

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of heart failure is continuously increasing worldwide and, accordingly, patients suffering from advanced heart failure with refractory symptoms despite optimal medical treatment and device therapy who require either a durable left ventricular assist device (LVAD) or a transplanted heart to survive also constitute a significant number of individuals.1234 However, the number of heart donors is limited, and many critically ill patients are not receiving such treatment in a timely fashion.56 For these patients, recently, temporary mechanical circulatory support (MCS) options such as percutaneous ventricular assist devices (VADs), surgically implanted extracorporeal VADs, and veno-arterial extracorporeal membrane oxygenation (VA-ECMO) systems have become increasingly used as bridges to heart transplantation (HT).5678
In Korea, high suicide rates and accidents leading to death lead to the existence of a relatively short time before an adequate donor heart may be available once the patient is placed on the waiting list with an INTERMACS profile 1 or 2 designation. Also, priority status is given when VA-ECMO is applied, making it the selection of choice for temporary MCS rather than other options, while insurance issues in Korea push for the same.79 Prior studies have reported that such strategies might be feasible, but only case reports could be found demonstrating whether an early extubation ECMO approach is beneficial in patients awaiting HT, although several studies have indicated the merit of early extubation ECMO in patients who received veno-venous ECMO while waiting for lung transplantation.1011 Therefore, we sought to investigate the clinical outcomes of patients who received VA-ECMO as a bridge to transplantation and compared them between those receiving early extubation ECMO and deferred extubation ECMO, respectively.
METHODS
Study population
The current study was a retrospective, single-center, observational study involving patients who underwent VA-ECMO as a bridge to HT between November 2006 to December 2018 at Samsung Medical Center in Seoul, Korea. All study participants were 18 years or older and were expected to receive optimal medical treatment according to current guidelines.12 VA-ECMO was indicated when a patient experienced refractory cardiogenic shock equivalent to INTERMACS profile 1 or 2 and was placed on the national organ transplant registry with the intention of undergoing HT.12 A total of 102 patients were eligible for inclusion in this study. The final decision to implant VA-ECMO was determined by an experienced medical team, and the VA-ECMO apparatus itself was inserted at the bedside or in a catheterization laboratory by cardiovascular surgeons or interventional cardiologists.
Implantation of the VA-ECMO device and management
The management of VA-ECMO was thoroughly introduced previously.13 In short, a VA-ECMO device was inserted by percutaneous cannulation using the Seldinger technique or surgical cannulation using the cut-down method. A 14- to 17-French arterial cannula and a 20- to 24-French venous cannula were used. Femoral vessels were usually utilized as vascular access sites. The Capiox® Emergency Bypass System (Terumo, Inc., Tokyo, Japan) and the Permanent Life Support system (Maquet, Rastatt, Germany) were available in our hospital at the time of the study. In the event of distal limb ischemia after arterial cannulation, a catheter was inserted distal to the cannulation site for limb perfusion. Pump speed was adjusted to obtain a cardiac index of greater than 2.2 L/min/body surface area (m2), a mean arterial pressure of more than 65 mmHg, and a central mixed venous saturation of more than 70%. Intravenous heparin was infused to maintain an activated clotting time ranging from 150 to 180 seconds unless life-threatening bleeding was observed. Successful weaning was defined as the disconnection of the patient from ECMO without reinsertion or death within 24 hours.
Data collection, definition, and clinical outcomes
We obtained additional information retrospectively by reviewing patient medical records from the Samsung Medical Center ECMO registry. When the same laboratory data were measured several times before ECMO insertion, the laboratory value measured at the time nearest to ECMO insertion was used. The duration of intensive care unit (ICU) stay during the whole admission period and the length of hospital stay after discharge from the ICU were measured in days. The durations on mechanical ventilation, of ICU stay, and of hospital stay after transplantation were additionally collected in patients who successfully underwent HT.
A patient was defined as being part of the early extubation ECMO group if their intubated period was 48 hours or less during the time period of VA-ECMO. For patients who received durable LVAD, the duration of early extubation ECMO was calculated as only until the time LVAD implantation was finished. Previous studies considered early extubation ECMO as either being not intubated at any time or having a relatively short duration of mechanical ventilation, but no specific time cutoff was able to be identified.14151617 Therefore, we hypothesized that the definition of early extubation ECMO as being when a patient is intubated for 48 hours or less would have significant clinical meaning reflecting current definitions of ventilator-associated pneumonia.18
Delirium was diagnosed according to the Confusion Assessment Method for the ICU (CAM-ICU) and was measured both before and after HT.19 Infection cases were defined as those in which blood, sputum, urine, skin swab, or relevant cultures were positive and associated symptoms manifested, requiring antibiotics.20
The primary outcome was in-hospital mortality, while secondary outcomes included HT success rate, ECMO successful removal rate, delirium occurrence, infection, and ICU stay duration.
Statistical analysis
Categorical variables are presented as numbers and relative frequencies and their group differences were compared using the chi-squared test or Fisher's exact test as appropriate. Continuous variables are presented as means ± standard deviations or medians (25th–75th percentiles) and their group differences were compared using a Student's t-test or the Mann-Whitney U test where appropriate. Survival curves after HT were estimated by means of the Kaplan–Meier method and compared using a log-rank test. Statistical analyses were performed using the SPSS version 25 (IBM Corp., Armonk, NY, USA) and R version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria) software programs, with P < 0.05 considered to be statistically significant.
RESULTS
Study population
Among 102 patients presenting with refractory cardiogenic shock treated with VA-ECMO for bridge to transplantation, 67 were diagnosed with dilated cardiomyopathy (65.7%), 12 were diagnosed with ischemic cardiomyopathy (11.8%), nine were diagnosed with acute myocardial infarction (8.8%), four were diagnosed with myocarditis (3.9%), three were diagnosed with hypertrophic cardiomyopathy (2.9%), and seven were diagnosed with other causes (6.9%). Patients were classified either into the early extubation ECMO group (n = 24) or deferred extubation ECMO group (n = 78), as shown in Fig. 1. Eleven patients died before HT in the deferred extubation group and two patients died before HT in the early extubation group. Separately, seven deferred extubation group patients were able to be weaned from ECMO, and two patients in the early extubation group underwent durable LVAD before being successfully transplanted. Table 1 shows the baseline clinical and laboratory characteristics of the subjects at the time of VA-ECMO initiation. As compared with the deferred extubation group, patients in the early extubation group were more likely to be male and to undergo left ventricular decompression and less likely to have diabetes mellitus or a history of cerebrovascular disease.
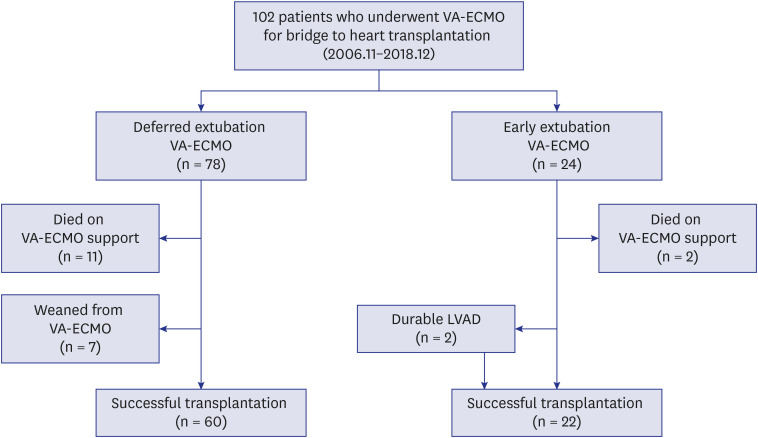
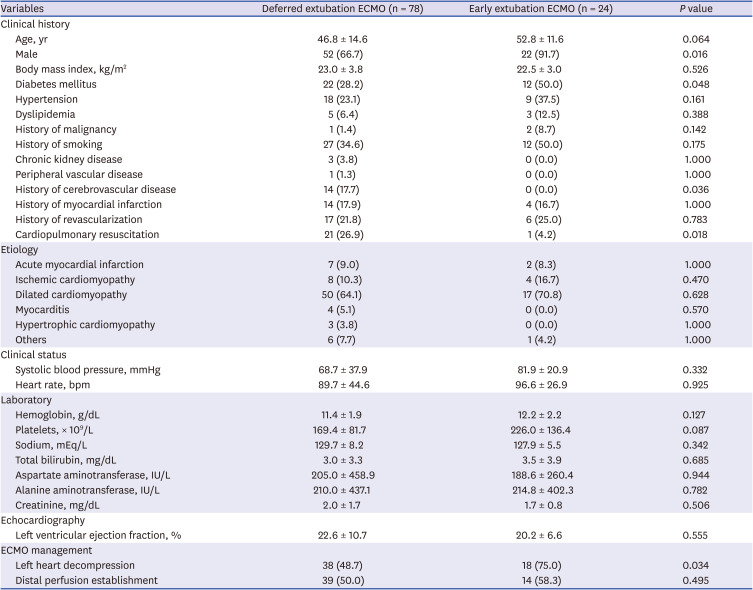
Fig. 1
Study population. Flow chart of patients, who received VA-ECMO as a bridge to heart transplantation. The patients were classified into either early extubation group or deferred extubation group depending on the length of period intubated.
VA-ECMO = veno-arterial extracorporeal membrane oxygenation.
![]()
Table 1
Baseline characteristics
Data are presented as mean ± standard deviation or number (%).
ECMO = extracorporeal membrane oxygenation.
![]()
Clinical outcomes
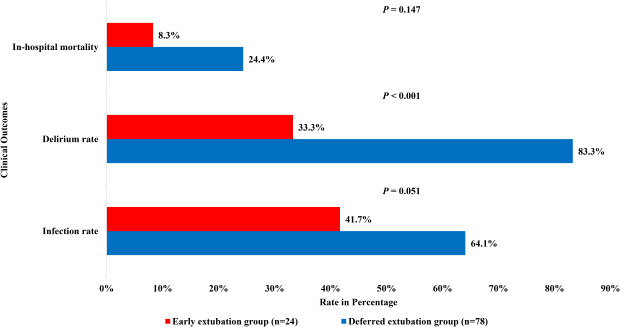
The number of patients who were in the early extubation ECMO group is presented in Fig. 2 according to the duration on ECMO without mechanical ventilation in days with a median duration of 10.0 (4.3–17.3) days. The total period during which patients from both groups were on ECMO is indicated in Supplementary Fig. 1. Clinical outcomes were presented in Tables 2 and 3. Two patients (8.3%) died during the index hospitalization in the early extubation ECMO group, while 19 patients (24.4%) died during the same period in the deferred extubation group (P = 0.147). Successful HT rates during ECMO support were 91.7% (n = 22) and 76.9% (n = 60) in patients classified as early extubation and deferred extubation, respectively (P = 0.147). Additionally, the rates of patients who were successfully weaned from ECMO either by HT or recovery were 91.7% (n = 22) and 85.9% (n = 67), respectively (P = 0.728). Delirium occurred in eight (33.3%) early extubation group patients and 65 (83.3%) deferred extubation group patients (P < 0.001). Infection of any site was found in 10 (41.7%) and 50 (64.1%) patients, respectively (P = 0.051). In particular, hospital-acquired pneumonia was seen in five (20.8%) and 34 (43.6%) patients of the early extubation and deferred extubation groups (P = 0.045). The total ICU stay durations were 21.5 (16.3–40.3) and 27.5 (20.0–45.5) days and the periods of hospital stay after ICU were 22.0 (15.8–33.5) and 17.0 (8.8–43.3) days, respectively, with no statistically significant differences.
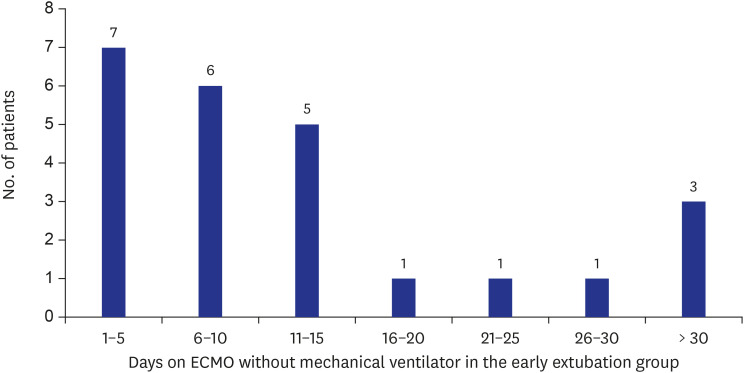
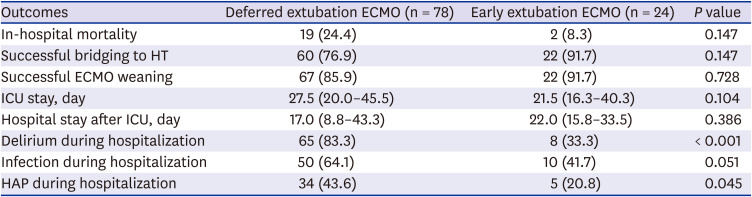
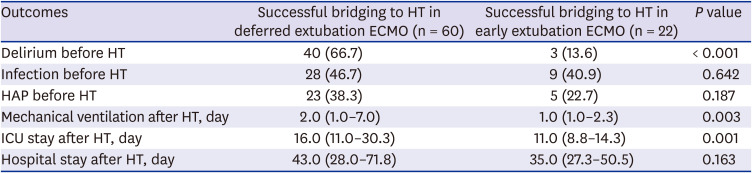
Fig. 2
Duration of ECMO without mechanical ventilation in the early extubation group. A total of 24 patients were in the early extubation ECMO group. The length of period on early extubation ECMO for each patient ranged from 1 to 44 days with a median duration of 10.0 (4.3–17.3) days.
ECMO = extracorporeal membrane oxygenation.
![]()
Table 2
Clinical outcomes of the study population
ECMO = extracorporeal membrane oxygenation, HT = heart transplantation, ICU = intensive care unit, HAP = hospital-acquired pneumonia.
![]()
Table 3
Clinical outcomes in patients who were successfully bridged to heart transplantation
Data are presented as median (interquartile range) or number (%).
HT = heart transplantation, ECMO = extracorporeal membrane oxygenation, HAP = hospital-acquired pneumonia, ICU = intensive care unit.
![]()
Among patients who were successfully bridged to HT, delirium occurrence rates were 13.6% (n = 3) and 66.7% (n = 40) infection rates were 40.9% (n = 9) and 46.7% (n = 28) and hospital-acquired pneumonia rates were 22.7% (n = 5) and 38.3% (n = 23) respectively for early extubation and deferred extubation patients (P < 0.001, P = 0.642, and P = 0.187). After HT, patients were on mechanical ventilation for 1.0 (1.0–2.3) and 2.0 (1.0–7.0) days, respectively (P = 0.003). Early extubation group patients stayed in the ICU and hospital after HT for 11.0 (8.8–14.3) and 35.0 (27.3–50.5) days, while deferred extubation group patients did so for 16.0 (11.0–30.3) and 43.0 (28.0–71.8) days (P = 0.001 and P = 0.163).
Survival curves, as depicted in Fig. 3, showed a survival rate of 89.7% in the first year after HT. The estimated five-year survival rate determined using the Kaplan-Meier method was 84.0% with a median follow-up duration of 637.5 (281.5–1,548.8) days.
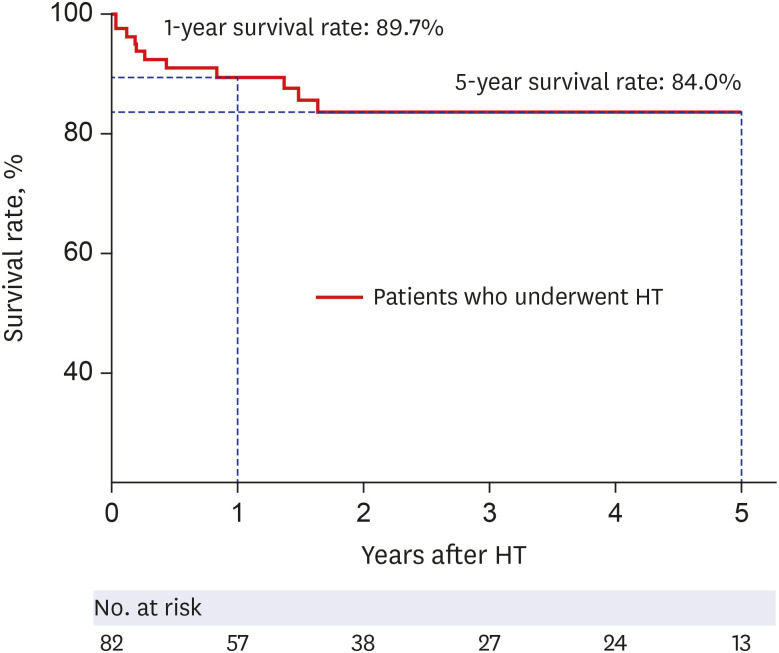
Fig. 3
Survival of patients bridged to HT with veno-arterial extracorporeal membrane oxygenation. Kaplan-Meier curve in heart transplantation recipients is shown, demonstrating a 1-year survival rate of 89.7% and a 5-year survival rate of 84.0% during the median follow up period of 637.5 (281.5–1548.8) days.
HT = heart transplantation.
![]()
DISCUSSION
In the present study, we sought to investigate the clinical outcomes of VA-ECMO as a bridge therapy in patients with refractory cardiogenic shock who were expected to have short waiting times for HT and compared them among early extubation and deferred extubation VA-ECMO strategy groups. The main findings were as follows. First, the short-term and long-term survival rates of VA-ECMO as bridge therapy in settings with relatively short expected times to transplantation are acceptable given the results of previous HT cohort research. Second, the early extubation ECMO strategy is feasible even in patients who used VA-ECMO as a bridge to transplantation. Third, the in-hospital mortality rate was numerically lower while delirium occurrence and infection, especially hospital-acquired pneumonia, were significantly lower in the early extubation group than in the deferred extubation group. Fourth, subgroup analysis including successfully transplanted patients showed that postoperative days on mechanical ventilation and ICU stay length in days were also significantly lower in the early extubation group.
The shortage of donor hearts and the increasing number of patients on the waiting list for HT mandates some form of MCS be deployed in a subset of candidates.5621 Durable LVAD might be considered as a bridge to HT since it allows for recovery from organ damage and an improvement in patient quality of life.22 However, the high costs of LVAD therapy and resulting insurance reimbursement issues together with limited efficacy evidence and concerns regarding posttransplant mortality also exist.232425 Comparable outcomes in recipients with pretransplant temporary MCS are increasingly being reported and many centers have begun applying VA-ECMO before HT.726 In our study, survival analysis using the Kaplan–Meier method also demonstrated a one-year survival rate of 89.7%, which is comparable to that of nonbridged transplant recipients.23 Currently, successful bridging to transplantation has been reported on in previous studies with rates ranging from 44% to 76.3%.727 However, in this study, 82 (80.4%) out of 102 patients were able to survive until HT with an even higher survival rate of 91.7% in the early extubation VA-ECMO group. A recent investigation reported a success rate of 91.2% attributed in part to the high volume of procedures conducted and the management protocols specific to the institution involved in the study, but, according to the implications of our study, the outcome could have been more influenced by most patients being subjected to early extubation ECMO, since a fairly large number of them were extubated shortly after VA-ECMO commencement.26 While it seems plausible for VA-ECMO to be used as a bridge therapy, adopting the early extubation ECMO strategy might provide even better clinical outcomes and encourage temporary MCS such as VA-ECMO to be more widely used in urgent situations before definitive therapy.
The early extubation ECMO strategy has previously been deployed in patients waiting for lung transplantation with studies conducted as early as 2010.17 A few other subsequent studies revealed promising results with higher survival rates after discharge and shorter periods of hospital stay and mechanical ventilation.141516 Allowing for spontaneous breathing to occur during VA-ECMO application has some merits as compared with mechanical ventilation, as it helps to prevent ventilator-induced diaphragm dysfunction and ventilator-/intubation-associated pneumonia, reduce delirium and facilitate improved rehabilitation and interactions with medical staff.10 Likewise, the strategy has been attempted in patients undergoing high-risk percutaneous coronary intervention or suffering from refractory cardiogenic shock, but no studies involving a population bridged to transplantation were found.282930 Therefore, we investigated whether the use of an early extubation ECMO strategy is beneficial in patients who received VA-ECMO as a bridge to HT and found that early extubation VA-ECMO was associated with reductions in the rates of delirium and infection. A subgroup analysis with successfully transplanted patients also showed the existence of less postoperative days on mechanical ventilation and reduced ICU stay length in the early extubation group, presumably leading to reductions in medical costs and complications related to prolonged hospitalization.
The feasibility of early extubation VA-ECMO might be controversial since many patients who are intubated may have just indications. With no definite protocols concerning indications of intubation and mechanical ventilation before VA-ECMO application, many patients are routinely intubated before the procedure and possibly are not extubated for reasons such as keeping their priority status on the waiting list. However, at our institution, 19 patients were not intubated at all, undergoing VA-ECMO insertion only with local anesthesia while communicating with the medical staff. In a study conducted in a Russian hospital, 84.1% of patients were able to be extubated within one hour after the commencement of VA-ECMO and only 17.0% were reintubated.26 Of the intubated patients in our study, 47 (56.6%) were established as such to protect the airway in situations of altered mental status resulting in cardiopulmonary resuscitation or elective procedures. This, along with the fact that five patients were able to be extubated within 48 hours, suggests that the early extubation ECMO strategy might be applicable in a broader spectrum of patients with close monitoring of the patient's status and early detection of hemodynamic compromise to minimize situations of cardiopulmonary resuscitation.
Our study had several limitations that should be highlighted. First, this study was a single-center study from a tertiary referral center and thus had a significant potential for inherent selection and referral biases. Second, we may not be able to exclude the influence of a time difference, as the early extubation ECMO strategy was mainly used after 2016 in our institution. Also, due to the study's observational design, it should be noted that it is not totally exempt from the criticism that patients who were originally in better condition were subjected to the early extubation ECMO strategy, leading to better outcomes. Third, due to the retrospective and observational nature of this study, there were no pre-defined indications for early extubation. However, we attempted to aggressively extubate as early as possible whenever the patient was of clear consciousness and passed the test for weaning from the ventilator which are probably the cases when most other patients on mechanical ventilators are extubated. Finally, the small sample size of this study might have limited its statistical precision. Despite seemingly significant differences in numbers, statistical significance was not achieved in in-hospital mortality or survival curves by means of the Kaplan-Meier method.
In conclusion, VA-ECMO as a bridge therapy seems to be feasible in candidates waiting for HT and the early extubation ECMO strategy was specifically associated with a lower in-hospital mortality rate and reductions in both delirium and infection onset in this population. Further investigation is needed to clarify the optimal patient selection criteria for early extubation VA-ECMO and to elucidate the best timing of VA-ECMO to allow such a strategy to be successfully employed.
 XML Download
XML Download