

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Idiopathic inflammatory myopathies (IIM) are a group of rare autoimmune rheumatic disease that primarily induces chronic inflammation of skeletal muscles, leading to proximal muscle weakness and disability. Patients with IIM generally receive high dose systemic glucocorticoids in combination with antimalarial agents or conventional non-targeting immunosuppressive,1 but the management of IIM remains challenging for clinicians.
Patients with IIM often experience extensive muscular inflammation, causing difficulty in swallowing, voiding, and deterioration of performing activities of daily living. Life-threatening extra-muscular complications, including interstitial lung disease (ILD), are also prevalent. However, a considerable portion of patients inadequately responds to the current treatment options. Owing to the rarity and heterogeneity of IIM, clinical trials and evidence for guidelines are also insufficient, and the 10-year mortality was still high in recent studies (14%–38%).23 Although interest in biologic agents that directly target the immune cells or cytokines has increased in other systemic rheumatic disease following advances in the understanding of the immunopathogenesis, studies that have investigated the efficacy and safety of biologic agents in patients with IIM are limited.4
Rituximab (RTX) is a monoclonal antibody that selectively binds to CD20+ B cells.5 RTX was originally developed for the treatment of lymphoproliferative diseases,6 but it is also approved for the treatment of rheumatoid arthritis,7 pemphigus vulgaris,8 granulomatosis with polyangiitis (GPA), and microscopic polyangiitis (MPA).9 In addition, it is used widely to manage a variety of immune-related disorders, including idiopathic thrombocytopenic purpura,10 systemic lupus erythematosus,1112 and multiple sclerosis.13 In terms of IIM, RTX also has been believed to be a potential therapeutic option along with the B cell infiltration in the muscles of patients with IIM and myositis-associated antibodies (MAA).114 RTX showed favorable outcomes in patients with refractory IIM who failed to respond to corticosteroid and conventional immunosuppressive agents, but most studies were case series and open label studies. In Korea, a case series described four patients with refractory IIM treated with RTX and all patients responded to IIM.15 Therefore, this paper aimed to identify the efficacy and safety of RTX for patients with refractory IIM.
METHODS
Study population
We conducted a retrospective multicenter study of 16 patients with refractory IIM who were treated with RTX from July 2006 to October 2017. This multicenter retrospective study comprised patients from seven tertiary rheumatology clinics that had obtained official endorsement for the use of RTX for refractory IIM from the Ministry of Health and Welfare and the Health Insurance Review & Assessment Service (HIRA). Off-label RTX use must be officially allowed by each hospital after receiving institutional review board approval and submission to the HIRA, because RTX currently is not approved by the Korean Ministry of Food and Drug Safety (MFDS) for the treatment of IIMs.
The medical records of patients with a diagnosis of possible or definite IIM according to Bohan and Peter's criteria1617 and treated with RTX were respectively reviewed. Patients with a shorter than 6 months' observation period (from RTX administration to the data collection), whose age at diagnosis of IIM was less 16 years of age, and patients with malignancy were excluded. RTX was prescribed by expert rheumatologists due to an inadequate response or intolerance to corticosteroids and conventional immunosuppressive therapy. All patients received RTX intravenously, and the RTX dosing and cycle differed depending on the decision of the rheumatologist.
Patient assessment and response criteria
Demographic characteristics, including age (years), sex (female/male), height (cm), and weight (kilograms) were recorded. Disease-specific variables, including IIM duration, concomitant and cumulative immunosuppressive agent history, IIM activity, the reason for RTX administration, and RTX dose and interval, were also assessed at the time of RTX administration. The IIM activity was measured by muscle weakness (grade), extra-muscular symptoms (skin rash, skin necrosis, dysphagia, dyspnea, Raynaud phenomenon, and ILD), constitutional symptoms (fever, fatigue, and weight loss), and laboratory markers including muscle enzymes levels (serum creatine phosphokinase [CPK], lactate dehydrogenase [LDH], aldolase, aspartate aminotransferase [AST], alanine transaminase [ALT]), complete blood count, erythrocyte sedimentation rate (ESR), and C reactive protein (CRP). IIM activity was assessed in each hospital and at baseline and followed up at the regular clinical visit schedule (2- or 4-week intervals). The reference ranges and units for laboratory markers were similar among the 7 rheumatology clinics.
We assessed the efficacy of RTX based on the serum CPK level, daily dose of corticosteroid and opinion of the physician.18 A decrease in CPK level and daily corticosteroid dose was considered to be significant if it was > 25% of the baseline. The physician's opinion on the response was dichotomized to “response” or “no response.” Complete response (CR) and partial response (PR) were defined as a patient meeting all three or only two efficacy criteria, respectively. Three patients were administered a second cycle of RTX after completion of the first cycle of RTX administration but the response was assessed based on the first cycle of RTX administration.
Statistical analysis
The general statistics of the study population are presented medians (first interquartile, third interquartile) for continuous variables, and frequencies with percentage (%) for categorical variables. Demographic and clinical characteristics were compared by using Fisher's exact test (binary variables) and the Mann-Whitney U test (linear variables). All statistical analyses were conducted using IBM SPSS version 25.0 (IBM Corp., Armonk, NY, USA). P values of < 0.05 (two-tailed) were considered statistically significant.
Ethics statement
This study was approved by the institutional review board (IRB) of each hospital and the requirement for informed consent was waived because of the retrospective nature of the study (IRB No. HYUH 2018-01-020-002 in Hanyang University Hospital, AJIRB-MED-OBS-17-509 in Ajou University Hospital, 2018-0567 in Asan Medical Center, 2018-0541-001 in Severance Hospital, Yonsei University Health System, 2018-02-027 in Chungnam National University Hospital, KUH1010916 in Konkuk University Medical Center, CNUH-2018-058 in Chonnam National University Hospital).
RESULTS
Demographic and clinical characteristics
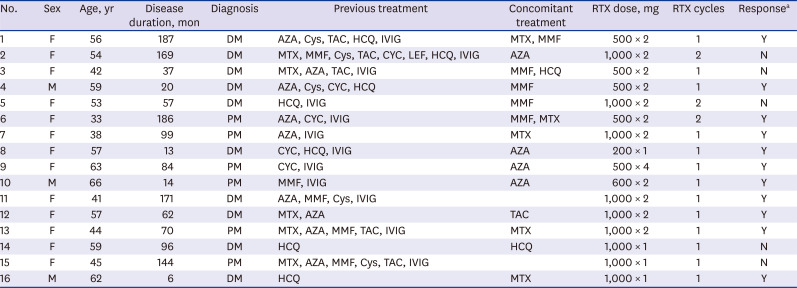
The baseline demographic and clinical characteristics are presented in Table 1. Ten patients with dermatomyositis and six patients with polymyositis were treated with RTX. Thirteen (81.3%) were female, the median age at RTX treatment was 51.8 (42.5–59.0) years of age, and the median IIM disease duration (from IIM diagnosis to RTX treatment) was 88.4 (24.3–162.8) months. All patients had insufficient response or intolerance to at least one (median, 3.6 [2.0–5.0]) conventional immunosuppressive agent: azathioprine, n = 12, 75.0%; methotrexate, n = 11, 68.8%; mycophenolate mofetil, n = 10, 63.0%; hydroxychloroquine, n = 8, 50.0%; cyclosporine, n = 5, 31.3%; cyclophosphamide, n = 5, 31.3%; tacrolimus, n = 5, 31.3%; leflunomide, n = 1, 6.3%). Twelve (75.0%) patients had received intravenous immunoglobulin therapy.
Table 1
Clinical characteristics of 16 patients with idiopathic inflammatory myopathies treated with RTX
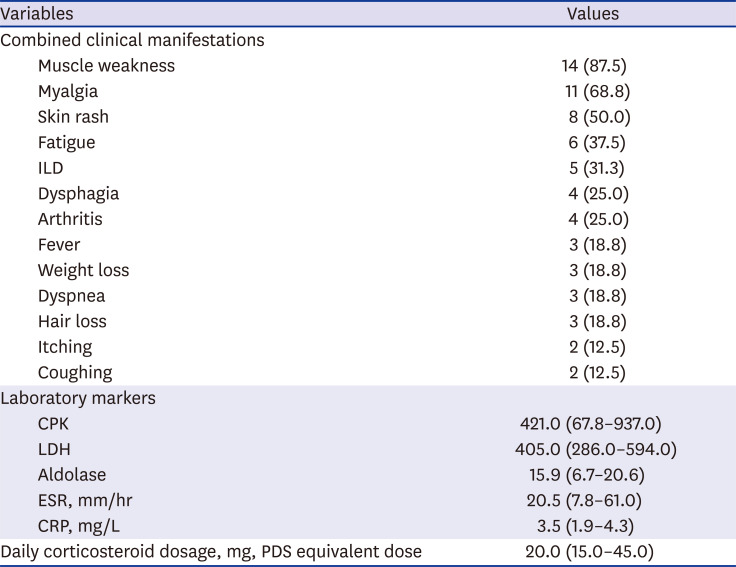
IIM activity at the time of RTX treatment is summarized in Table 2. Most patients (n = 14, 87.5%) experienced muscle weakness and all patients had at least one extra-muscular manifestation (dermatomyositis specific skin rash, n = 8, 50.0%; ILD, n = 5, 31.3%; dysphagia, n = 4, 25.0%; arthritis, n = 4, 25%). Eight (50%) patients had constitutional manifestations, such as fatigue (n = 6, 37.5%), fever (n = 3, 18.8%), and weight loss (n = 3, 18.8%). The median serum CPK level was 421.0 (67.8–937.0) unit/L and the median corticosteroid dose was 20.0 (15.0–45.0) mg (prednisone equivalent dose) (Table 2).
Table 2
Myositis activity at the time of rituximab treatment
RTX administration and treatment response
Six (37.5%) patients received two doses of 1,000 mg RTX 2 weeks apart (total 2 g), 4 (25.0%) patients received two doses of 500 mg RTX 2 weeks apart (total 1 g), 3 (18.8%) patients received a single dose of 1,000 mg, one patient received 500 mg weekly for a total of four doses (total 2 g), 1 patient received 600 mg RTX 2 weeks apart (total 1.2 g), and one patient received a single dose of 200 mg RTX (Table 1).
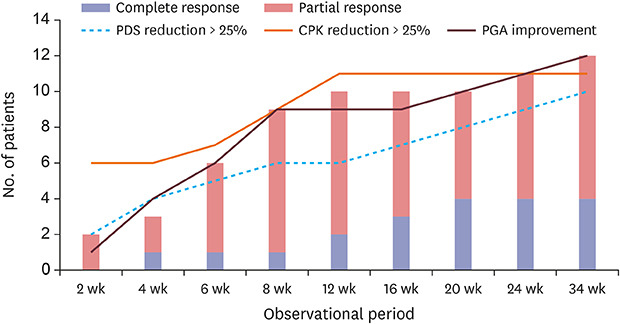
The response rate to RTX treatment is shown in Fig. 1. At 12 weeks after RTX treatment, 11 (68.8%) and 9 (56.3%) patients achieved a 25% reduction in CPK and daily corticosteroid, respectively, and 6 (37.5%) patients showed improved physician's global assessment (PGA). CR and PR were achieved by 2 and 6 patients, respectively, and the overall response rate was 62.5% (10 patients).
Fig. 1
Response rate of RTX treatment.
CPK = creatine phosphokinase, PGA = physician's global assessment, PDS = prednisolone, RTX = rituximab.
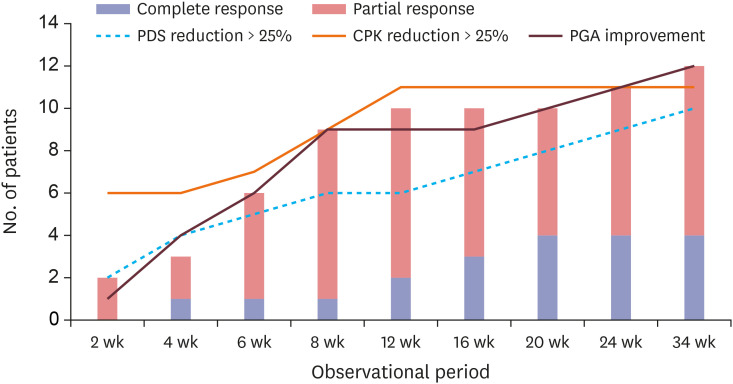
At 24 weeks after RTX treatment, 11 (68.8%) patients achieved a 25% reduction in corticosteroid dose and CPK levels and 9 (56.3%) showed improved PGA. CR was achieved by 4 (25.0%) patients, and the overall response rate was 68.8% (11 patients). The median serum CPK level decreased from 421.5 (67.8–973.0) to 42.0 (interquartile range [IQR], 15.5–222.0) and the median dose of corticosteroid decreased from 20 mg/day (IQR, 15–45.0) to 13.8 mg (IQR, 10.6–15.2). At the end of follow-up (median 24 weeks, range 24–68 weeks), the overall response was 12 (75.0%) patients: 4 (25.0%) and 8 (50.0%) patients achieved CR and PR, respectively.
Three patients were re-administered RTX after completion of the first cycle of RTX administration (at intervals of 27, 30, and 52 weeks) when IIM relapsed or was clinically indicated. Two patients were assessed to have no response in both the first and second cycles.
Factors associated with response to RTX treatment
A comparison between responders and non-responders at 24 weeks after RTX treatment is shown in Table 3. Baseline median muscle enzyme levels were higher in responders than non-responders: serum CPK, 692.0 vs. 64.0, P = 0.013; LDH, 530.0 vs. 286.0, P = 0.013; and aldolase, 18.1 vs. 6.7, P = 0.013. All patients with baseline serum CPK over 400 responded to treatment, but 2 out of 3 patients with CPK between 100 and 400, and only 1 out of 5 patients with CPK below 100 responded to RTX treatment. However, all other demographic and clinical characteristics, including patient age, sex, disease subtype, disease duration, RTX dose, ESR, and serum CRP, were not significantly different between the two groups.
Table 3
Comparison between responders and non-responders at 24 weeks after RTX treatment
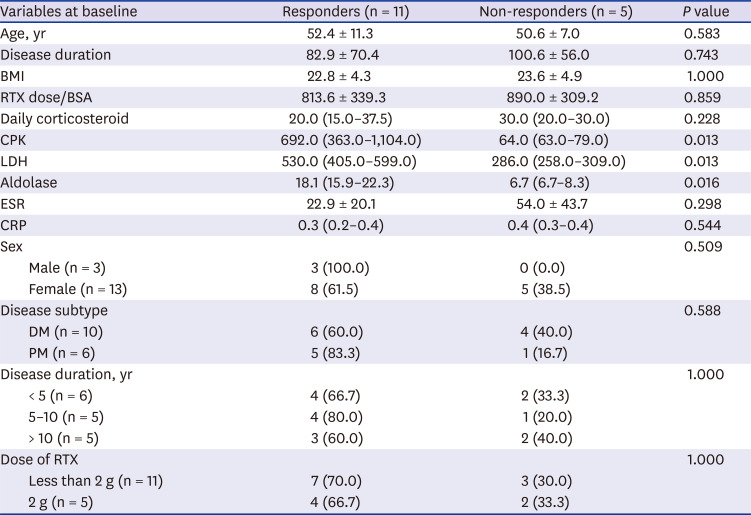
Values are given as mean (standard deviation), median (interquartile rage) or number (%).
Normality was tested using Shapiro-Wilk normality test.
RTX = rituximab, BMI = body mass index, BSA = body surface area, CPK = creatine phosphokinase, LDH = lactate dehydrogenase, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, DM = cermatomyositis, PM = polymyositis.
We investigated autoantibody patterns and treatment response. Of the 16 patients, 10 patients tested ANA at the time of RTX administration, and ANA was detected in 6 patients. The speckled pattern was the most common ANA pattern (4 out of 6 patients), followed by mixed and cytoplasmic patterns (1 patient each). All the 6 ANA–positive patients responded to RTX treatment (including all the 4 cases of CR), while only 2 cases achieved PR and the other 2 cases did not respond to RTX treatment among the 4 ANA-negative patients. Anti Jo-1 antibody was tested for in 3 patients and detected in 2 patients. All the 3 patients who tested positive for anti Jo-1 antibody achieved CR.
DISCUSSION
In this multicenter study, RTX was effective in 75% of patients (12/16) at a median of 24 weeks after treatment for patients with refractory IIM who had responded poorly to conventional immunosuppressant treatment. The serum CPK level and daily dose of corticosteroid decreased significantly compared with the baseline after RTX in most patients, suggesting the clinical efficacy and safety of RTX in patients with refractory IIM.
Since the first classification criteria and 5 subsets for IIM were provided by Bohan and Peter17 in 1975, extended understanding and more clinical subsets of IIM have been suggested. However, unlike the simple terminology “myopathy,” neither the pathophysiology nor phenotype of patients with IIM are straightforward. It is important to note that the diagnosis of IIM may be challenging, as the diagnosis of IIM should be made circumspectly after the exclusion of a variety of diseases that mimic IIM.1920 Patient assessment also is complicated. The pattern and severity of organ involvement is highly heterogeneous in each patient, and an objective measurement of muscular and extra-muscular involvement is complex. Given the rarity and heterogeneity of IIM,192021 outcome measure and response criteria have been available only in recent years, and evidence level for IIM treatment strategy is low. Unfortunately, a meaningful portion of patients with IIM responds incompletely to conventional immunosuppressive agents; therefore, patients with refractory IIM may be subjected to therapeutic strategies that have not been sufficiently investigated.
RTX, a selective CD20+ B lymphocyte-depleting agent, is a potential therapeutic option for the IIM treatment with evidence of prominent B lymphocyte infiltration in the muscles of patients with IIM. Infiltration of cytotoxic CD8+ T lymphocytes at the endomysium and/or that of B lymphocytes accompanied by CD4+ T lymphocytes at perivascular sites are the pathologic hallmark of IIM.2223 Although earlier studies suggested that B lymphocytes were considered to be more important in dermatomyositis than in polymyositis,2425 subsequent studies identified the presence of plasma cells and immunoglobulin-transcribing genes in the endomysium of patients with polymyositis and inclusion body myositis.26
The strong association between MAA and clinical phenotype also supports the critical role of B lymphocytes in the pathophysiology of IIM. Antisynthetase syndrome (ASS) is a well-known subtype of IIM, characterized by a progressive disease course with severe ILD, mechanic's hand, a distinct histological pattern on muscle tissue, and ASS-specific autoantibodies, such as anti-Jo-1 antibody.27 Immune-mediated necrotizing myopathy (IMNM) is another particular subtype of IIM, associated with necrosis of microfibers without inflammatory cell infiltrates and IMNM-specific antibodies, including anti-3-hydroxy-3-methylglutaryl CoA reductase antibody and anti-signal recognition protein antibody.282930 Anti-melanoma differentiation–associated gene 5 (MDA5) antibody is a novel and specific antibody associated with amyopathic dermatomyositis with rapidly progressive ILD.3132 Anti-transcription intermediary factor 1γ antibody and the NM fragment of anti-nuclear matrix protein antibody have been described as related to cancer-associated myositis.333435
Thus, evidence has started to accumulate regarding the efficacy of RTX in the management of IIM. A number of case series and small open-label trials have been published, and the majority of the studies have described patients with refractory and/or life-threatening IIM. There also is a completed randomized, double-blinded, controlled clinical trial in patients with IIM (the RTX in myositis [RIM] trial).36 In total, 195 definite or probable patients with dermatomyositis or polymyositis or juvenile patients with dermatomyositis with poor response to glucocorticoids and at least one immunosuppressive agent were included in the RIM trial. Patients were randomly assigned to receive RTX at baseline (RTX early group) or 8 weeks later (RTX late group), and the time to achieving the International Myositis Assessment and Clinical Studies (IMACS) definition of improvement was compared between the two groups.37 At the end of the study (44 weeks after RTX treatment), 82.6% (161/195) of the patients met the definition of improvement although early and late treatment of RTX showed no significant differences for the primary and secondary end points.
It also is important to emphasize that previous reports show a considerable association between the clinical response and presence of MAA. The efficacy of RTX in patients with refractory ASS has been reported.38 Levine et al.39 reported that patients with the anti-Jo-1 antibody had a greater improvement in lung function after RTX treatment, and one recent study reported that the serum titer of MAA decreased after B cell depletion and was correlated with changes in disease activity.40 Aggarwal et al.41 evaluated predictors for the response to RTX from the RIM trial, and revealed that presence of MAA and less IIM-associated damage were associated with good prognosis and rapid clinical improvement. In this present study, we also revealed that ANA-positivity was associated with better clinical response to RTX treatment: all the 4 cases of CR were ANA–positive, while among the 4 ANA-negative patients, 2 cases achieved PR and the other 2 cases did not respond to RTX treatment.
When comparing responders and non-responders, ESR and serum CRP levels tended to be higher in non-responders (although not statistically significantly), despite the lower CPK levels in non-responders. This could be associated with the fact that the improvement in extra-muscular involvement was not fully reflected in the current response criteria. There were 2 patients who received RTX due to acute aggravation of organizing pneumonia, with normal serum CPK level (64 unit/dL and 79 unit/dL, respectively) and high ESR (116 mm/hr and 64 mm/hr, respectively). Unlike previous studies4243 which reported especially favorable responses to pulmonary involvement, the 2 patients mentioned above with organizing pneumonia did not fully recover after RTX treatment, and they did not achieve CPK reduction nor by their physician's opinion. Contrarily, one patient with generalized and refractory skin lesions with normal serum CPK (32 unit/dL), CRP (0.15 mg/dL) and ESR levels (18 mm/hr) had almost fully recovered after RTX treatment and was classified as a responder. With the brief response criteria in this study, the data regarding extra-muscular lesions were simply handled by ‘physician's global assessment’, and further studies should apply a standardized assessment protocol for extra-muscular involvement such as the 2016 ACR-EULAR response criteria.44
Most of the patients did not receive additional immunosuppressive agents during the observational period except one patient who started MTX 6 weeks after RTX administration. Our data reveals that the long-term clinical efficacy of RTX may persist, which is similar to previous studies,45 whereas reconstitution of peripheral blood B cell lineage occurs within a few months.46
Although this study describes the clinical efficacy of RTX in patients with refractory IIM, our study differs from the RIM trial as RTX is not approved for use in Korean patients with IIM and our study is based on real-world data. Participants in our study were older (median, 51.8 years of age) with a longer disease duration (median, 7.4 years) than those in the RIM trial (mean age early forties, mean disease duration 5.3 years). However, the ratio of female participants (81%), the number of previous immunosuppressive agents administered prior to RTX treatment (median, 3.6), and the daily corticosteroid dose at RTX administration (median, 20.0 mg) were similar to that of the RIM trial (71% female patients, mean 3.1 immunosuppressive agents, approximately 20 mg of daily corticosteroid). The dosing regimen for RTX in IIM was also different. In the RIM trial, the dose of RTX used (total 2 g, as 2 × 1 g infusions) was the same as the FDA-approved dose for RA, GPA, and MPA.
The safety of RTX should also be discussed. We observed only one infection, and no SAE or infusion reaction occurred in this study; the rate of AEs in this study is lower than that of other studies. In a study that analyzed the efficacy and safety of RTX in Korean patients with active lupus nephritis, four out of 39 patients experienced an infusion reaction and three patients had an infection.12 In the RIM trial, there were 67 SAEs in 64 patients, and the RTX group showed significantly more infusion reactions than the placebo group. This underestimation of AE/SAEs may be related to the RTX dose, which was lower than that of other studies (less than half the patients received a total of 2 g RTX) and the collection of AE/SAEs by retrospective chart review.
The relatively small number of study populations, lack of long term outcome and repeated treatment, incompletion of the autoantibody data and the lack of MAA and immunological data including B lymphocyte count are the limitations of our study.
Despite these limitations, it can be concluded that RTX is an effective and safe therapeutic option in patients with refractory IIM who have responded poorly to conventional treatment. We believe that this study adds to the current knowledge of RTX in patients with IIM. Further prospective studies in Korean patients with IIM are required to provide a rationale for the application of RTX in patients with refractory IIM.
 XML Download
XML Download