

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In Korea, low birthrate is now emerging as a serious social problem, and the tendency toward late marriage is considered to be the cause of this phenomenon. The tendency to postpone marriage is continuously strengthened due to various economic, social, and cultural factors. As a result, the age with respect to first marriage continues to increase. In accordance with the population trend survey of the Korea National Statistical Office, the mean first marriage age for men increased from 29.3 years in 2000 to 32.9 years in 2016 while the mean first marriage age for women increased from 26.5 years to 30.1 years during the same period.1
Through several studies based on the positive effects of maintaining one's marital status on health,23 we can infer the negative effects of never-married status. Married people were found to have lower psychological stress and greater life satisfaction than never-married people45; moreover, married people were observed to have better health conditions than never-married people when examined for various diseases including mental disorders, suicide risks, and mortality.67891011 The Organisation for Economic Co-operation and Development's (OECD) estimated that Korea's suicide rate is more than twice as high as the OECD countries' average suicide rate.12 Additionally, the annual social cost of suicide in Korea was about 6.5 trillion won in 2014, and the impact of suicide on the Korean society is very serious.13 To reduce the suicide rate, it is important to screen and prevent suicide by considering various risk factors.
Marriage seems to have several positive effects. First, the roles of spouses in marriage form a major component in shaping an adulthood identity, and married people receive social and psychological support from their families.14 Second, sharing economic resources with a spouse increases access to health care and reduces stress associated with financial issues4; married people tend to do less harm to their health than never-married people. In addition to these protective effects of marriage, positive aspects are explained through the selective effect that healthy people are more prone to get and stay married, but unhealthy people are less prone to get married or may be separated, divorced, or experiencing bereavement status.4615
Due to the worsening of the overall employment situation in recent years, men and women of marriageable age are delaying marriage, as they cannot afford to get married16; in addition, there is anxiety about bearing and raising children in the future.16 However, the expectation of marriage by parents or people around them causes significant stress, and the extent of interpersonal relations decreases as their friends and acquaintances start getting married. These changes often occur as the age of never-married people passes the mean marriage age. Additionally, a prejudice that there is something wrong with never-married people above the marriageable age damages their self-esteem.1718192021 Therefore, maintaining their never-married status beyond the mean marriage age could be a psychological burden for many people.
To date, many studies have explored the association of never-married status with mental health2223242526272829303132; however, no study has scrutinized the impact of diverse status in never-married people, i.e., getting older than mean marriage age, on mental health. From the public health viewpoint, establishing a risk factor for a disease and mortality is very crucial. This study investigated the impact of getting older than the mean marriage age alone on mental disorders and suicidality.
Go to : 
METHODS
Participants
We conducted a nationwide study of mental disorders, the Korean Epidemiologic Catchment Area Study-2016 (KECA-2016), from April to November in 2016. We employed a stratified multistage cluster sampling method to select respondents, which was based on the 2010 census of population and housing data in Korea.
From 21 community catchment areas throughout the country, we extracted the sample of the respondents. Primary and secondary sampling units (Si/Gun/Gu and Eup/Myeon/Dong, respectively, in Korean) were considered as the administrative regions. Tertiary sampling units were developed for the official announcement of statistics, and the size of which were about one-thirtieth of the size of Eup/Myeon/Dong. Chunks representing the quaternary sampling units consisted of 24 households. Finally, a segment selected from each chunk through systematic sampling methods composed four households and represented the ultimate sampling units. Employing the last-birthday method, we selected and interviewed one person per household. In total, 147 interviewers took a training session over five-days in accordance with the standard protocols developed by the World Health Organization (WHO). Interviews were performed face to face with 5,102 subjects aged over 18 years old living in the community. In this study, we defined the mean marriage age, i.e., the mean age of first marriage (men = 32.8 years; women = 30.1 years), according to the 2016 population trend survey of Korea National Statistical Office.1
Assessment of sociodemographic factors
We gathered the data on sociodemographic factors during interviews: marital status (separated, divorced, or widowed/never married/married), age, gender (men/women), number of years of education (less than 12 years/more than 13 years), employment status (employed/unemployed), area of residence (urban/rural), living arrangement (alone/not alone), and average monthly household income (≤ 2,000,000 Korean won [KRW]/2,000,000–4,000,000 KRW/≥ 4,000,000 KRW).
Assessment of the mental disorders
The KECA-2016 employed the Korean version of the Composite International Diagnostic Interview 2.1 (K-CIDI) for assessing the mental health. The CIDI 2.1 was a standardized diagnostic tool, and a structured interview that could be applied by trained general people.33 It was translated into Korean in accordance with the WHO guidelines.34 Moreover, K-CIDI has been previously verified in terms of reliability and validity by Cho et al.33
We evaluated the mental disorders using the Diagnostic and Statistical Manual of Mental Disorders, fourth edition classification in the KECA-2016.35 The mental disorders assessed in this study were psychotic disorders (delusional disorder, brief psychotic disorder, schizoaffective disorder, schizophreniform disorder, and schizophrenia), mood disorders (bipolar disorder, dysthymic disorder, major depressive disorder), nicotine use disorders (nicotine withdrawal and nicotine dependence), anxiety disorders (post-traumatic stress disorder, generalized anxiety disorder [GAD], specific phobia, agoraphobia, panic disorder, social phobia, obsessive–compulsive disorder [OCD]) and alcohol use disorders (alcohol dependence and alcohol abuse).
Assessment of the suicidal ideations, intentions, and attempts
We assessed suicidality employing the modified Suicide Prevention Multisite Intervention Study on Suicidal Behaviors that was devised by the WHO.36 We conducted assessment using the following three questions. “Have you ever seriously thought about committing suicide?” was the question used to assess lifetime suicidal ideations; “Have you ever made a plan for committing suicide?” was the question used to assess lifetime suicide plans; “Have you ever attempted suicide?” was the question used to assess lifetime suicide attempts.
Statistical analysis
We assigned the standardized weighted values to approximate the national population regarding gender and age, for each respondent, using the 2015 census of Korea National Statistical Office. We conducted Pearson's χ2 test to compare gender, number of years of education, area of residence, employment status, and household income between groups. An independent t-test was employed to compare ages between groups. We conducted logistic regression analyses to assess the effect of sociodemographic factors on never-married status. To calculate the odds ratios (ORs) and 95% confidence intervals (CIs) for mental disorders and suicidality, we conducted logistic regression analyses using the never-married status as the independent variable after adjustment for age, gender, number of years of education, employment status, area of residence, living arrangement, and household income in both above- and under-the-mean-marriage-age groups. In the suicidality, we conducted additional analyses with adjustments for sociodemographic factors and mental disorders. For the never-married group, we additionally analyzed ORs of mental disorder and suicidality for those who are above the mean marriage age compared with those who are under the mean marriage age. In addition, we divided never-married people above the mean marriage age into two groups (younger old/older old) based on the median age of the above the mean marriage age group in the study sample (men = 40.0 years; women = 37.0 years) and scrutinized attendant risks of mental disorder and suicidality for each group because social norms for the age of older unmarried men and older unmarried women are higher than the mean marriage age. Furthermore, the older-old group is supposedly more likely to be under greater social pressure to marry, resulting in greater psychological burden. We investigated ORs of mental disorders and suicidality using each above-the-mean-marriage-age group (younger-old/older-old) as the independent variable with the under-the-mean-marriage-age group as the reference group. Instead of having separate groups for individual psychotic disorders, we categorized them all under the “psychotic disorders” group in the analyses, as there were very few respondents diagnosed with each disorder. All statistical analyses were executed employing SPSS version 25.0 for Windows software (IBM Co., Armonk, NY, USA). In this study, for all analyses, P values of < 0.05 were regarded as statistically significant.
Ethics statement
The Institutional Review Board of Samsung Seoul Hospital permitted this study (approval No. 2016-05-014). Informed written consent was provided by each participant before participation.
Go to :
RESULTS
Descriptive statistics
Of 5,102 respondents, we recruited 3,665 respondents who are married or have never been married (excluding statuses such as widowed, divorced, or separated). Table 1 exhibits the sociodemographic characteristics of study participants. The sociodemographic factors associated with the never-married status varied depending on above- or under-the-mean-marriage-age (Table 2). Never-married people above the mean marriage age accounted for 6.4% of Korea's general population. Factors such as younger age, men, urban residence, living alone, and lower household income (less than 2,000,000 KRW) were associated with increased OR for never-married status in the group above the mean marriage age. People who have never been married and are under the mean marriage age accounted for 19.5% of Korea's general population. Factors such as younger age, men, more number of years of education (more than 13 years), living alone, and low household income (less than 2,000,000 KRW) were associated with increased OR for never-married status among the respondents in the group under the mean marriage age.
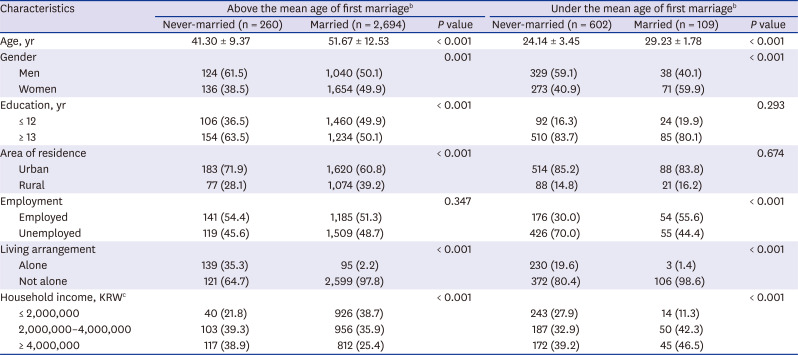
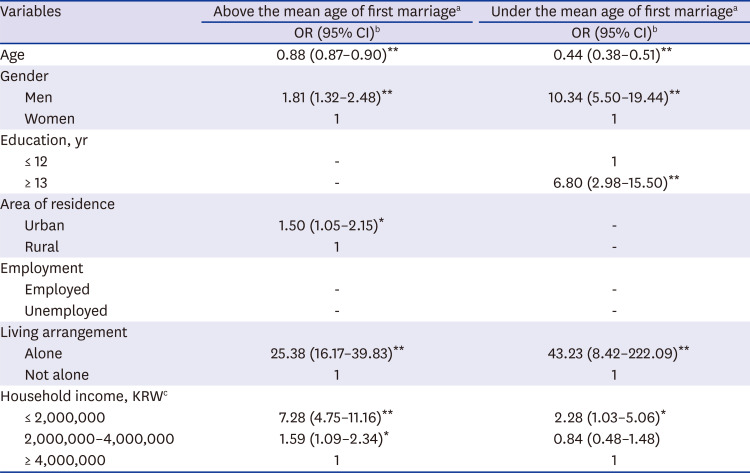
Table 1
Sociodemographic characteristics of study participantsa
Data are presented as mean ± standard deviation or number (%).
KRW = Korean won.
aThe number of study participants was not weighted, but other demographic characteristics were assigned standardized weighted values in respect of gender and age as defined by the 2015 census of Korea National Statistical Office.; bThe mean age of first marriage was 32.8 years for men and 30.1 years for women, according to the data from the 2016 population trend survey of Korea National Statistical Office; c1 US dollar = 1,133.89 KRW at the time of survey.
![]()
Table 2
Results of logistic regression of sociodemographic factors associated with never-married people
OR = odds ratio, CI = confidence interval, KRW = Korean won.
*P < 0.05, **P < 0.001.
aThe mean age of first marriage was 32.8 years for men and 30.1 years for women, according to the data from the 2016 population trend survey of Korea National Statistical Office; bAfter controlling for other sociodemographic factors in multiple logistic regression analyses with a backward stepwise method; c1 US dollar = 1,133.89 KRW at the time of survey.
![]()
Association of marital status with mental disorders
Table 3 demonstrates the prevalence and ORs of mental disorders in never-married people compared with married people. In the group above the mean marriage age, people who have never been married were more likely to have agoraphobia (adjusted OR [aOR], 6.95; 95% CI, 1.57–30.66), OCD (aOR, 5.45; 95% CI, 1.63–18.20), mood disorders (aOR, 2.06; 95% CI, 1.11–3.84), and major depressive disorder (aOR, 2.31; 95% CI, 1.24–4.28) when controlling for sociodemographic factors. On the contrary, in the group under the mean marriage age, people who have never been married were less likely to have GAD (aOR, 0.06; 95% CI, 0.01–0.37), alcohol use disorders (aOR, 0.54; 95% CI, 0.29–1.00), and alcohol dependence (aOR, 0.38; 95% CI, 0.16–0.91).
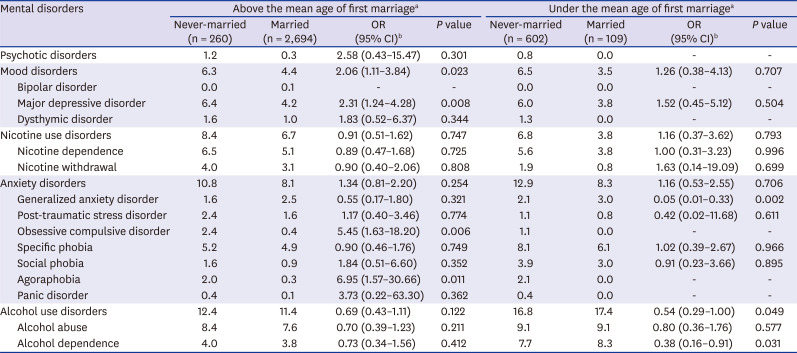
Table 3
Prevalence and ORs of mental disorders in never-married people compared with married people
Values are presented as number (%).
OR = odds ratio, CI = confidence interval.
aThe mean age of first marriage was 32.8 years for men and 30.1 years for women, according to the data from the 2016 population trend survey of Korea National Statistical Office; bAfter controlling for age, gender, number of years of education, employment status, area of residence, living arrangement, and household income.
![]()
Association of the marital status with suicidality
The prevalence and ORs of suicidality in never-married people compared with married people are exhibited in Table 4. About 22.1%, 5.5%, and 5.6% of the never-married people above the mean marriage age reported the experience of suicidal ideations, suicide plans, and suicide attempts, respectively. This prevalence was significantly higher than that of married people (14.1%, 2.1%, and 1.8%, respectively). When we considered the people above the mean marriage age, individuals who have never been married were 2.6-fold more likely to have made suicide plans (aOR, 2.56; 95% CI, 1.19–5.51) and 3.5-fold more likely to have attempted suicide (aOR, 3.46; 95% CI, 1.61–7.46) after controlling for sociodemographic factors. The association of never-married status with suicide attempts (aOR, 3.21; 95% CI, 1.36–7.60) remained significant after controlling for sociodemographic factors and mental disorders. Approximately 17.4% of never-married people under the mean marriage age reported having experienced suicidal ideations, which was significantly higher than married people (9.9%). Among individuals who were under the mean marriage age, never-married status was not associated with suicidality after controlling for sociodemographic factors or for mental disorders and sociodemographic factors.

Table 4
Prevalence and ORs of suicidality in never-married people compared with married people
Values are presented as number (%).
OR = odds ratio, CI = confidence interval.
aThe mean age of first marriage was 32.8 years for men and 30.1 years for women, according to the data from the 2016 population trend survey of Korea National Statistical Office; bAfter controlling for age, gender, number of years of education, employment status, area of residence, living arrangement, and household income; cAfter controlling for age, gender, number of years of education, employment status, area of residence, living arrangement, household income, and mental disorders.
![]()
Associations of age with mental disorders and suicidality in never-married people
In never-married people, the above-the-mean-marriage-age group was not associated with an increased prevalence of mental disorders compared with the under-the-mean-marriage-age group. When scrutinizing the above-the-mean-marriage-age group, the younger-old group did not show increased OR for any mental disorders compared with the under-the-mean-marriage-age group. However, the older-old group was 6.3-fold more likely to have GAD (aOR, 6.32; 95% CI, 1.01–39.44) compared with the reference group controlling for sociodemographic factors.
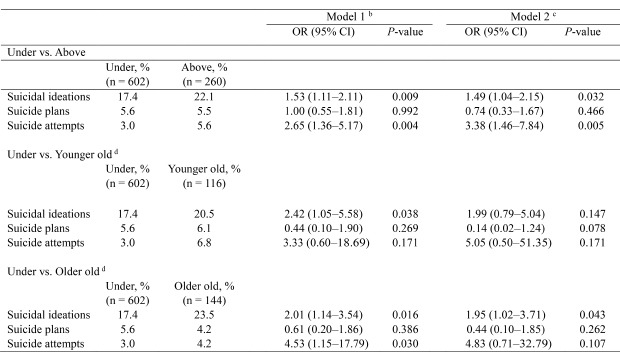
Table 5 demonstrates the prevalence and ORs of suicidality of those who have never been married and are above the mean marriage age compared with those who have never been married and are under the mean marriage age. People who have never been married and are above the mean marriage age are 1.5-fold more likely to have thought about suicide (aOR, 1.53; 95% CI, 1.11–2.11) and 2.7-fold more likely to have attempted suicide (aOR, 2.65; 95% CI, 1.36–5.17) compared with never-married people under the mean marriage age after adjusting for sociodemographic factors. The association of getting older than the mean marriage age with suicidal ideations (aOR, 1.49; 95% CI, 1.04–2.15) and suicide attempts (aOR, 3.38; 95% CI, 1.46–7.84) remained significant when controlling for mental disorders and sociodemographic factors. The prevalence and ORs for suicidality of those who are in the younger-old/older-old group within the above-the-mean-marriage-age group are also shown in Table 5. The younger old group was 2.4-fold more likely to have thought of suicide (aOR, 2.42; 95% CI, 1.05–5.58) after adjusting for sociodemographic factors. The older-old group was 2.0-fold more likely to have thought of suicide (aOR, 2.01; 95% CI, 1.14–3.54) and 4.5-fold more likely to have attempted suicide (aOR, 4.53; 95% CI, 1.15–17.79) after adjusting for sociodemographic factors. The older-old group was still significantly associated with suicidal ideations (aOR, 1.95; 95% CI, 1.02–3.71) when controlling for sociodemographic factors and mental disorders.
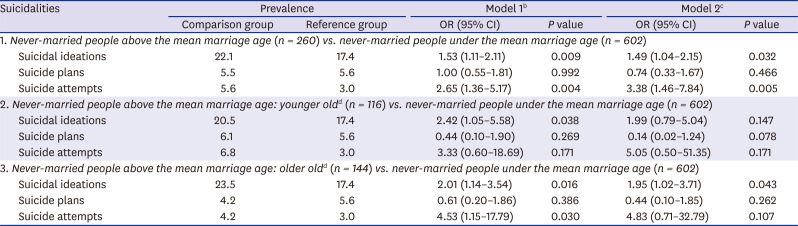
Table 5
Prevalence and ORs of suicidality in never-married people above the mean marriage age compared with never-married people under the mean marriage agea
Values are presented as number (%).
OR = odds ratio, CI = confidence interval.
aThe mean marriage age was 32.8 years for men and 30.1 years for women, according to the data from the 2016 population trend survey of Korea National Statistical Office; bAfter controlling for age, gender, number of years of education, employment status, area of residence, living arrangement, and household income; cAfter controlling for age, gender, number of years of education, employment status, area of residence, living arrangement, household income, and mental disorders; dWe divided the above-the-mean-marriage-age group into two groups (younger old/older old) based on the median age (men = 40.0 years; women = 37.0 years) of the above-the-mean-marriage age group in the sample.
![]()
Go to :
DISCUSSION
We investigated the different associations of marital status with mental disorders and suicidality above- and under-the-mean-marriage-age. In the above-the-mean-marriage-age group, the never-married people were more likely to have mental disorders (agoraphobia, OCD, mood disorders, and major depressive disorder) and suicidality (suicide attempts), which is congruous with previous findings. However, in the under-the-mean-marriage-age group, the never-married people were not more likely to have mental disorders and suicidality; on the contrary, they were less likely to have GAD, alcohol use disorders, and alcohol dependence. In addition, never-married people above the mean marriage age were more likely to have experienced suicidal ideations and have attempted suicide compared with those under the mean marriage age when controlling for sociodemographic factors and mental disorders. These findings suggest that never-married people are not homogeneous, and the impacts of never-married status on mental health are different depending on whether they are past the mean marriage age.
When considering only the above-the-mean-marriage-age group, the results were consistent with previous studies. In line with previous studies, this study showed an association between mood disorders, depression, and never-married status above the mean marriage age.2223242537 The benefits of marriage on mental health may be mediated through diverse mechanisms, including social support,38 access to economic resources (financial security and the “marriage premium” by which married people demand higher salary),39 and the beneficial influence of spouses on marital partners’ health behaviors.4041 In line with previous studies that have described that never-married status could increase the prevalence of anxiety disorders,4243444546 we found a significant association between the never-married people and agoraphobia and OCD in this study. Nevertheless, we should be prudent when interpreting results with large CI for agoraphobia. Because of a small number of respondents, there may be a lack of validity about the true effect. We need to assess more precisely the true association between never-married status and agoraphobia via larger sample size.
Never-married people under the mean marriage age did not exhibit significant results in most psychiatric disorders and exhibited lower ORs for GAD, alcohol use disorders, and alcohol dependence, which differed from the results of previous studies.26272847484950 These disagreements may have resulted from differences in participants and prevalence by countries; however, we could assume that never-married status does not have a significant effect on mental health in those who are under the mean marriage age. Young couples who have been married for a few years may experience significant economic pressures for some time, as they have been married with debt following their wedding (e.g., paying back home loans, installment payments for car, etc.).515253 They are likely to experience various kinds of stresses during the birth and upbringing of children,165455 which usually occurs in the early years of marriage. In this respect, the process of marriage itself can be a greater source of stress to people under the mean marriage age.
Never-married status is generally considered a risk factor for suicidality,2930 and, as predicted, never-married people above the mean marriage age exhibited an increased risk of possessing suicide attempts than married people in this study. Never-married people may be vulnerable due to a lack of the protective factors that married people usually possess, such as social and moral support,29 responsibilities toward the family, and an outlet for relieving stress.30 However, this study did not show significant outcomes between never-married status and suicidality under the mean marriage age. Moreover, when we considered only the never-married people, getting older than the mean marriage age was associated with a higher ORs of suicide ideations and suicide attempts controlling for age. Thus, these findings suggest that getting older than the mean marriage age is independently associated with suicide, and its meaning is clearly different from the previous findings that age itself is a risk factor for suicide.56575859
Never-married people above the mean marriage age are considered damaged, immature, insecure, self-centered, or unattractive.192021 These negative stereotypes and labeling can have an effect on their psychological conditions.17 Feeling deficient and inadequate for being alone for extended periods, never-married people above the mean marriage age often lose self-esteem and self-worth owing to internalizing responsibility for not being married and not belonging to a “normal” group.18 Moreover, they are vulnerable to self-blame because they get older in a culture that is primarily dominated by married people, and therefore, the ever-present isolation, emptiness, loneliness, and despair sets in and becomes a constant companion.60 Consequently, they find it easy to have thoughts of death from these feelings of shame and loneliness.6061 In this regard, a high association of suicidality may have been observed among those above the mean marriage age.
The negative impact of an individual's unmarried status on their mental health was more profound in the older-old group than in the younger-old group. In this study, unmarried status in the older-old group was significantly associated with GAD, which was consistent with previous findings.626364 Being an old never-married person could be considered “abnormal” or “different,” which can cause anxiety.60 Moreover, getting older alone without a spouse or any children is a concern for older never-married people that no one will take care of them when they become sick or are dying.65 As such, they are likely to be more vulnerable to anxiety.
In terms of suicidality, suicide ideations were significant in both younger- and older-old groups, but suicide attempts were significant only in the older-old group. Suicide attempts are the more serious form of suicidality than suicidal ideations. In this respect, the older-old group can be considered to be suffering greater psychological distress. In addition, the association between the older-old group and suicidal ideation was significant even after controlling for mental disorders, which means that relatively healthy people without mental disorders think more about suicide. Therefore, further investigation should be conducted to determine the cause of suicidal ideations in never-married people without mental disorders.
The results in this study indicate that clinicians should closely examine the suicidal thoughts and behaviors in never-married people above the mean marriage age, especially the older ones among them. Further, policymakers should strengthen support measures to improve the mental health of never-married people above the mean marriage age and develop strategies to reduce the suicide risks of those who are vulnerable.
However, there are several limitations to consider. First, as this study was based on a cross-sectional design, the causality between marital status and mental health could not be investigated. We interpreted the results to mean that having never been married increased prevalence of mental disorders, but people with poor mental health may not have been selected as partners due to the selective effects of marriage. Furthermore, we need to explore the impacts of marital status on mental disorder and suicidality through further longitudinal studies. Second, the judgment that their age is early or late for marriage and the impact of getting older than the mean marriage age alone could differ from person to person. Thus, we should be careful when generalizing the conclusions of this study. Third, this study was conducted in Korea, which is strongly influenced by Confucian culture that supports the notion that one must get married and continue a family lineage successively. However, values and attitudes toward marriage differ from country to country. Depending on the culture, exceeding the mean marriage age may not be a significant psychological burden. Nevertheless, this was the first study that analyzed the impact of getting older than the mean marriage age on mental disorders and suicidality. Moreover, the use of reliable methodology for psychiatric diagnoses in a large, nationwide representative sample enhances the validity of this study.
In conclusion, unlike those under the mean marriage age, never-married people above the mean marriage age were associated with mental disorders and suicidality. In particular, never-married people above the mean marriage age were more likely to have experienced suicidal ideations and have attempted suicide compared with those under the mean marriage age. This study demonstrates the need to address the risks of mental health and suicidality of never-married people above the mean marriage age and could be used as a basic resource for public mental health policy. Furthermore, it suggests the need for a national strategy to develop an environment where never-married people do not suffer even if their marriage is delayed.
Go to :
 XML Download
XML Download