

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endoscopic resection has been increasingly used for the treatment of superficial esophageal squamous carcinoma (SESC).12 To overcome the challenges of the inevitable morbidity and mortality associated with radical esophageal resection, endoscopists have been successfully using endoscopic resection as a minimally invasive treatment in recent years.1234 However, endoscopic resection with curative intent is indicated only for mucosal invasive tumors because these tumors rarely metastasize to the lymph nodes.5 Therefore, accurate prediction of invasion depth in SESC is crucial for making a proper decision on the treatment strategy.
Endoscopic ultrasonography (EUS) has become the investigation of choice for staging esophageal cancer in terms of both invasion depth and presence or absence of involved lymph nodes.678 Recent reports have suggested that magnifying endoscopic classification based on microvascular morphology can provide a more accurate prediction of tumor invasion depth.9 However, magnifying endoscopes are not available at all institutions and the procedure involves additional costs and time. There are concerns that multiplicity of classifications involving complicated criteria might confuse general endoscopists.9 Moreover, some authors have reported that EUS showed an accuracy of no greater than 70% in the T staging of superficial esophageal cancer.71011 In addition, other authors have reported that there were no statistically significant differences among magnifying endoscopy (ME) with narrow-band imaging (NBI), high-frequency EUS, and high-resolution endoscopy in predicting invasion depth in SESC.1213 The macroscopic classification of superficial neoplasia in the Paris classification may help predict the extent of invasion into the submucosa and thus the choice between endoscopic or surgical treatment, but it is not accurate in predicting submucosal invasion because it reflects only the height, but not the other characteristics, of the lesion.14 To the best of our knowledge, no standard endoscopic criteria for diagnosing SESC have been established to date.
Therefore, we proposed novel endoscopic criteria for predicting invasion depth in SESC and evaluated the diagnostic accuracy and usefulness of the criteria.
METHODS
Patients
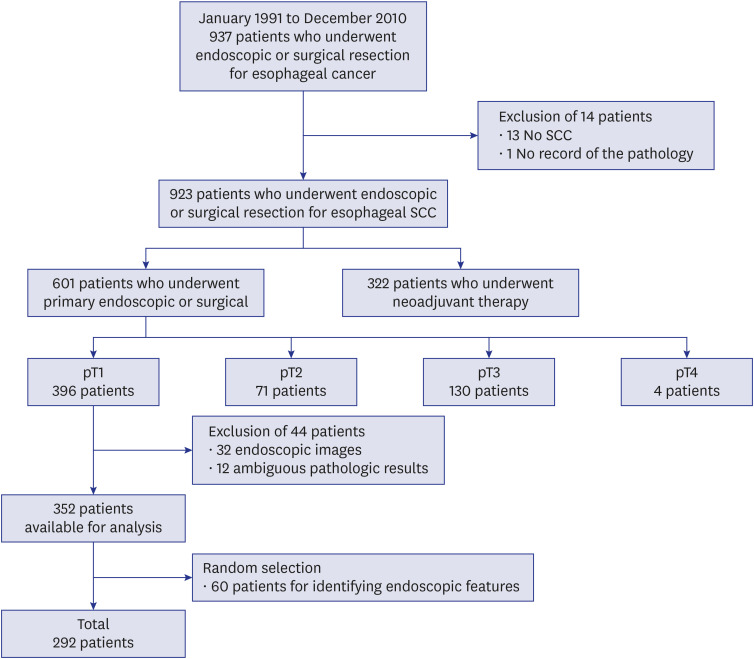
We retrospectively analyzed the data of 939 patients with esophageal cancer who had undergone endoscopic or surgical resection between January 1991 and December 2010 at Asan Medical Center, Seoul, Korea. Of the 939 patients, 396 underwent surgical or endoscopic resection for SESC without preoperative therapy, such as radiotherapy and chemotherapy. Among them, we excluded 44 patients with ambiguous pathologic results or endoscopic images that were inadequate for the prediction of tumor invasion depth. In the absence of standard endoscopic criteria for differentiating between mucosal (T1m) and submucosal (T1sm) cancers, we randomly selected 60 of the 352 patients to identify characteristic endoscopic features of T1m and T1sm cancers and to create the novel endoscopic criteria. The details of 60 randomly selected tumors are shown in Supplementary Table 1. Finally, we analyzed the remaining 292 patients based on the novel criteria (Fig. 1).
Staging workup, treatment, and follow-up
Staging workup included endoscopy with biopsy, EUS, esophagography, and chest computed tomography (CT). In addition, patients with lower esophageal cancer underwent abdominal CT scans. After March 2001, positron emission tomography was routinely included in the staging workup. The endoscopes used in the staging workup were mainly GIF-H260 (Olympus Optical Co, Tokyo, Japan). Endoscopic resection was performed with endoscopic submucosal dissection and surgical resection was performed with a transhiatal, abdominal–right thoracic (Ivor–Lewis) or right thoracic–abdominal–cervical (McKeown) approach. After discharge, all patients entered a follow-up program according to a standard protocol. The endpoint of the oncological outcome was tumor recurrence. For the assessment of recurrence-free survival, recurrence was defined as the development of locoregional recurrence, distant metastasis, or de novo esophageal cancer (metachronous esophageal cancer) after endoscopic or surgical resection. All cases of recurrence were documented pathologically and/or by radiological imaging.
Endoscopic staging
We evaluated macroscopic morphology in accordance with the Japanese criteria15 after reviewing all endoscopic findings. The morphologic classification was published as follows: Type 0 is divided into three categories corresponding to protruding (0–I), nonprotruding and nonexcavated (0–II), and excavated lesions (0–III). Type 0-I is subdivided into pedunculated (0–Ip) and sessile lesions (0–Is). Type 0–II is divided into three subtypes, a, b, and c, corresponding to slightly elevated, flat, and depressed lesions. Type 0–III is an ulcer.
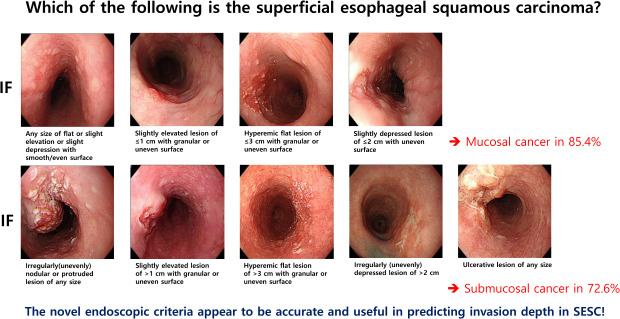
In the absence of standard endoscopic criteria, we identified characteristic endoscopic features such as mucosal elevation/flatness/depression, tumor size, surface regularity and granularity of tumor base, nodularity and protrusion of tumor, and ulceration by reviewing and analyzing the recorded still images in 60 cases of pathologically proven SESC. Then we matched tumor depth by pathologic staging. When the surface was smooth and even, we found that it was more likely to be mucosal cancer than submucosal cancer, regardless of the size. Cases with endoscopic features such as a nodular/protruded or ulcerative lesion seemed like a submucosal cancer regardless of size. By contrast, when the surface was granular or irregular, the tumor depth varied depending on the tumor size and mucosal elevation/flatness/depression. In detail, flat lesions with a granular or uneven surface tended not to invade the submucosal layer even though they are large, whereas elevated or depressed lesions with a granular or uneven surface tended to invade the submucosal layer even though they are small. Therefore, the size of the submucosal invasion was set differently according to elevated, flat, and depressed lesions, and for simplification of clinical application, to 1, 3, and 2 cm, respectively, in these criteria for tumors with a granular or uneven surface. In other words, if the tumor with a granular or uneven surface was more than 1 cm in size for an elevated lesion, 3 cm for a flat lesion, and 2 cm for a depressed lesion, we classified it as a submucosal cancer. Finally, we developed novel endoscopic criteria on the basis of these results (Supplementary Fig. 1).
The novel endoscopic criteria for T staging in SESC were as follows: I. flat or slightly elevated or depressed lesion with smooth/even surface of any size, II. slightly elevated lesion of ≤ 1 cm with granular or uneven surface, III. hyperemic flat lesion of ≤ 3 cm with granular or uneven surface, IV. slightly depressed lesion of ≤ 2 cm with uneven surface for T1m cancer (Fig. 2) and I. irregularly (unevenly) nodular or protruded lesion of any size, II. slightly elevated lesion of > 1 cm with granular or uneven surface, III. hyperemic flat lesion of > 3 cm with granular or uneven surface, IV. irregularly (unevenly) depressed lesion of > 2 cm, V. ulcerative lesion of any size for T1sm cancers (Fig. 3). Using the novel endoscopic criteria, the endoscopic stage was determined based on the consensus of two experienced endoscopists blinded to histologic information. In detail, two endoscopists evaluated the lesions separately on the basis of the novel criteria and discussed the results if these did not match. If the lesions corresponding to different categories co-existed, we classified the lesions into the category that represented deeper invasion depth. Then, we evaluated the diagnostic usefulness of the endoscopic criteria for predicting invasion depth by comparing the endoscopic stages with the histology from the resected specimens.
Fig. 2
Endoscopic criteria proposed for mucosal cancer. (A) flat or slightly elevated or depressed lesion with smooth/even surface of any size, (B) slightly elevated lesion of ≤ 1 cm with granular or uneven surface, (C) hyperemic flat lesion of ≤ 3 cm with granular or uneven surface, (D) slightly depressed lesion of ≤ 2 cm with uneven surface.
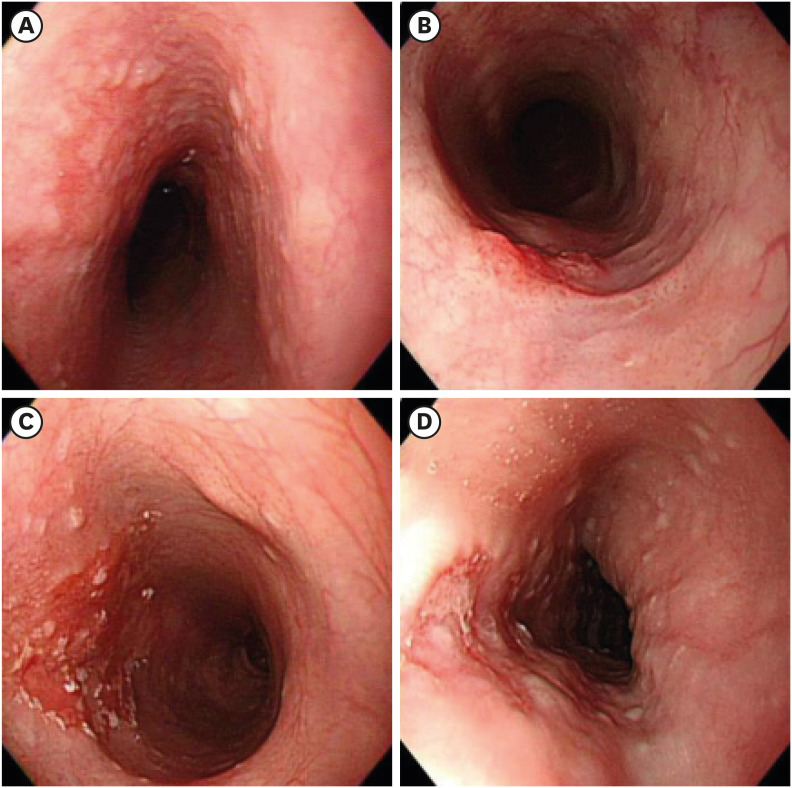
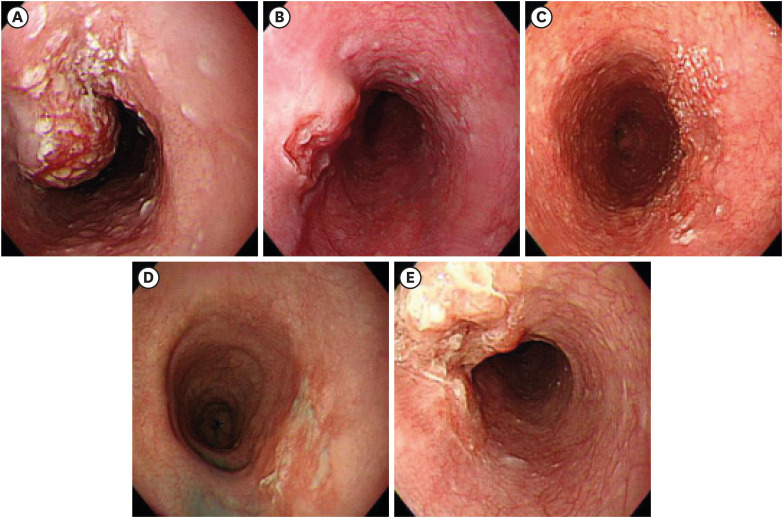
Fig. 3
Endoscopic criteria proposed for submucosal cancer. (A) irregularly (unevenly) nodular or protruded lesion of any size, (B) slightly elevated lesion of > 1 cm with granular or uneven surface, (C) hyperemic flat lesion of > 3 cm with granular or uneven surface, (D) irregularly (unevenly) depressed lesion of > 2 cm, (E) ulcerative lesion of any size.
Histopathology
Histologic examination of the endoscopically or surgically resected tumors was used as a standard to establish the accuracy of the novel endoscopic criteria. The specimens were analyzed using a standard method. All specimens were fixed in 10% formaldehyde, and the tumor and surrounding normal tissues were embedded in paraffin. The endoscopic and surgical specimens were serially sectioned perpendicularly at 2-mm and 5-mm intervals, respectively. Two pathologists with expertise in gastrointestinal cancer and blinded to the endoscopic findings examined the sections. Further, the size of the resected specimens and tumors, invasion depth, and histologic differentiation were evaluated. T1 cancer was further classified as T1m or T1sm, as described previously.16 The degree of differentiation was as recommended by the World Health Organization.17
Statistical analysis
To establish the criteria, some cases were randomly selected using simple random sampling with SPSS. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated using standard definitions. The χ2 test or Fisher's exact test was used to compare categorical variables, and the Mann–Whitney test was used to compare continuous variables. Univariate and multivariate logistic regression analyses were used to identify factors independently associated with the accuracy of endoscopic prediction. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to estimate the effect of variables influencing the accuracy. Oncologic outcomes were calculated using the Kaplan–Meier method and were compared using the log-rank test. A P value of < 0.05 was considered significant. All statistical tests were performed using SPSS versions 18.0 and 20.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
This study was approved by the Institutional Review Board of Asan Medical Center, University of Ulsan College of Medicine (2011-0346). It was a retrospective study using medical records, and personal information protection measures were appropriately established so that the informed consent of the subject was exempted.
RESULTS
Patient characteristics
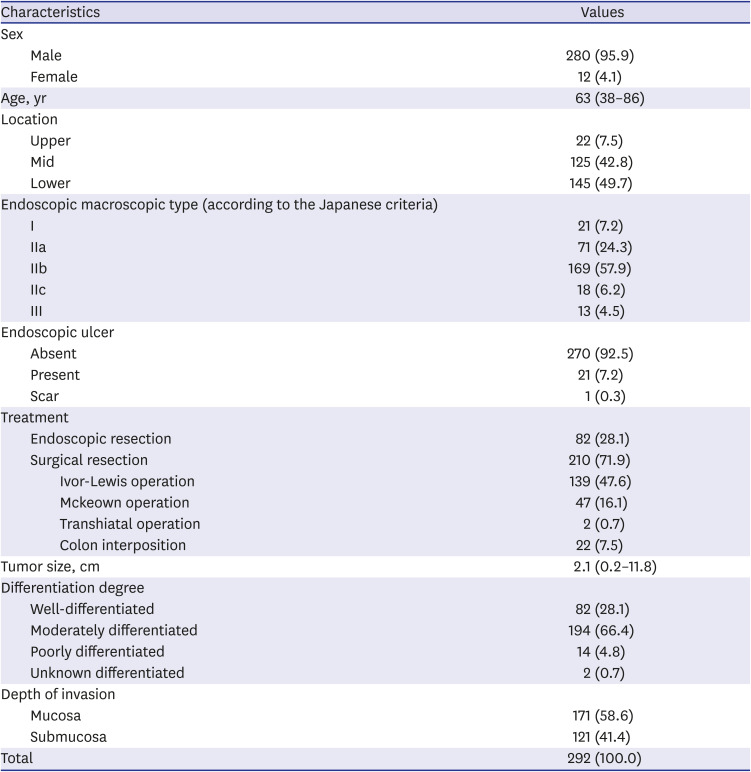
A total of 292 patients (280 men, 12 women; median age 63 years, range 38–86 years) were enrolled in this study. Eighty-two (28.1%) and 210 (71.9%) patients underwent endoscopic resection and surgical resection, respectively. All lesions were squamous cell carcinomas and confirmed as T1 (171 lesions as T1m and 121 lesions as T1sm) on pathology. In detail, six (7.3%) of the 82 patients who underwent endoscopic resection were diagnosed pathologically with T1sm, three of whom had additional treatments (three radiotherapy and one chemoradiotherapy). The median tumor size was 2.1 cm (range, 0.2–11.8 cm), and other clinicopathological characteristics of patients are shown in Table 1.
Table 1
Clinicopathological characteristics of 292 patients with superficial esophageal squamous cell carcinoma
Accuracy of endoscopic staging
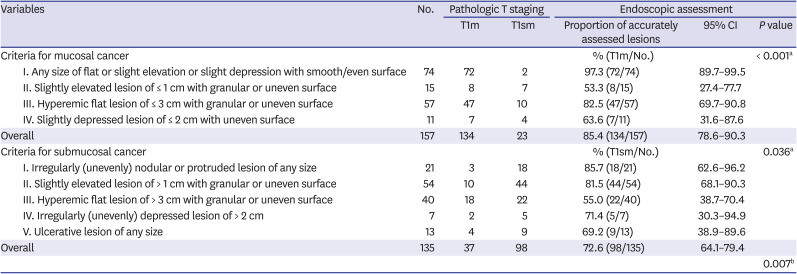
The overall accuracy of T staging based on the novel endoscopic criteria was 79.5% (232/292; 95% CI, 74.3%–83.8%). The relationships between endoscopic staging and pathologic staging of the tumor invasion depth are detailed in Table 2. The sensitivity, specificity, PPV, and NPV for T1m cancers were 78.4%, 81.0%, 85.4%, and 72.6%, respectively, whereas those for T1sm cancers were 81.0%, 78.4%, 72.6%, and 85.4%, respectively. Among these 292 cases, the endoscopic staging of 60 (20.5%) were incorrect: 37 cases (12.7%) were overestimated (staged as T1sm for pathologic T1m cancer) and 23 cases (7.9%) were under-estimated (staged as T1m for pathologic T1sm cancer). The relationship between accuracy and the novel endoscopic criteria was as follows (Table 3): for T1m cancer, a high diagnostic accuracy was observed for lesions of any size that were flat or slightly elevated or depressed (97.3%, 72/74), whereas a low diagnostic accuracy was observed for slightly elevated lesions of < 1 cm in size with granular or uneven surface (53.3%, 8/15). For T1sm cancer, a high diagnostic accuracy was observed for lesions of any size with irregular/nodular protrusions (85.7%, 18/21), whereas a low diagnostic accuracy was observed for hyperemic flat lesions of >3 cm with granular or uneven surface (55.0%, 22/40). All the details of accuracy rates with regard to the novel endoscopic criteria are shown in Table 3.
Table 2
Accuracy rate of the novel endoscopic criteria for T staging

| Stage | Pathologic stage | Accuracy, % | |||
|---|---|---|---|---|---|
| Mucosa | Submucosa | Total | |||
| Endoscopic stage | |||||
| Mucosa | 134 | 23 | 157 | 85.4 | |
| Submucosa | 37 | 98 | 135 | 72.6 | |
| Total | 171 | 121 | 292 | 79.5 | |
Table 3
Accuracy rates according to each item of the novel endoscopic criteria for mucosal and submucosal cancers
Clinicopathological parameters related to the accuracy of the novel endoscopic criteria
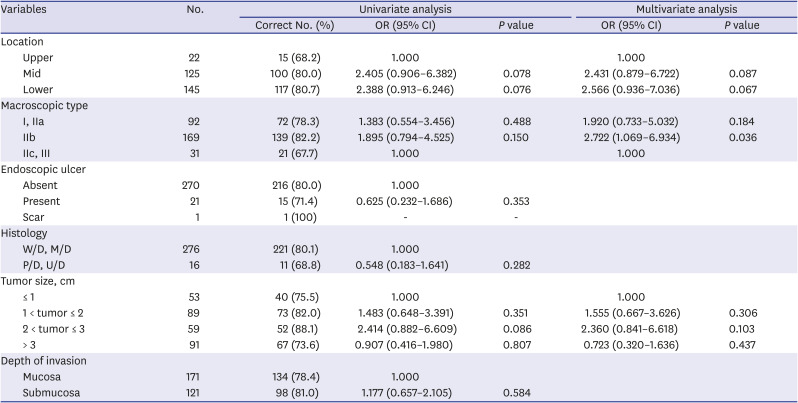
The accuracy of endoscopic staging tended to be higher for lesions located in the mid or lower-third esophagus, macroscopic type IIb lesions, and those with a tumor size between 2 and 3 cm. Multivariate analysis revealed that the variable that affected the accuracy of endoscopic prediction was macroscopic type IIb lesion (OR, 2.722; 95% CI, 1.069–6.934; P = 0.036) (Table 4).
Table 4
Univariate and multivariate analyses of variables affecting the endoscopic prediction accuracy
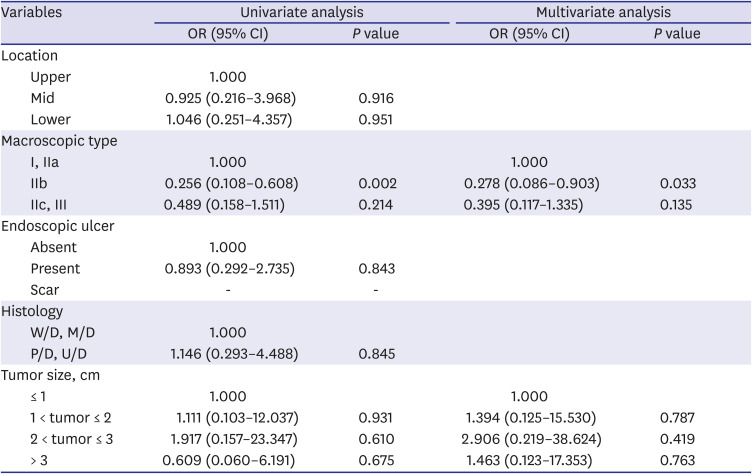
Clinicopathological parameters affecting the accuracy in subgroups diagnosed with mucosal and submucosal cancers on endoscopy
On univariate analysis of 157 patients with endoscopically diagnosed mucosal cancer (M), location of the lesion in the mid or lower-third esophagus and macroscopic type IIb significantly affected the accuracy of endoscopic prediction. Multivariate analysis revealed that macroscopic type IIb lesion (OR, 6.152; 95% CI, 1.525–24.807; P = 0.011) was an independent factor that affected the accuracy of the endoscopic prediction in the M group (Table 5). Univariate analysis for 135 patients with endoscopically diagnosed submucosal cancer (SM) revealed that macroscopic type IIb lesion significantly affected the accuracy of the endoscopic prediction. Multivariate analysis revealed that macroscopic type IIb lesion (OR, 0.278; 95% CI, 0.086–0.903; P = 0.033) had an independent effect on the prediction accuracy in the SM group (Table 6).
Table 5
Univariate and multivariate analyses of variables affecting the endoscopic prediction accuracy in 157 patients with endoscopically diagnosed mucosal cancer
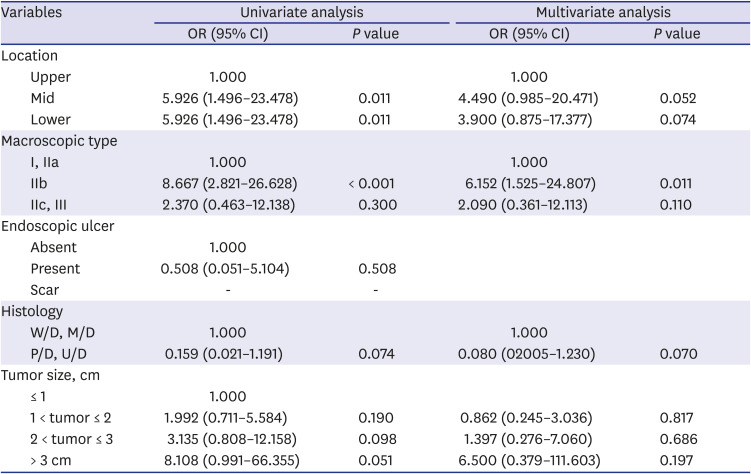
Table 6
Univariate and multivariate analyses of variables affecting the endoscopic prediction accuracy in 135 patients with endoscopically diagnosed submucosal cancer
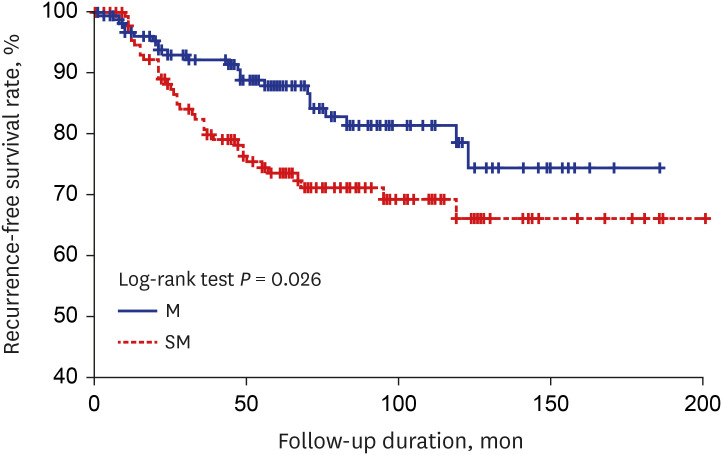
Oncological outcomes according to the novel endoscopic criteria
The median follow-up duration for 292 patients with SESC was 69 months (interquartile range [IQR], 42–106 months). During the follow-up, recurrence was observed in 59 patients (20.2%), 23 (14.6%) of which were in the M group and 36 (26.7%) in the SM group. The risk of recurrence was significantly different between the M and SM groups (hazard ratio [HR] for the SM group was 2.12; 95% CI, 1.18–3.80; P = 0.011). The 5- and 10-year recurrence-free survival rates were 87.8% and 81.3%, respectively, for the M group and 73.7% and 66.4%, respectively, for the SM group; the differences between the two groups were statistically significant (P = 0.026) (Fig. 4).
DISCUSSION
This relatively large-scale study showed that the novel endoscopic criteria using conventional endoscopy alone are useful for predicting invasion depth in SESC. The overall accuracy rate of this criteria was approximately 80%, which is sufficiently accurate for clinical use. In addition, we found that the novel criteria can not only help determine how to treat but also predict clinical outcomes before endoscopic or surgical resection. The Kaplan–Meier curve for recurrence-free survival showed significant differences between the M and SM groups.
Since endoscopic resection has become an established therapeutic option for mucosal cancer, differential diagnosis between mucosal and submucosal cancers in the gastrointestinal tract, especially in the esophagus, has become critical.18 Although EUS has been considered to be the method that most accurately predicts invasion depth in SESC,19 it is associated with several limitations. Conventional EUS systems are not ideal for assessing early neoplastic changes, particularly mucosal and submucosal cancers.13 Recently, EUS using high-frequency catheter probe has played a central role in endoscopic work-up for esophageal cancer staging.1219 However, it is more difficult in the esophagus than in the other portions of the gastrointestinal tract because filling the esophageal lumen with water is often inhibited by esophageal peristalsis, or cardiac/aortic motion prevents taking a fine EUS image.1219 Several recent studies have demonstrated that ME with or without NBI is useful for estimating superficial tumor depth.71218 However, the ME classification of SESC invasion depth, which is based on intrapapillary capillary loop morphological alteration, has never been validated by an independent observer agreement study. Moreover, more advanced equipment such as EUS or ME-NBI are not available at all institutions and operating them requires skill and experience as they are often based on complicated and difficult standards.919 Therefore, they could not be a useful standard for non-experts.
Our study proposed novel endoscopic criteria using conventional endoscopy alone for predicting invasion depth in SESC, and we tried to prove this with many patients. With approximately 300 patients, the present study is currently the largest investigation assessing the value of conventional endoscopy in SESC. Moreover, our criteria are based on relatively simple and objective standards, which can be highly practical and reproducible. We sought to improve the prediction accuracy by reflecting not only on the macroscopic type but also on surface regularity, granularity of the tumor base, and tumor size, although most studies on endoscopic staging of esophageal cancer were conducted using the macroscopic type according to the Paris endoscopic classification or Japanese classification.1315202122 Thus, the novel criteria would help us visually differentiate between mucosal and submucosal invasions of SESC under endoscopy, particularly in medical institutions that do not possess experienced endoscopists or other modalities such as EUS or ME.
Our novel criteria showed sensitivities of 78.4% and 81.0% and specificities of 81.0% and 78.4% for T1m and T1sm, respectively, and an accuracy rate of 79.5% (232/292). The accuracy was also comparable to or higher than previously reported accuracy of other techniques such as EUS, ME, and NBI.81019 In particular, the accuracy of lesions corresponding to the criteria I for T1m cancer (flat or slightly elevated or depressed lesion with smooth/even surface of any size) was very high (72/74, 97.3%). Only two were incorrect. This result suggested that the flat lesions with smooth/even surface were potential candidates for curative treatment by endoscopic resection. Furthermore, the overestimation and underestimation rates were 12.7% (37/292) and 7.9% (23/292), respectively, which were acceptably low. This could be partly explained by the fact that our study included a similar proportion of mucosal (58.6%, 171/292) and submucosal cancers (41.4%, 121/292). The difference in the proportions of mucosal and non-mucosal cancers may account for the higher rate of overestimation and underestimation rates.19
In our criteria for T1sm cancer, hyperemic flat lesion of > 3 cm with granular or uneven surface (criteria III) did not sufficiently predict submucosal invasion. In addition, although not statistically significant, we found that tumors larger than 3 cm tended to be less accurate than smaller lesions in the analysis of the variables that affected the prediction accuracy. Overall, these findings indicate that our endoscopic criteria should be interpreted with caution in relation to tumor size of > 3 cm, and further research is needed to improve the accuracy. On the other hand, macroscopic type IIb lesions were significantly predictive of tumor invasion depth (P = 0.036). In our criteria for T1m cancer, most of the flat or slightly elevated or depressed tumors with smooth/even surface of any size (criteria I) were diagnosed with mucosal cancer and showed high accuracy (97.3%). Therefore, flat lesions can be diagnosed with more confidence using our criteria. However, further studies with more detailed endoscopic findings suggesting submucosal invasion in the flat lesions are required to identify lesions that require curative surgical esophagectomy.
Our study has some limitations. First, in this study, endoscopic staging was determined based on the consensus between two experienced endoscopists. Therefore, if an endoscopist with less experience determines the invasion depth alone, the accuracy rate may be reduced. Second, endoscopic staging was retrospectively performed using still images, whereas in clinical practice, this is likely to be performed by viewing moving images in dynamic situations. These limitations indicated that additional studies involving non-experts are required to determine the true diagnostic accuracy of endoscopic staging. Third, this endoscopic staging was not developed strictly according to the statistical data due to small sample size. Therefore, another validation cohort will be required. Fourth, because we have not obtained information about LN metastasis based on surgical cases, whether ESD can be indicated with these criteria alone is difficult to clearly determine. Therefore, a further validation study based on data containing information about LN metastasis is needed. Finally, because the data of recurrence-free survival involved many selection biases such as treatment modality, a decision on additional treatment, and lymphovascular invasion, care should be taken when predicting the clinical outcomes.
In conclusion, conventional endoscopy provides reliable accuracy for predicting tumor invasion depth in SESC. Careful endoscopic examination with the novel endoscopic criteria for SESC can help decide the best treatment strategy between endoscopic and surgical resection. Furthermore, it might also help provide useful information about oncologic outcomes.
 XML Download
XML Download