

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) is an ongoing pandemic characterized by high morbidity and mortality. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus responsible for COVID-19, causes respiratory and intestinal infections in humans and animals.12 Strokes in patients with COVID-19 have recently been reported, and for neurologists, strokes that occur during pandemics are highly problematic.34 The mechanisms, phenotype, and optimal management of strokes in COVID-19 patients are unresolved. To determine how COVID-19 might cause or exacerbate ischemic stroke, we describe five patients with both diseases who were treated by us over the course of 3 months. We also discuss the problems associated with stroke management during epidemics.
CASE DESCRIPTION
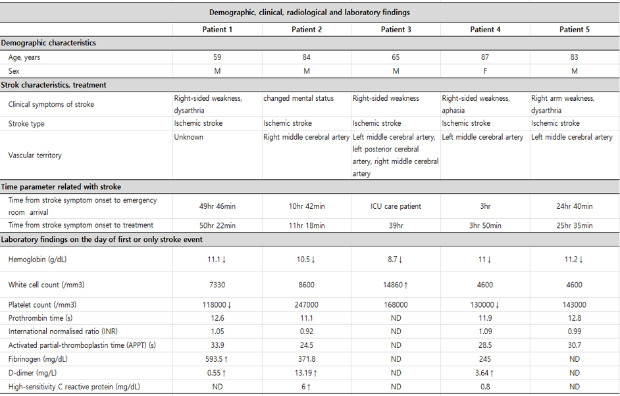
The Korean city of Daegu endured the first large COVID-19 outbreak outside of China. The first confirmed case in Daegu was reported on February 18, 2020, and 6,880 confirmed cases were reported by May 29, 2020.56 A search of a retrospectively mainlined database identified five patients who were treated for both COVID-19 and ischemic stroke at four tertiary hospitals in Daegu during this time period. COVID-19 was confirmed via real-time reverse transcription polymerase chain reaction (RT-PCR). Stroke was diagnosed by clinical presentation and neurological examination, and later confirmed by computed tomography (CT) and magnetic resonance imaging (MRI) of the brain. We compiled the demographic, clinical, radiological, and laboratory characteristics of the five patients (Tables 1-4).
Table 1
Demographics and stroke characteristics
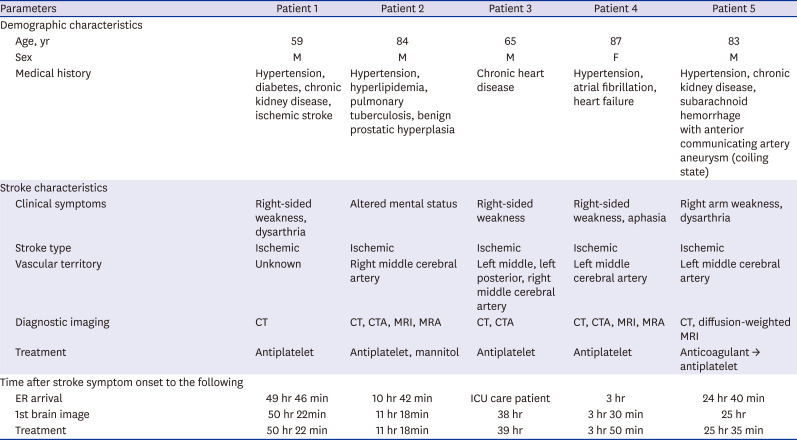
Table 2
Signs and symptoms related to COVID-19
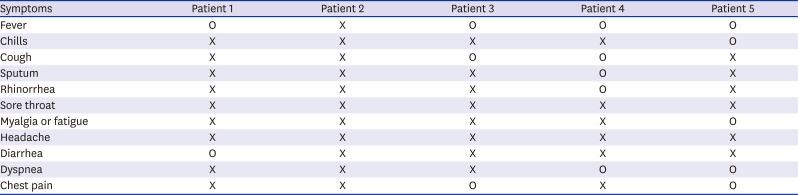
Table 3
Laboratory findings on the day of the first or only stroke event
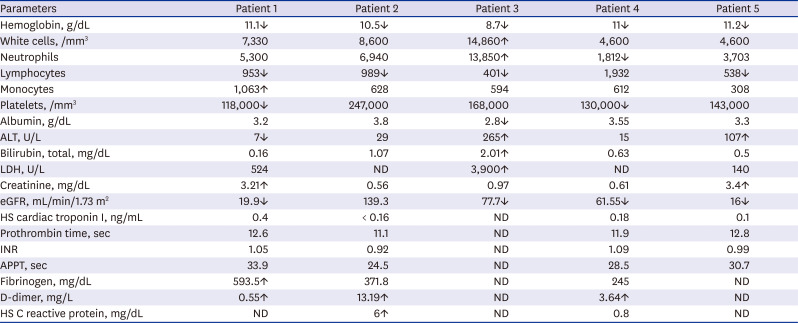
Table 4
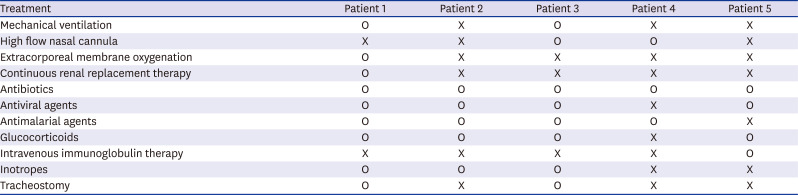
Treatment for coronavirus disease 2019
Patient 1
On March 12th, a 59-year-old man with hypertension, diabetes, chronic kidney disease, and previous ischemic stroke presented with transient dysarthria and right-sided weakness. He arrived at the emergency room 49.8 hours after symptom onset. Brain CT showed normal findings, and a transient ischemic attack was diagnosed. After arrival at the hospital, he complained of fever and diarrhea. RT-PCR confirmed SARS-CoV-2 infection, and antiviral and antimalarial agents were administered. Laboratory tests showed high levels of D-dimer (0.55 mg/L) and fibrinogen (593.5 mg/dL). Owing to chronic kidney disease, the estimated glomerular filtration rate (eGFR) was very low (19.9 mL/min/1.73 m2). On day 2, he developed severe respiratory symptoms and was admitted to the intensive care unit for mechanical ventilation and extracorporeal membrane oxygenation (ECMO). On day 3, he developed acute left-sided weakness. Further stroke evaluations could not be performed because of the mechanical ventilation and ECMO treatment.
Patient 2
On March 18th, an 84-year-old man with hypertension, hyperlipidemia, and previous pulmonary tuberculosis presented with an altered mental status. He arrived at the emergency room 10.7 hours after symptom onset. Brain MRI and angiography confirmed acute infarction in the right middle cerebral artery (MCA) territory (Fig. 1A) and occlusion of the right MCA M1 segment. Although he had no COVID-19-related symptoms, RT-PCR confirmed SARS-CoV-2 infection. Laboratory tests showed elevated levels of D-dimer (13.19 mg/L) and high-sensitivity C reactive protein (6 mg/dL).
Fig. 1
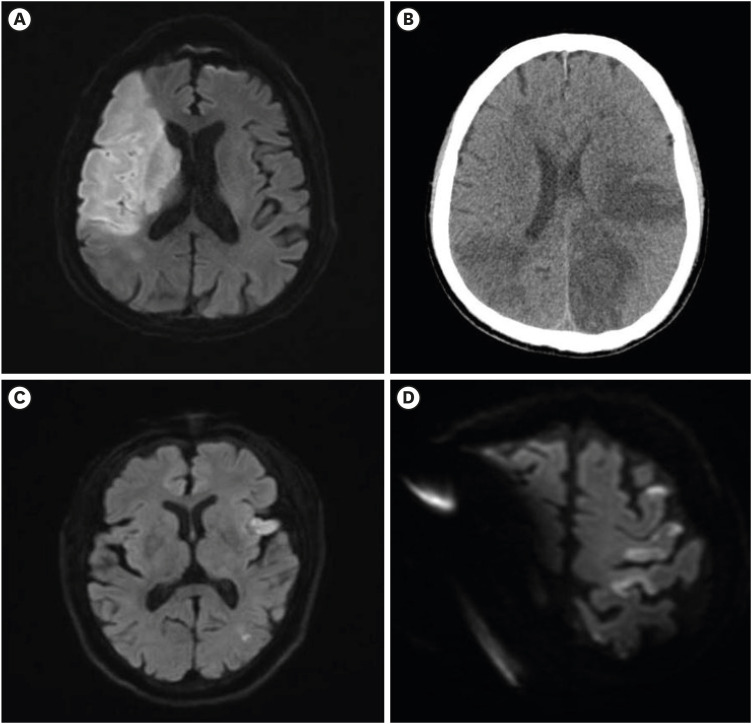
Radiologic findings of the patients.
(A) Patient 2. Diffusion-weighted brain MRI showed acute infarction in the right MCA territory. (B) Patient 3. Brain computed tomography showed multiple hypodense lesions in both the MCA and left posterior cerebral artery territories. (C) Patient 4. Diffusion-weighted brain MRI showed acute multiple embolic infarction in the left MCA territory. (D) Patient 5. Diffusion-weighted brain MRI showed acute multiple embolic infarction in the left MCA territory along with artifacts.
MRI = magnetic resonance imaging, MCA = middle cerebral artery.
Patient 3
On April 4th, a 65-year-old man presented 7 days after the onset of COVID-19 symptoms (fever, cough, and chest pain), with respiratory failure warranting mechanical ventilation in the intensive care unit. He had chronic heart disease. Pseudomonas aeruginosa infection was treated with piperacillin/tazobactam and levofloxacin. On hospital day 13, he began to recover consciousness. However, upon regaining consciousness, right-sided weakness, which had not documented before, was discovered. Brain CT showed multiple hypodense lesions in both the MCA and left posterior cerebral artery territories (Fig. 1B). Because CT angiography findings were normal, a cardioembolic stroke was suspected, and a transthoracic echocardiogram (TTE) was performed to assess the cause of the stroke. The TTE revealed a vegetation of about 5 mm in size on the mitral valve, and endocarditis was diagnosed. Laboratory tests showed that the eGFR was low (77.7 mL/min/1.73 m2). Blood coagulation tests including measurement of D-dimer levels were not performed at the time of symptom onset.
Patient 4
On April 17th, an 87-year-old woman with hypertension, atrial fibrillation, and heart failure presented with right-sided weakness and aphasia. She arrived at the emergency room 3 hours after symptom onset. Brain MRI and angiography showed acute multiple infarctions in the left MCA territory without occlusion or stenosis of the intracranial or extracranial arteries (Fig. 1C). After arrival at the hospital, she complained of fever, cough, sputum, rhinorrhea, and dyspnea. RT-PCR confirmed SARS-CoV-2 infection, and, laboratory tests showed high D-dimer levels (3.64 mg/L) and a low eGFR (61.55 mL/min/1.73 m2).
Patient 5
On May 20th, an 83-year-old man taking aspirin presented with right arm weakness and dysarthria. He arrived at the emergency room 24.7 hours after symptom onset. He had hypertension and chronic kidney disease and had previously been treated for subarachnoid hemorrhage via endovascular coiling of an aneurysm in the anterior communicating artery. Brain MRI confirmed acute multiple infarctions in the left MCA territory (Fig. 1D). After arrival at the hospital, he complained of fever, chills, myalgia, dyspnea, and chest pain. RT-PCR confirmed SARS-CoV-2 infection, and laboratory tests showed that the eGFR was very low (16 mL/min/1.73 m2) because of chronic kidney disease. The D-dimer test was not performed.
DISCUSSION
In our study, D-dimer (reference value: < 0.4 mg/L, turbidimetric immunoassay) levels were high in all three patients (Patients 1, 2, and 4) who underwent D-dimer blood tests. In Patient 1, high D-dimer levels (0.55 mg/L) were accompanied by exceptionally high fibrinogen levels (593.5 mg/dL). Three of the five patients (Patients 2, 4, and 5) had multiple embolic infarctions. Although not confirmed via brain imaging, another patient (Patient 1) was thought to have an embolic infarction because his symptoms changed from right-sided to left-sided.
The most influential hypothesis implicates SARS-CoV-2-induced inflammatory responses in the onset or worsening of stroke. These responses activate proinflammatory cytokines, resulting in coagulation and thrombin generation and consequent thromboembolism and D-dimer accumulation.8910 This mechanism may explain the high D-dimer levels and multiple embolic infarctions in most of our patients. However, owing to the presence of multiple vascular risk factors in most stroke patients, our data cannot confirm a causal relationship between SARS-CoV-2 infection and stroke.
Typical symptoms of COVID-19 include fever, cough, sputum, shortness of breath, fatigue, and diarrhea. In particular, it invades the lungs, causing severe acute respiratory distress syndrome (ARDS), respiratory failure, and death.11 Most of the patients included in our study complained of fever and/or cough, two of whom required mechanical ventilation for ARDS. Notably, in four of the five patients, SARS-CoV-2 infection was confirmed after stroke diagnosis in the emergency room. In other words, despite SARS-CoV-2 positivity, they had no apparent COVID-19-related symptoms and visited the emergency room owing to stroke-related symptoms. In fact, one patient (Patient 3) had no COVID-19 related symptoms even after admission. Hence, the attending medical staff members were quarantined for 2 weeks, and the inspection equipment was disinfected before reusing to prevent the spread of infection. In the emergency room, medical spaces for COVID-19 positive, COVID-19 negative and suspected COVID-19 patients should be highly compartmentalized. Most importantly, patients and medical staffs should wear recommended personal protection equipment such as respirators, eye protection, gowns, and gloves.
Stroke patients are reluctant to go to the hospital for fear of contracting the virus and are ill-served by emergency responses that prioritize the infectious diseases. Because all efforts were concentrated on COVID-19 treatment, stroke evaluation was improperly performed in the cases presented here. Patient 1 did not undergo brain imaging after the relapse of stroke symptoms, and Patient 5 did not undergo brain angiography. Only one of the five patients (Patient 3) underwent TTE. Moreover, the mean time from symptom onset to emergency room arrival was 22 hours in our study. This is far longer than the median time of 6.2 hours reported by the Clinical Research Collaboration for Stroke in Korea statistics in 2018.12 Hence, acute treatment for ischemic stroke was delayed.
The control of COVID-19 is very important, but at the same time, stroke management should not be neglected. Recently, consensus-reached recommendations for delivering high quality treatments to stroke patients during the COVID-19 pandemic have been proposed.13 The main limitation of this study is the small number of patients. Hence, studies with larger sample sizes are needed to confirm our conjectures. However, our findings provide early insights into stroke and stroke care in COVID-19 patients in epidemic conditions.
Ethics statement
This case was reviewed and approved by the Institutional Review Board (IRB) of Keimyung University Dongsan Hostpial (IRB No. 2020-08-044). Requirement for informed consent was waived after review of IRB because it was practically impossible and this study was of retrospective design.
 XML Download
XML Download