

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Colloids are theoretically more beneficial than crystalloids in augmenting intravascular blood volume, and possibly cerebral blood flow.1 Hydroxyethyl starch (HES, 6%) with molecular weight of 130 kD and molecular substitution ratio of 0.4 (130/0.4) has been used for this purpose. Despite the mechanisms of early neurological deterioration (END) are complex, cerebral hypoperfusion is regarded as a major cause.2 Therefore, treatment with induced hypertension and/or administration of volume expanders is considered to mitigate cerebral hypoperfusion in patients with END caused by cerebral hypoperfusion.34 Likewise, HES use was linked to a non-significant tendency toward better outcome in acute ischemic stroke.15 However, recent data showed that HES use was associated with adverse renal outcome in patients with sepsis or in critical conditions, which limited its use in intensive care units (ICUs).6789 Given that the rate of new-onset acute renal injury (AKI) and the usual dose of HES is much lower in patients with acute ischemic stroke compared to those with sepsis or in critical conditions,78 it is still not clear whether HES use is associated with renal adverse outcome in patients with acute ischemic stroke.
Go to : 
METHODS
Study population
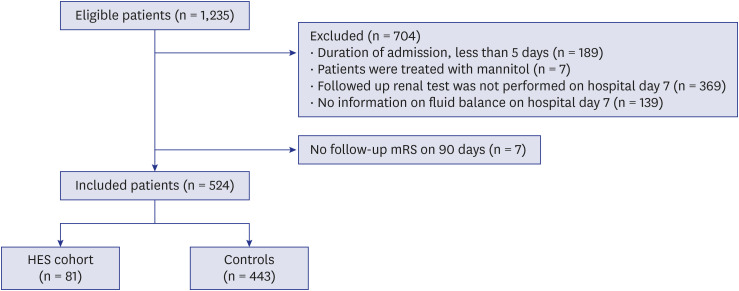
A retrospective analysis was performed on stroke registry. We initially screened 1,235 patients who were admitted to our institution under the diagnosis of acute ischemic stroke within 7 days from onset between January 2012 and May 2016. Excluded patients were those with duration of admission was less than 5 days (too short to determine renal function outcome, n = 189), those with incomplete information on follow-up renal function (n = 369) or fluid balance (n = 139), those with concomitant treatment with medications which might have affected the renal outcome (n = 7), and those without information on modified Rankin Scale (mRS) on day 90 after acute ischemic stroke (n = 7). As a consequence, a total of 524 patients were included for the analysis, regardless of renal status on admission (Fig. 1).
Baseline characteristics and laboratory findings
Baseline characteristics including risk factors and laboratory results were reviewed using electronic medical records. The stroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS) in all included patients at admission and on day 7. Baseline serum creatinine (SCr) and estimated glomerular filtration rate (eGFR) were assessed on admission, and at follow-up on hospital day 7 (± 2 days). The fluid balance on hospital day 7 was calculated from the net difference between the total amount of intravenous infusion volume (crystalloids and HES) and total urine output. The dose and infusion rate of HES was left at the discretion of the physician as part of clinical practice. In general, 500 mL of HES was infused over 24 hours for several consecutive days.10 eGFR was calculated using the Modification of Diet in Renal Disease (MDRD) equation.11 AKI was defined according to Kidney Disease: Improving Global Outcomes (KDIGO) guideline, as follows: 1) an increase in SCr by ≥ 0.3 mg/dL within 48 hours; or 2) increase in SCr to ≥ 1.5 times baseline, which is known or presumed to have occurred within the prior 7 days; or 3) urine volume less than 0.5 mL/kg/hour for more than 6 hours.1213 In addition, chronic kidney disease (CKD) was defined according to KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease, as follows: CKD is defined as abnormalities of kidney structure or function, present for > 3 months, with implications for health.14
Outcomes
The primary outcome was percentage of a new-onset AKI on hospital day 7 (± 2 days). The secondary outcome was the proportion of good functional outcomes (modified Rankin Scale [mRS], 0–2) at 90 days from the onset of acute ischemic stroke. In addition, END was defined as an increase 2 or more in the total NIHSS score or 1 or more in the motor NIHSS score within the first 72 hours of admission.1516 We re-evaluated NIHSS scores within 24 hours of END in patients with END.
Statistical analysis
Categorical variables are presented as percentages (%) and compared by a χ2 test or Fisher's exact test. Continuous variables are evaluated as mean ± standard deviation or median with interquartile range (IQR). We evaluated continuous variables by using a Student t test or a Mann–Whitney U test. For reducing selection bias caused by the differences between two groups who received HES or not, propensity score matching (PSM) was performed to balance the distribution of confounders across the two groups. Patients were matched 1 to 1 using matching algorithm. Baseline characteristics were analyzed in the matched and unmatched patients.17 In addition, the association between HES treatment and a new onset AKI was analyzed using logistic regression analyses. Covariates with statistically significant differences (P < 0.1) by univariate analysis and those with clinically important factors were adjusted for multivariate analysis. For all analyses, P < 0.05 was considered as significant. All data were analyzed using SPSS 23.0 (SPSS Inc., Chicago, IL, USA). GraphPad Prism (Version 8, GraphPad Software, San Diego, CA, USA) were performed for creating scientific graphs.
Ethics statement
The present study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. H-1009-062-332). Informed consent was waived by the IRB due to the retrospective study.
Go to :
RESULTS
Clinical characteristics
A total of 524 patients (male, 56.5%; mean age, 68.6 years) were included for the analysis (Table 1). Among them, 81 patients (15.5%) were treated with HES (HES cohort; mean cumulative dose, 1,450 ± 805 mL) for the treatment (n = 35) or prevention (n = 42) of END due to cerebral hypoperfusion. HES cohort were younger (mean age, 64.8 ± 14.7 years vs. 69.3 ± 12.5 years, P = 0.004) and were less likely to have atrial fibrillation (7.4% vs. 27.1%, P < 0.001) compared to controls. Large artery atherosclerosis was the most common (54.3%) stroke mechanism in HES cohort whereas cardioembolism was (38.6%) in controls (P < 0.001). After PSM, however, there were no differences in baseline characteristics between HES cohorts and controls. Major stroke risk factors did not differ between two groups. In addition, the percentage of patients with CKD (4.2% vs. 5.6%), those exposed to nonsteroidal anti-inflammatory drug (NSAIDs) (9.7% vs. 11.1%) or those who underwent radiological imaging using contrast agents (94.4% vs. 94.4%) did not differ between the groups. Baseline and discharge NIHSS were also not different between two groups after PSM (Table 1).
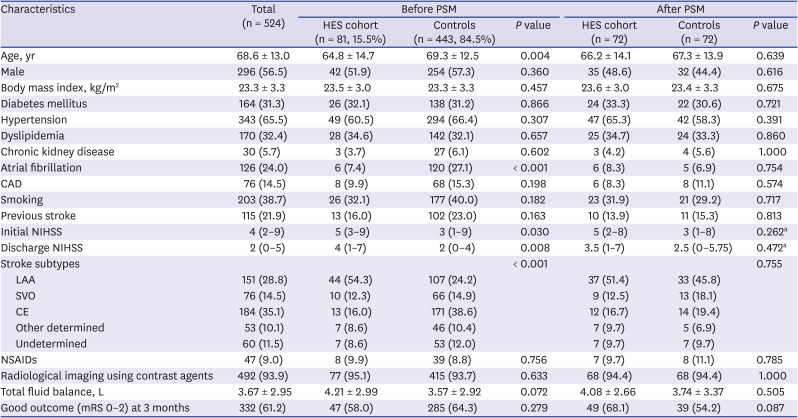
Table 1
Baseline characteristics of the study population
Data are presented as mean ± standard deviation or median (interquartile range) or number (%).
PSM = propensity score matching, HES = hydroxyethyl starch, CAD = coronary artery disease, NIHSS = National Institutes of Health Stroke Scale, LAA = large artery atherosclerosis, SVO = small vessel occlusion, CE = cardioembolism, NSAIDs = nonsteroidal anti-inflammatory drugs, mRS = modified Rankin Scale.
aMann-Whitney U test was used.
![]()
Laboratory findings and fluid balance
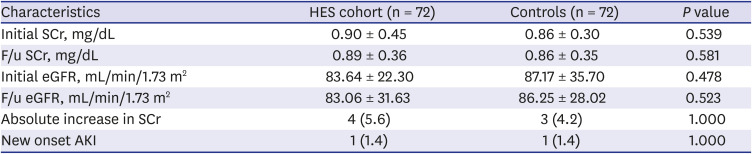
Initial and follow-up SCr and eGFR were comparable between HES cohort and controls (Table 2 and Fig. 2). Only 4 patients in HES group (5.6%) had an aggravation in SCr while 3 patients (4.2%) had in controls, which is not statistically tended (P = 1.000). Only a small percentage of patients in each group (1.4% vs. 1.4%) had a new onset AKI on day 7 based on KDIGO criteria. In addition, the total fluid balance over the hospital day 7 was positive and did not differ between HES groups and controls (Table 1).
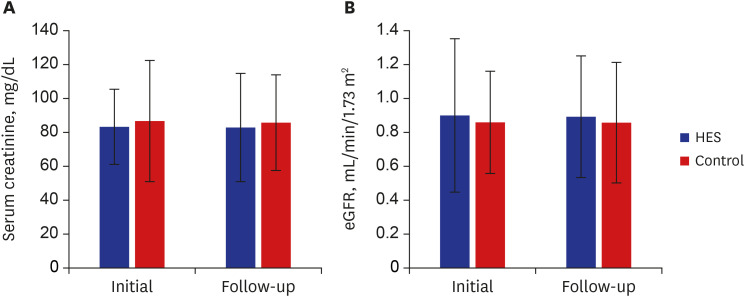 | Fig. 2The change of SCr and eGFR between HES cohorts and controls. (A) The initial and follow-up levels of SCr and (B) eGFR were not different between the two groups.HES = hydroxyethyl starch, SCr = serum creatinine, eGFR = estimated glomerular filtration rate.
|
Table 2
The changes of renal function over the study periods
Data are presented as mean ± standard deviation or number (%).
HES = hydroxyethyl starch, SCr = serum creatinine, f/u = follow-up, eGFR = estimated glomerular filtration rate, AKI = acute kidney injury.
![]()
The percentage of patients with previous history of CKD did not differ between HES cohort and controls. There was no interaction between the history of CKD and new-onset AKI. In HES group, none had a new-onset AKI out of 3 patients with CKD. In addition, no one in each group had a deterioration of renal function requiring renal replacement therapy (RRT). Multivariate logistic regression analysis showed that a new-onset AKI was not associated with HES treatment (odds ratio, 1.422; 95% confidence Interval, 0.072–28.068; P = 0.817) after adjusting for confounders (Table 3).

Table 3
Multivariate logistic regression analysis of the factors related with new-onset AKI
Adjusted covariates were age, initial NIHSS, fluid balance, and initial eGFR.
AKI = acute kidney injury, OR = odds ratio, CI = confidence interval, eGFR = estimated glomerular filtration rate, NIHSS = National Institutes of Health Stroke Scale, HES = hydroxyethyl starch.
![]()
The secondary outcomes, the proportion of good functional outcomes (mRS 0–2) at 3 months, were also compared in each group. Compared to controls, HES cohort had similar NIHSS score on admission and at discharge (Table 1). Likewise, the proportion of patients with good functional outcome (mRS 0–2) at 3 months did not differ between HES cohort and controls (Table 1). Among the total of 23.6% (n = 34) of the patients experienced END in 72 pairs of PSM. In 72 pairs of PSM patients, the proportion of the patients with END was higher in HES group compared to control group (41.2% in HES group vs. 7.9% in controls, P < 0.001). Moreover, the NIHSS score at the time of END was significantly higher in HES group (median, 7 [6–11] vs. 6 [3–9], respectively, P = 0.039). The NIHSS score at 24 hours after the onset of END was not significantly different in two groups (median, 7 [5–11], in HES vs. 5 [3–9], in controls, P = 0.202). In 24 hours after the onset of END, more patients in HES group had an improvement in neurological symptoms compared to the control groups assessed by NIHSS score (46.4% vs. 28.6%, P = 0.036).
Go to :
DISCUSSION
In this study, we found that administration of a low cumulative dose of HES was not associated with new-onset AKI in patients with acute ischemic stroke, regardless of the previous history of CKD.
HES has a theoretical advantage over crystalloid in augmenting intravascular volume.25610 However, the role of HES as a volume expander has recently lost popularity since the publication of several clinical trials which raised renal concerns, such as new-onset AKI or requirement of RRT in patients with critically ill or septic shock.78 In contrast, our results showed that the use of HES in ischemic stroke was safe and did not increase the risk of new-onset AKI. There are several possibilities why HES use showed different renal outcomes. First, the total amount of HES was lower in our study. The average cumulative dose of HES was 1.45 L during our study (2.7 ± 1.5 day), which is much lower than that in septic shock or critical condition in the literature (approximately 3.0 L [first 4 days] and 4.7 L [first 3 days], respectively).78 Given that the risk of renal injury increases with a higher dose of HES in septic shock, the relatively lower dose of HES in our study may explain the lack of association between HES users and new-onset AKI. Second, new-onset AKI is not common in patients with ischemic stroke. The incidence of new-onset AKI in ischemic stroke is reported as high as 11%, which is only one-sixth of the incidence in septic shock (60%).18 As described above, the rate of new-onset AKI was only 1.4% in both groups, which is lower than previous reports. Over the 7 days of hospital stay, eGFR and SCr did not change regardless of HES use. The patients in both groups had a positive fluid balance over the study periods, which might have affected better SCr and eGFR mediated by hemodilution effect.19 However, we do not think that renal toxicity of HES was masked by hemodilution effect because the fluid balance was also similar in both groups.
The definition of AKI varies according to the criteria. Therefore, the incidence of AKI may differ based on the criteria in each study. In our study, we used the KDIGO criteria for defining a new-onset AKI. Previous studies which raised renal concerns of HES used the Renal Serial Organ Failure Assessment score or Risk, Injury, Failure, Loss of kidney function, and end-stage kidney disease (RIFLE) criteria.78 RIFLE criteria is less sensitive in identifying relative renal deterioration and has limitations in predicting mortality or requirement of RRT. The Acute Kidney Injury Network (AKIN) classification, another AKI criteria, requires an adequate hydration status to be achieved. AKIN classification requires two SCr measurements at least 48 hours apart; however, it does not require baseline SCr to define AKI.181920212223 However, KDIGO definition is regarded as more accurate in diagnosing AKI, as it better predicts mortality and the risk of RRT compared to other definitions.2425 However, most patients in this study were diagnosed using the change of SCr greater than 1.5 times on day 7 because not all of the patients underwent SCr on day 2 and the measurement of hourly urine output was not feasible in the non-ICU setting. With these limitations, we think that the low incidence of AKI in HES cohort in our study was true not rather than the underestimation of AKI owing to its less sensitive definition.
The clinical benefit of HES in patients with ischemic stroke still remains to be elucidated. Although small non-randomized observational studies have shown a positive trend in patients after HES cohort, more direct evidence is lacking.235 In this study, END events occurred more frequently in HES group compared to controls because END triggered the use of HES. Besides, the NIHSS score at the time of END was higher in HES group compared to the control. However, the proportion of the improvement in NIHSS score within 24 hours after the END was significantly higher in the HES group, which could possibly suggest the beneficial effect of HES treatment in END.235 Additionally, we tried to compare the functional outcome of the ischemic stroke at day 90 between HES cohort and controls. However, initial stroke severity and baseline risk factors differed between the groups. Moreover, the percentage of patients with a good functional outcome did not differ between HES cohort and controls.
This study has several limitations. First, this was a retrospective study based on registry data. Therefore, a certain degree of bias is inevitable. Second, HES cohort and controls were not initially balanced with regard to the baseline risk factors, which was properly adjusted using PSM. Third, renal function was affected by multiple factors such as decreased renal blood flow, exposures to nephrotoxic drugs, and post-renal obstructions. Although we adjusted the pre-renal factors using fluid balance over 7 days and the use of nephrotoxic medications, we could not measure post-renal factors or information on renal perfusion such as blood pressure. In patients with END due to cerebral hypoperfusion, induced hypertension could be used as an alternative treatment option.26 In our patients, only 2 patients (1 in HES group and 1 in controls) were treated with induced hypertension. The effect of induced hypertension on renal outcome could not be evaluated in this study, which requires further studies. Fourth, the duration of renal function follow-up was limited. In patients with acute ischemic stroke, examinations were often conducted with a focus on whether the clinical symptoms worsened and the risk factors (DM, HTN, dyslipidemia, etc.) that greatly affected the occurrence of acute ischemic stroke after hospitalization.27 Therefore, in order to confirm changes in renal function, laboratory tests were not performed within 48 hours after admission. Moreover, the duration of renal function follow-up was only 7 days, which may be insufficient to evaluate long-term renal outcomes. We did not have information on renal function recovery after the study period. With these limitations, we think that a low dose of HES for treating hypoperfusion in patients with acute ischemic stroke does not negatively affect renal outcome, regardless of baseline renal function.
Go to :
 XML Download
XML Download