

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
N-terminal pro-B type natriuretic peptide (NT-proBNP) is a well-known prognostic biomarker in heart failure (HF).123 NT-pro BNP is a marker of ventricular overload and myocyte stress; however, it has a known limitation of being affected by age, renal function, atrial fibrillation, etc.4 Accordingly, a multimarker prognostic stratification strategy for patients with HF would be desirable. The activation of the renin-angiotensin-aldosterone system (RAAS) results in a series of complex enzymatic reactions that culminate in the generation of angiotensin II, the main effector molecule of the system, central to multiple causal pathways in hypertension, HF, and atherosclerosis.5 Plasma renin activity (PRA) has been suggested to be a surrogate of RAS activation and a marker of increased cardiovascular risk.67891011 However, in patients with HF, the association of PRA and NT-proBNP has not been fully investigated. This study aimed to determine the association between PRA and NT-proBNP and to investigate the incremental value of PRA to NT-proBNP for predicting long term prognosis in patients with acute HF.
Go to : 
METHODS
Study populations
This was a retrospective single-center study including 546 patients from December 2004 to July 2013. Patients with newly diagnosed HF and those with acute exacerbations of chronic HF were included. The diagnosis of HF was determined by the history, symptoms, physical examination, pulmonary congestion on chest X-ray, and instrumental findings for the assessment of structural myocardial involvement. Cardiac morphology and function were assessed by 2-dimensional Doppler echocardiography. The inclusion criterion was patients over 18 years of age. The exclusion criterion was patients in whom PRA and NT-proBNP were not measured simultaneously. The prognosis was assessed using composite events of all-cause mortality and readmission for HF. During the follow-up period, data were obtained by reviewing medical records and telephone interviews with patients or with their relatives.
Blood sampling and assays
Plasma NT-proBNP levels were measured by the SIEMENS diagnostic assay (Dimension VISTA 1500; Siemens, München, Germany). PRA levels were measured using the radioimmunoassay Angiotensin I RIA KIT (IM3518; Beckman Coulter, Prague, Czech Republic). Coefficients of variations were 11.3% and 20.9% for intra-assay and inter-assay variation, respectively. Blood samples were drawn at 8.00 am after an overnight fast, according to a standardized experimental protocol.12
Statistical analysis
Data are expressed as mean ± standard deviation (SD) for continuous variables and percentages (%) for categorical variables. Student's t-test was used to compare continuous variables while Pearson's χ2 test was used for categorical variables. Univariate analyses were performed to determine the clinical predictors of cardiac death. The Cox proportional hazards model was used to determine independent predictors of cardiac death during the follow-up period. Variables with P values of < 0.05 on univariate analysis were selected and entered into the multivariate Cox proportional hazards analyses to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs) of adverse events during follow-up periods. The optimal cut points for PRA and NT-proBNP were quantified using receiver operating characteristic (ROC) curves. The cumulative incidence rates of the composite outcome of all-cause mortality and readmission for HF during follow-up periods according to the cutoff values for PRA and NT-proBNP were estimated by using the Kaplan-Meier method and compared by using the log-rank test. The increased discriminative value after the addition of log-transformed NT-proBNP and/or log-transformed PRA to clinically relevant variables was estimated using 3 measures (the Harrell's C index, net reclassification improvement [NRI], and integrated discrimination improvement [IDI]). The Harrell's C index (C-statistic) is defined as the proportion of usable patient pairs, in which the prediction and outcomes are concordant.13 We estimated ROC curves and compared the areas under the ROC curves (C-statistics with 95% CI) in corresponding logistic models.14 The NRI and IDI were calculated by analyzing the differences in individual estimated probabilities for the prognosis after the addition of log-transformed NT-proBNP and/or log-transformed PRA to a model containing clinically relevant variables.15 Given that no prior risk categories exist for the composite outcome of all-cause mortality and readmission for HF, we calculated the category-free NRI.15 For all analyses, a two-sided p-value of < 0.05 was considered statistically significant. Statistical analysis was performed using the software R (version 4.0.2; R Foundation for Statistical Computing, Vienna, Austria) statistical.
Ethics statement
The Institutional Review Board of the Kyungpook National University Hospital approved this study (approval No. KNUIH 2020-04-022). The need for informed consent was waived by the board.
Go to :
RESULTS
Baseline characteristics
The baseline characteristics of the study subjects are shown in Table 1. The mean age ± SD was 64.7 ± 15.9 years, and 212 (53.5%) were male. The etiology of HF was ischemic in 116 (29.3%) patients, 148 patients had idiopathic HF, 46 had tachycardia-induced cardiomyopathy, 25 had valvular heart disease, 17 had hypertension-related HF, 15 had stress-induced cardiomyopathy, 14 had hypertrophic cardiomyopathy, 7 had restrictive cardiomyopathy, 6 had myocarditis, and 2 had unknown cause HF.
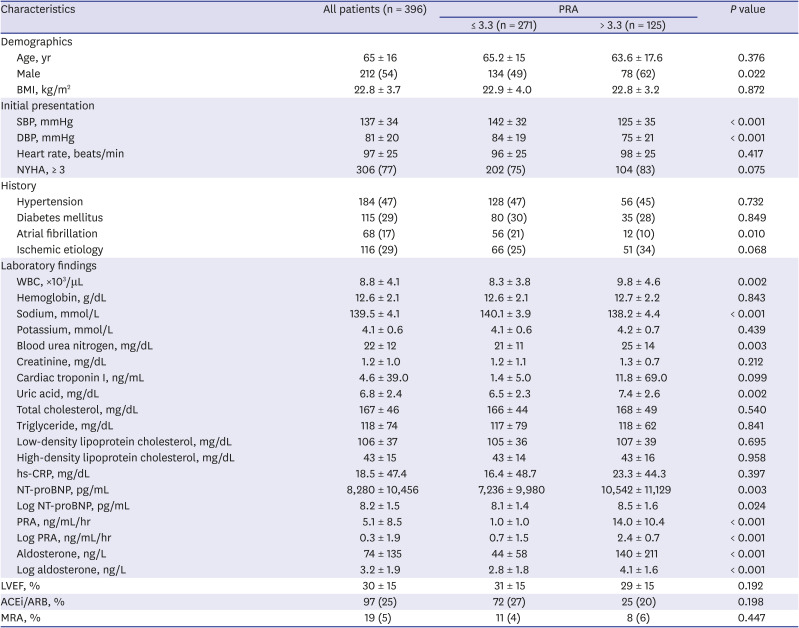
Table 1
Clinical characteristics of patients according to PRA value ≤ 3.3 or > 3.3 ng/mL/hr cutoff values
Data are presented as mean ± standard deviation or number (%).
PRA = plasma renin activity, BMI = body mass index, SBP = systolic blood pressure, DBP = diastolic blood pressure, NYHA = New York Heart Association Functional Classification, WBC = white blood cell, hs-CRP = high-sensitivity C-reactive protein, NT-proBNP = N-terminal pro-B type natriuretic peptide, LVEF = left ventricular ejection fraction, ACEi = angiotensin-converting enzyme inhibitor, ARB = angiotensin receptor blocker, MRA = mineralocorticoid receptor antagonist.
![]()
During the 2-year follow-up period, 119 (30.1%) composite events and 96 (24.2%) deaths were observed.
Association between PRA levels and the prognosis of the patients with acute HF
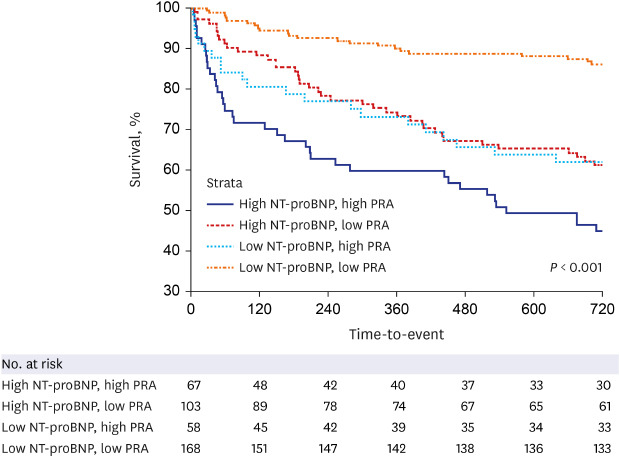
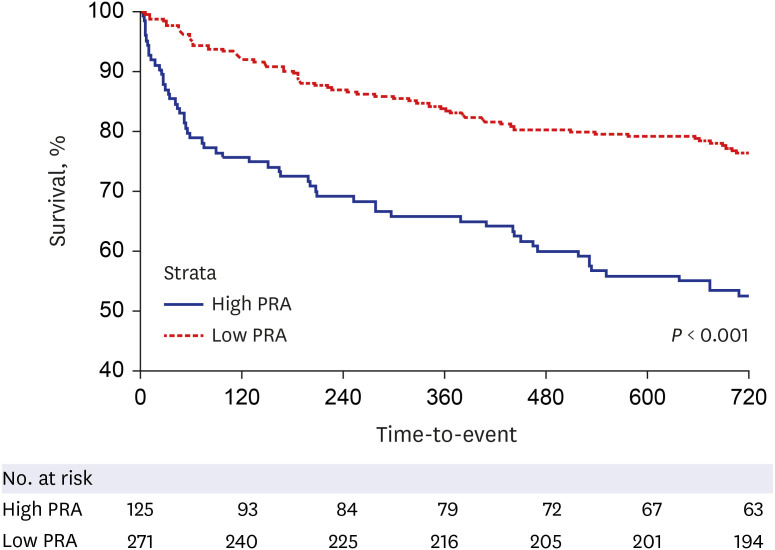
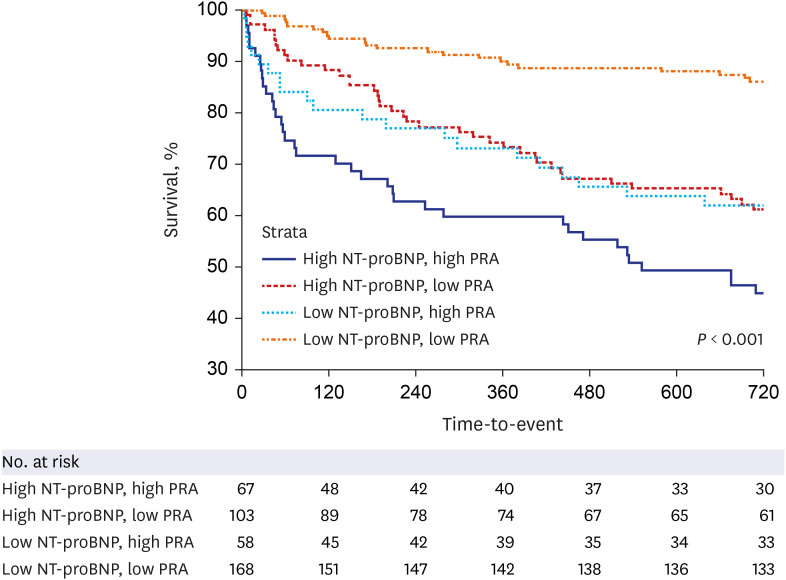
On ROC analysis, the cutoff value of 3.3 ng/mL/hr for PRA best predicted composite outcome of all-cause mortality and readmission for HF (area under the ROC curve 0.650; sensitivity 50%, specificity 73%). As shown in the Kaplan-Meier analysis, patients with PRA > 3.3 ng/mL/hr had a higher rate of the composite outcome of all-cause mortality and readmission for HF in two years (n = 61 in the low PRA group vs. n = 58 in the high PRA group) (Fig. 1). All-cause mortality for 2 years was confirmed by 48 events (17.7%) out of 271 in the Low PRA group and 48 events (38.4%) out of the 125 High PRA. On ROC analysis, the optimal cutoff value for log-transformed NT-proBNP was 5,190 pg/L for cardiac death (area under the ROC curve 0.668; sensitivity 64%, specificity 66%). As shown in Fig. 2, patients with an elevation of both biomarkers showed the highest risk of the composite outcome of all-cause mortality and readmission for HF; those with either high PRA or NT-proBNP showed an intermediate outcome, while the subset with both markers below the ROC cutoff values presented the lowest rate of composite outcome (log-rank P < 0.001). In addition, in-hospital death was confirmed in 12 patients (4.4%) in the low PRA group and 26 patients (20.8%) in the high PRA group, respectively. The Kaplan-Meier survival analysis revealed significant differences between the PRA levels of both groups (log-rank P < 0.001). In the univariate model, age, sex, systolic blood pressure, diastolic blood pressure, New York Heart Association Class III to IV, left ventricular ejection fraction (LVEF), diabetes mellitus, ischemic etiology, white blood cell (WBC) count, hemoglobin level, sodium level, blood urea nitrogen, low-density lipoproteins, log-transformed PRA, and log-transformed NT-proBNP were significant association with composite outcome. In the multivariate model, age, LVEF, WBC, and log-transformed PRA were independent predictors for the composite outcome.
Incremental predictive value of the PRA
The incremental predictive values of log-transformed PRA in the Cox proportional hazards model are shown in Table 2. The PRA added incremental value to the combination of age, sex, LVEF, and log-transformed NT-proBNP in predicting the composite outcome of all-cause mortality and readmission for HF. The reclassification of patients with or without composite outcome at the time of 2-year follow-up is presented in Table 3. The addition of log-transformed NT-proBNP to age, sex, and LVEF yielded an NRI of 0.31 (P < 0.003) and 0.03 of IDI (P < 0.001). The addition of PRA to WBC count, age, and log-transformed NT-proBNP also significantly improved the reclassification (0.47; P < 0.001) and the integrated discrimination (0.10; P < 0.001) of subjects compared to the previous model.
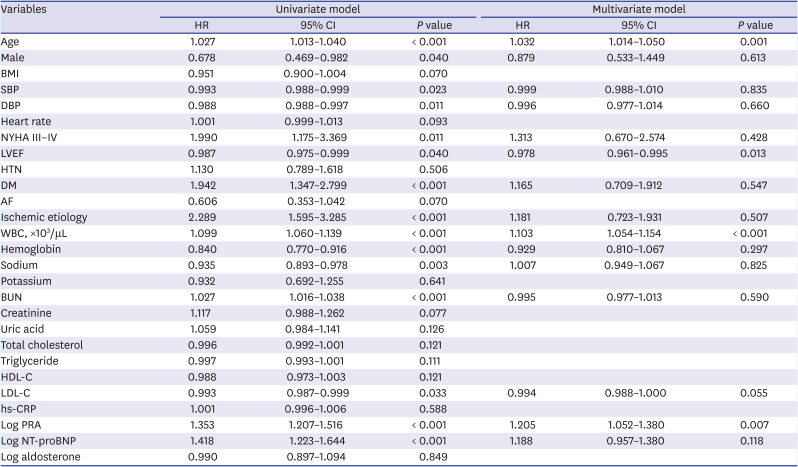

Table 2
Univariate and multivariate models for the composite outcome of all-cause mortality and readmission for heart failure using Cox-proportional hazards regression
HR = hazard ratio, CI = confidence interval, BMI = body mass index, SBP = systolic blood pressure, DBP = diastolic blood pressure, NYHA = New York Heart Association Functional Classification, LVEF = left ventricular ejection fraction, HTN = hypertension, DM = diabetes mellitus, AF = atrial fibrillation, WBC = white blood cell, BUN = blood urea nitrogen, HDL-C = high-density lipoprotein cholesterol, LDL-C = low-density lipoprotein cholesterol, hs-CRP = high-sensitivity C-reactive protein, PRA = plasma renin activity, NT-proBNP = N-terminal pro-B type natriuretic peptide.
![]()
Table 3
Discrimination of multivariate logistic regression models in predicting all-cause mortality and readmission for heart failure
Model 1 = age + sex + left ventricular ejection fraction; Model 2 = Model 1 + log NT-proBNP; Model 3 = Model 2 + log PRA.
NRI = net reclassification improvement, IDI = integrated discrimination improvement.
![]()
Go to :
DISCUSSION
In the present study, the main findings were that the baseline PRA level at admission was an independent prognosticator for the composite outcome of all-cause mortality and readmission for HF in patients with acute HF. Moreover, PRA had a predictive value incremental to the combination of NT-proBNP and clinically relevant risk factors.
The activation of neurohormonal axes, in particular of the RAAS as a maladaptive response to cardiac dysfunction, plays a key role in the evolution and outcome of HF.16171819 High circulating concentrations of PRA and natriuretic peptides have been found in patients with HF.2021 However, few data are available on the relative independent contribution of PRA and NT-proBNP to predict outcome in HF when compared directly in the same patient population.
Our results are consistent with previous studies, showing that PRA is a strong prognosticator in patients with HF. In addition, PRA and NT-proBNP together, appear to provide additive prognostic information.
The domain of cardiac biomarkers is rapidly expanding and novel markers are emerging fast. Unfortunately, only few do reach a level of clinical significance and are chosen for use in clinical practice. In the present study, PRA showed favorable results for predicting the composite outcome of all-cause mortality and readmission for HF in patients with HF. Therefore, PRA might be a useful prognostic biologic marker in patients with HF. Recent studies have shown that baseline PRA levels are highly associated with 30-day HF rehospitalization or death in patients with acute HF.22 Moreover, there has been a study that showed that high PRA levels are significantly related to mortality and rehospitalization when patients with acute HF are treated after optimal medical treatment.2324
Our study had several limitations. First, the retrospective analysis of prospectively collected data is a major limitation of this study. Therefore, we cannot completely exclude the possibility of residual confounding factors, and our results should be interpreted with caution. Second, because of the limited sample size, the patients in our study might not be representative of the entire population of HF. Third, PRA was measured only at baseline, so the effect of discharge medication on the relationship between PRA and mortality could not be further investigated. The previous medical history of study subjects may affect PRA levels. However, there were no differences between low and high PRA groups in patients taking angiotensin-converting enzyme inhibitor (ACEi)/angiotensin receptor blocker (ARB) or mineralocorticoid receptor antagonist (MRA) with baseline anti-hypertensive medication (Table 1). Moreover, taking ACEi/ARB or MRA before hospitalization did not affect the prognosis of patients in univariate analysis. A plausible explanation may be that the study population was targeted at patients with acute decompensated HF, and the RAAS system can be overactivated regardless of medication.
In conclusion, our results suggest that PRA is an independent prognosticator in patients with HF and has a predictive value incremental to the combination of NT-proBNP. Further studies are required in a larger population to confirm the association between PRA and NT-proBNP for the prognosis in patients with acute HF.
Go to :
 XML Download
XML Download