

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Suicide is a major cause of death,1 with the ever increasing number of deaths due to suicide reaching more than 800,000 worldwide each year.2 Suicide attempts occur about 20-fold more often than deaths due to suicide.3 In the United States, the average annual number of emergency department visits for suicide attempts and self-inflicted injury is 538,000.4 A history of previous suicide attempts is the most powerful predictor for suicide attempts or death due to suicide.56
The emergency department is the most common contact point providing management and prevention interventions for suicide attempt patients.7 Previous research has focused on developing effective interventions for patients who have visited the emergency department after attempting suicide. Several randomized controlled trials have suggested several types of interventions, such as active contact and follow-up, psychotherapy, and pharmacotherapy.8910 A recent meta-analysis showed that, among several types of interventions, community-based active contact and follow-up is most effective in reducing the risk of repeat suicide attempts among individuals who visit the emergency department after attempting suicide.11
Nevertheless, according to previous research, patients visiting the emergency department after attempting suicide have complained that suicide prevention interventions are insufficient or completely absent.121314 Thus, there has been a continuous demand to improve suicide prevention interventions in emergency departments and for the collaboration between emergency departments and community-based mental healthcare centers that enable ongoing community-based care.7
Previous research has also suggested that systematic collaborations between hospitals and aftercare providers should operate to increase the long-term maintenance of continuity of care for individuals who have attempted suicide in the past.15 However, there have been few studies investigating which factors influence collaborations between emergency departments and community-based mental healthcare centers. Therefore, we evaluated factors affecting collaborative efforts between an emergency department and community-based mental healthcare centers in the management of patients who have attempted suicide.
METHODS
Study sample
This study was conducted in the emergency department and suicide prevention center of an 843-bed, medical college-affiliated, tertiary referral hospital located in Incheon, Korea. Incheon is the third largest municipality in the Seoul Metropolitan Area, with a population of 2.95 million. In 2018, 60,570 people visited the emergency room of this hospital, and 11,988 (19.8%) were admitted, among whom 2,142 (3.5%) were admitted to the intensive care unit.
The hospital's suicide prevention center was opened in May 2017. All patients visiting the emergency department after a suicide attempt are registered in the hospital's suicide prevention center. The center offers a hospital-based psychological counseling program to registered patients. The program is led by a psychologist. The program consists of three counseling sessions during hospitalization and one counseling session after discharge. The length of counseling session during hospitalization is about 40 to 60 minutes, and the length of the counseling session after discharge is about 90 minutes. The first counseling session focuses on building rapport, the second and third counseling sessions focus on the causes of suicide attempt and their solutions. The final counseling session is designed to help a patient address a particular problem, such as stress management or alcohol addiction. The center also provides out-of-pocket expenses for patients deemed necessary for economic support.
Study design
This was a retrospective study of data obtained from participants' medical records and counseling records. The study was conducted over a period of 24 months, from May 1, 2017 to April 30, 2019. The inclusion criteria were patients visiting the emergency department after a suicide attempt. Patients who met the following criteria were excluded: patients who were dead on arrival, patients who were transferred to another hospital for patient-level reasons, patients who were transferred to the psychiatric hospital because of clinical conditions that did not require medical treatment, patients who died before scheduled medical care and psychiatric treatment, patients who were lost to follow-up during treatment in the emergency department, and patients with missing data. Owing to the cross-sectional study design, we included only data from the first visit for patients who visited multiple times within the study period, regardless of the number of visits.
We set the collaboration between the emergency department and a community-based mental healthcare center as the dependent variable in our analysis. Collaboration between the emergency department and a community-based mental healthcare center was defined as a case in which both of the following conditions were satisfied: 1) the information about patients who attempted suicide was communicated to a community-based mental healthcare center after the completion of scheduled medical treatment, psychiatric treatment, and psychological counseling and 2) face-to-face psychological counseling in a community-based mental healthcare center was performed at least twice.
The independent variables were clinical factors, psychiatric factors, and factors related to socioeconomic status. Clinical factors included gender, age, initial vital signs, initial severity, and history of chronic disease. We evaluated the initial severity using the Korean Triage and Acuity Scale (KTAS) score.16 History of chronic disease was defined as whether there was a disease that required a visit to the hospital at least once every 3 months. However, psychiatric disease was excluded from the definition of chronic disease.
Psychiatric factors included history of mental disorders, history of previous suicide attempts, history of psychiatric hospitalization, suicide attempts associated with mental disorders, suicide attempts associated with interpersonal relationships, suicide attempts associated with economic difficulties, suicide attempts associated with physical illness, preplanned suicide attempts, method of suicide attempt, place of suicide attempt, alcohol consumption status at the time of suicide attempt, sustained suicidal ideation after suicide attempt, insight about the suicide attempt after the suicide attempt, and completion of hospital-based psychological counseling. The causes of suicide attempts were defined based on psychiatric records. Suicide attempt methods were defined as either poisoning or other violent behavior. The place of suicide attempt was defined as either home or “other.” Alcohol consumption status at the time of the suicide attempt was defined as either drunk or not on the basis of participants' statement. Completion of hospital-based psychological counseling was defined as having completed all four counseling sessions within a month after the suicide attempt.
Socioeconomic factors included monthly income, education level, marital status, employment status, health insurance status, type of residence, and economic support. Monthly income was defined as either above or below USD 1,250 (median income of single-person households in Korea as of 2017), based on the psychological counseling record. Educational level was defined based on whether participants graduated from college or not. Health insurance status was defined based on whether or not participants were insured with national health insurance scheme. Type of residence was defined according to whether participants lived with someone or lived alone. Economic support was defined according to whether out-of-pocket expenses had been supported or not.
Statistical analysis
Statistical analyses were performed with SPSS Statistics for Windows, Version 18.0 (IBM Corp., Armonk, NY, USA). Patients were divided into two groups, the failed group and the successful group, based on the failure or success of the collaboration between the emergency department and community-based mental healthcare centers. Previously collected patient data were analyzed for differences in basic characteristics using the χ2 test, independent samples t-test, and Mann-Whitney U test. We performed logistic regression analyses of characteristics that significantly differed between the groups to identify factors influencing collaboration between the emergency department and community-based mental healthcare centers. Statistical significance was defined when P values were less than 0.05.
Ethics statement
The data collected were used for study purposes only. This study was approved by the Institutional Review Board of the Catholic University of Korea Catholic Medical Center, where the study was conducted (approval No. OC18RESI0089). Informed consent was waived since we used retrospective de-identified data.
RESULTS
A total of 743 patients visited the emergency department after a suicide attempt within the study period. Of these, 674 patients were enrolled, after excluding 42 patients who were dead on arrival, four patients who were transferred to a lower level general hospital for patient-level reasons, 13 patients who were immediately transferred to the psychiatric hospital because of clinical conditions that did not require medical treatment, eight patients who died before scheduled medical care and psychiatric treatment, and two patients who were lost to follow-up during treatment in the emergency department. No patient was excluded because of missing data.
Of the 674 enrolled patients, 153 (22.7%) patients were successfully managed via collaboration between the emergency department and a community-based mental healthcare center and were categorized in successful group; the remaining 571 patients made up the failed group. There were 144 (21.4%) patients admitted to the intensive care unit, including six patients who needed emergency surgery. There were 152 (22.6%) patients admitted to the general ward; 197 (29.2%) patients were discharged from emergency department on the day of presentation. The remaining 181 (26.9%) patients were self-discharged against medical advice during medical and psychiatric treatment.
Clinical factors of patients in the successful and failed groups were as follows (Table 1). Mean KTAS score was significantly higher in the successful group than in the failed group. There were significantly more self-discharges against medical advice in the successful group than the failed group. Other factors, such as gender, age, initial vital signs, and history of chronic disease did not significantly differ between the groups.
Table 1
Characteristics of the failed and successful collaboration groups

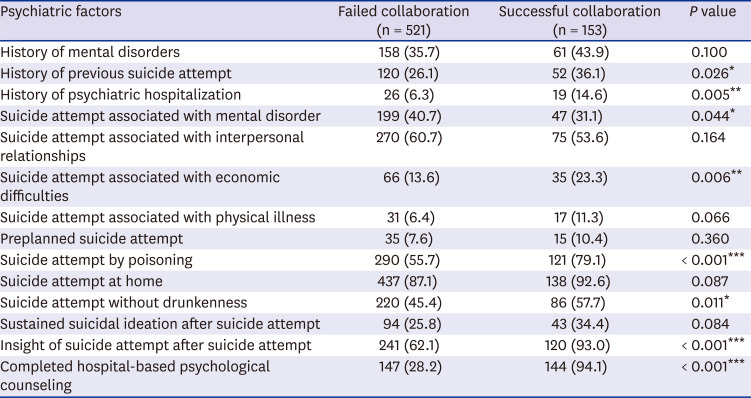
Psychiatric factors in the failed and successful groups are summarized in Table 2. The successful group had significantly more patients with a history of previous suicide attempts and psychiatric hospitalization. Suicide attempts associated with mental disorders were more common in the failed group, and suicide attempts associated with economic difficulties showed more in the successful group. In the successful group, the proportions of suicide attempts by poisoning and suicide attempt without alcohol associated intoxication were significantly higher than the failed group. There were significantly more patients who had insight of their suicide attempts after the fact and more patients who completed hospital-based psychological counseling in the successful group. Other factors did not significantly differ between the groups.
Table 2
Psychiatric factors of the failed and successful collaboration groups
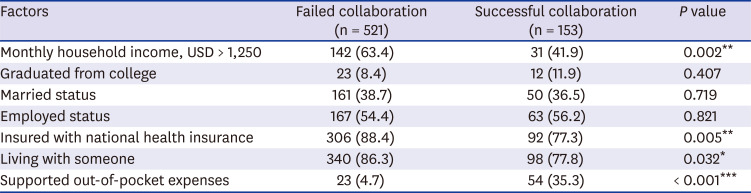
The factors associated with socioeconomic status in the failed and successful groups were as follows (Table 3). In the successful group, the number of patients who had monthly household incomes USD > 1,250 and patients who were supported by out-of-pocket expenses was significantly higher than the failed group. On the other hand, the number of patients who were married and who were living with someone else was significantly higher in the failed group. Other factors did not significantly differ between the groups.
Table 3
Factors associated with socioeconomic status in the failed and successful collaboration groups
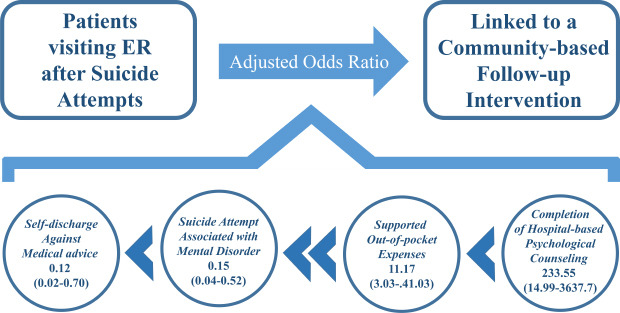
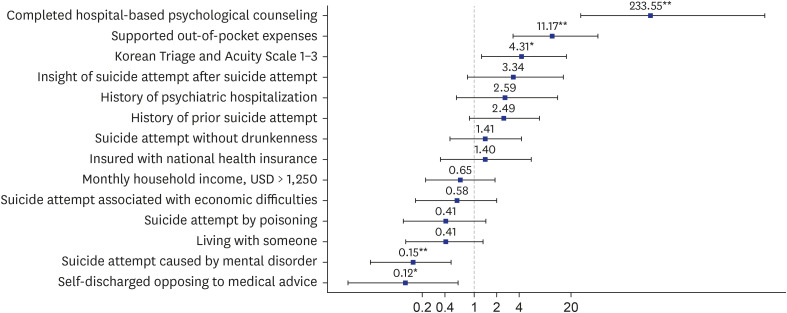
The results of the logistic regression analysis are presented in Fig. 1. Completed hospital-based psychological counseling, supported out-of-pocket expenses, KTAS score 1–3, suicide attempt associated with a mental disorder, and self-discharge against medical advice were independent factors influencing the collaboration between the emergency department and community-based mental healthcare centers in the management of suicide attempts.
DISCUSSION
We observed that completed hospital-based psychological counseling, supported out-of-pocket expenses, KTAS score 1–3, suicide attempt in association with mental disorder, and self-discharge against medical advice were factors influencing the collaboration between the emergency department and community-based mental healthcare centers in the management of suicide attempts. Completion of hospital-based psychological counseling was the most highly influential factor. The results regarding the factors influencing collaborations between the emergency department and community-based mental healthcare centers could be a theoretical foundation for the development of an appropriate suicide prevention system.
According to the 2018 Death and Cause of Death in Korea report, suicide is the fourth leading cause of death and the most common cause of death among people aged 10–40 years in Korea. The suicide rate in Korea was 26.6 per 100,000 people, which was the highest among the 36 countries of the Organization for Economic Co-operation and Development.17 However, these data include only completed suicides and tend to underestimate the frequency of suicide attempts in Korea. The lifetime prevalence of attempted suicide in Korea is known to be 3.2% (multiple 1.1%, and single 2.1%).18
Of the 743 patients who visited the emergency department after a suicide attempt within the study period, 55 (7.4%) died, which is consistent with the finding of a previous report in which the number of suicide survivors was much higher than the number of suicide victims.19 Furthermore, 19 (34.5%) patients who died had visited the same emergency department after a previous suicide attempt. This result is also consistent with the findings of previous research in which the experience of a previous suicide attempt was strongly associated with repeat suicide attempts.56
Among clinical factors, those associated with significant differences in the dependent variables were KTAS score 1–3 and self-discharge against medical advice. The lower proportion of patients with self-discharge opposing medical advice in the successful collaboration group was a predictable result. This result is consistent with the findings of previous research that suicide attempts with less severe injuries are associated with suicidal gestures related to personality disorders as impulsive gestures.20 In other words, it is possible that some of the subjects included in this study did not have a serious suicidal ideation.
Psychiatric factors associated with significant differences in the dependent variable were similar to characteristics of high-intent suicide attempters in the previous research. History of previous suicide attempts, history of psychiatric hospitalization, suicide attempt associated with a mental disorder, suicide attempt by poisoning, and suicide attempt without alcohol intoxication, which were associated factors in previous research, were analyzed as potentially influential factors in this study.21 Participants who strongly intend to commit suicide were more likely to have a successful collaboration; this may be because such individuals receive more attention from the emergency department and community-based mental healthcare centers.
Among the factors associated with socioeconomic status, the proportions of patients with monthly household income USD > 1,250, insured with national health insurance, and living with someone else were higher in the failed collaboration group. In contrast, the proportion of patients who need support for out-of-pocket expenses was higher in the successful group. In other words, the socioeconomic status of individuals who attempted suicide was lower in the successful group.
The variables that were significant in the logistic analysis were completed hospital-based psychological counseling, supported out-of-pocket expenses, KTAS score 1–3, suicide attempt associated with mental disorder, and self-discharge against medical advice. In successful collaborations between the emergency department and community-based mental healthcare centers, the impact of completed hospital-based psychological counseling was much greater than other significant variables.
This study had several limitations. First, because the data were collected from medical records and counseling records, it was difficult to identify accurate and objective information associated with socioeconomic status. Therefore, it is possible that the influence of socioeconomic status was underestimated. Second, although completion of hospital-based psychological counseling was the most highly influential factor, analysis of the quality of counseling, content of counseling, implementation of counseling, and benefit of counseling and counseling resources was not sufficient. Therefore, to evaluate more accurately the influence of counseling quality, studies specifically investigating counseling quality should be performed in the future. Third, the subjects in this study were patients who needed both medical treatment and psychiatric treatment. Therefore, it was not possible to conduct an analysis of patients who had only suicidal ideation. Fourth, this was a retrospective study based on medical records and counseling records, meaning that the statistical analysis could not necessarily completely control for confounders.
In conclusion, completion of hospital-based psychological counseling was the most significant factor influencing the collaboration between the emergency department and community-based mental healthcare centers in the management patients who attempted suicide. This suggests that completion of hospital-based psychological counseling will be expected to help reduce the risk of repeat suicide attempts. Therefore, we consider that hospital-based psychological counseling for patients who attempted suicide should be conducted in a large number of emergency departments than present.
 XML Download
XML Download