our study period, the most common cause of AIDS-defining infection was PCP, which was similar to our study. However, the second most common cause of infection was found to be progressive multifocal leukoencephalopathy in Japan compared with our finding of TB in Korea. Infection cause of death priorities appear to be different depending on high prevalence infectious diseases, such as TB. Toxoplasmosis was found in 2 patients (0.01%) in the Japanese study. However, there was no death from toxoplasma infection in this study. Among the AIDS-defining malignancies, lymphoma was the most common cause in the Japanese study. Death from AIDS-associated malignancies was also caused mainly by lymphomas in this study. Death from the Kaposi’s sarcoma was found in 2 patients (0.015%) in the Japanese study, but there was no death from Kaposi's sarcoma in our study. Suicide as the cause of death accounted for 8.5% of deaths in Japan, whereas this accounted for 4.5% in our study.
This study has several limitations. First, our study was conducted at a single center in Korea. Therefore, our findings may not be generalized to other regions of the country. Nevertheless, this was the first study in Korea to elucidate the trends of causes of death in HIV patients in the past 20 years. Second, it was not possible to identify the survival of follow-up loss patients and, in cases of death outside of the hospital there was a restriction on the cause of death analysis. Therefore, we had to exclude 4 patients who died outside of the hospital with unidentified causes of death. However, these numbers did not seem significant compared with the total number of deaths among HIV patients included in the death cause analysis, accounting for approximately 5%. Third, our database did not include data regarding ART adherence. We could not identify whether the patients continued to receive ART near their deaths or not; nor could we identify ART start time after HIV diagnosis. This may result in bias in the interpretation of the survival results according to the baseline CD4 count difference. Nevertheless, we believe that this study is worthy of sustained attention because our study demonstrated that there was no statistical difference regarding ever ART history and long-term survival analysis of overall causes of death, including AIDS-related death between the CD4 < 200 cells/mm3 group and the CD4 ≥ 200 cells/mm3 group.
In conclusion, our results showed that patients diagnosed with CD4 < 200 cells/mm3 are not at greater risk of death than those with CD4 ≥ 200 cells/mm3, and those diagnosed with HIV in more recent years show a tendency to die from non-AIDS-related diseases, suggesting that the effectiveness of ART and improved and solid medical care cascade systems greatly contribute to this. Ongoing monitoring of mortality trends by causes of death will continue to be important and will provide the necessary data to enable appropriate targeting of interventions to improve the quality of patient care and reduce avoidable mortality.
 XML Download
XML Download