

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Blood transfusion plays a vital role in acute hemorrhage patients.1 However, several studies have reported that the incidence of complications from blood transfusion increases mortality.2 In addition, excessive blood transfusions can lead to problems of management (lack of blood products and supply problems) as well as increased cost to the health care system.13
Although modern surgical techniques have improved in the orthopedic field, surgery for hip fractures is still associated with significant perioperative blood loss, which requires blood transfusion.4 Hip fracture itself causes many hemorrhages and is a serious injury in older patients with conditions such as anemia and lesser physiological reserves.56 Therefore, the high morbidity and mortality observed in these patients may be associated with bleeding and blood transfusion as well as underlying disease. Various studies have reported that the perioperative use of blood products is associated with postoperative morbidity and mortality.789 For this reason, various blood conservation strategies have been introduced.10 There are several reports on the incidence of transfusion in elderly patients with hip fracture.21112 However, these are small cohort studies and there are no larger studies with representative data. In addition, previous studies have focused on the cut-off value for blood transfusion to reduce complications, and management strategies to reduce blood transfusion requirements and the risk of bleeding due to factors such as aspirin or warfarin use.13
Prior to this study, a multicenter study of the Korean Hip Society reported a transfusion in Korean patients with hip fracture who had a large amount of transfusion and had a transfusion threshold of less than 10 dL/L, rather than bleeding or patient status.14
Therefore, we aimed to investigate whether blood transfusion is still performed in comparison with developed countries where patient blood management is well implemented through real world nationwide data.
Therefore, the aim of this nation-wide study was to investigate the blood transfusion status of elderly hip fracture patients and to examine the association between use of packed red blood cell (pRBC) transfusion and mortality within the first year after hip fracture surgery.
Go to : 
METHODS
Study subjects
In this cohort study, we selected subjects from the Senior Cohort of the Korean National Health Insurance Program (NHIS-Senior, NHIS-2018-2-036) collected by the Korean NHIS.
The Korean NHIS website (https://nhiss.nhis.or.kr/bd/ay/bdaya001iv.do) could be used to access the NHIS-Senior and other related cohorts. A total of 588,147 participants were randomly selected from the NHIS-Senior, using 10 percent simple random sampling from the database including around 5.5 million Korean enrollees who were older than 60 years of age in 2002. The NHIS-Senior was designed to represent the elderly people living in Korea statistically. All NHIS-Senior participants were followed up until December 31st, 2015 unless death or disqualification, such as emigration, occurred for National Health Insurance. Since the NHIS is the only single provider of the Health Insurance Service Policy universal health care program, all personal details, ages, and medical treatment data are collected and stored in the NHIS database for Korean people who have been designated as insured workers, insured self-employed persons or medical help beneficiaries.1516 The dataset included all information on ambulatory and inpatient medical claims, including codes for treatment procedures, and primary and secondary diagnosis.
Elderly hip fracture cohort
The eligibility criteria for hip fracture with elderly patients were as follows: 1) first admission (index admission) to an acute care hospital with diagnostic codes for femoral neck fractures (International Classification of Diseases, 10th Revision [ICD-10] S720) or intertrochanteric fracture (ICD-10 S721)1718; 2) at least a 3-year hip fracture-free period; 3) recipients of typical surgeries including internal fixation (open reduction of fractured extremity [femur], closed pinning [femur]), hemiarthroplasty (hip), and total arthroplasty (hip); and 4) age 65–99 years at the time of a hip fracture to assure inclusion of only osteoporotic hip fractures.18 To maintain a minimum follow-up duration of 365 days, cases with hip fracture that occurred within 365 days before the conclusion of the observation duration (December 31, 2015) were excluded. Patients with hip fracture before December 31, 2004 were also excluded to ensure a fracture-free period of at least 3 years in the hip. Hip fracture occurrence date (index date) was identified as the date of admission to the acute care hospital which met the eligibility criteria. The last follow-up date has been described as the date of death, or December 31, 2015, whichever came first.19
Volume of allogenic blood transfusion
Blood transfusion was defined as follows: 1) transfusion performed during hospitalization in an acute care hospital in which surgery was performed due to hip fracture and 2) transfusion of red blood cells (RBCs) packed in 320-mL or 400-mL units. The date of blood transfusion was set to the same day as admission for hip fracture under the assumption that a majority of the transfusion might be needed during or just after hip fracture surgery.
All-cause mortality and length of stay
Death by any cause and its date as the outcome event of this study were identified by the linkage of each subject's unique de-identified number with information provided by the Korean National Statistical Office.16 Length of hospital stay was defined as days between admission date and discharge date at the same hospital in which patients underwent hip fracture surgery.
Statistical analysis
Time zero was set to the date of the occurrence of hip fracture, and baseline characteristics were then established. For survival analysis, the measurement of the survival period was defined as the days from the date of the occurrence of hip fracture to the date of death (an event) or December 31, 2015 (censoring), whichever first occurred.
Since the surgery and blood transfusion are usually done soon after admission (due to characteristic of the hip fracture), the date of transfusion was set at the same date (time zero) as that of the hip fracture. The cumulative probabilities of survival were calculated using the Kaplan-Meier method with a product-limit formula, and a survival curve was plotted. The log-rank test was used to compare survival curves, under the null hypothesis of a common survival curve. To control the effects of potential confounders, a multivariate-adjusted Cox proportional hazards model investigated the effects of transfusion on all-cause mortality. In addition, the hazard ratio (HR) was determined according to the four blood volume classes, with all baseline characteristics changed. Effect sizes were shown as HRs and 95% confidence intervals (CIs).
The covariates included age group, gender, household income level, residential area, Charlson Comorbidity Score (CCS), type of fracture, type of procedure, forms of anesthesia, number of hospital days and calendar year of occurrence of hip fracture. The number of comorbidities of each subject was measured using the Quan ICD-10 coding algorithm of the CCS by diagnostic codes during the 3 years preceding the index date.20 At least two outpatient visits or one admission upon primary or first secondary diagnosis established the existence of CCS disease-constituting categories. In addition, we classified patients into three subgroups to determine the relationship between blood transfusion volume and mortality, considering clinical settings and statistical distribution. All statistical research was performed using version 7.1 of the SAS Enterprise Guide (SAS Institute, Cary, NC, US). P values < 0.05 had been found statistically significant.
Ethics statement
The protocol of this study was approved by the Institutional Review Board of Eulji University Hospital (No. EMC 2019-02-001-001). Informed consent was waived due to the retrospective nature of this study.
Go to :
RESULTS
Between January 1, 2002 and December 31, 2014, a total of 18,448 hip fracture patients were admitted to hospitals and received surgery. The 2,108 patients who first developed a hip fracture before December 31, 2004 were excluded to make sure of at least a 3-year hip fracture-free period. Additionally, 90 patients under 65 or over 99 years of age and 1,506 patients whose index date was within 365 days prior to December 31, 2015, were excluded. Finally, 14,744 patients were enrolled in the cohort as elderly hip fracture patients (Table 1). There were 10,973 patients (74.42%) in the transfusion group and 3,771 (25.58%) patients in the non-transfusion group. The mean age in the transfusion group was 80.28 (± 6.64) years and the number of women was 8,434 (76.86%). The mean volume of blood transfusion was 1,164.51 mL (± 865.25; median, 800 mL; interquartile range [IQR], 640–1,440). The mean age in the non-transfusion group was 78.24 (± 6.60) years and the number of women were 2,618 (69.42%). There were statistical differences in age, sex, income, residential area, anesthesia, and hospital days between the two groups (P < 0.05). The mean hospital stay in the transfusion group was significantly longer than in the non-transfusion group (32.29 ± 26.25 days vs. 27.59 ± 21.66 days, P < 0.001).
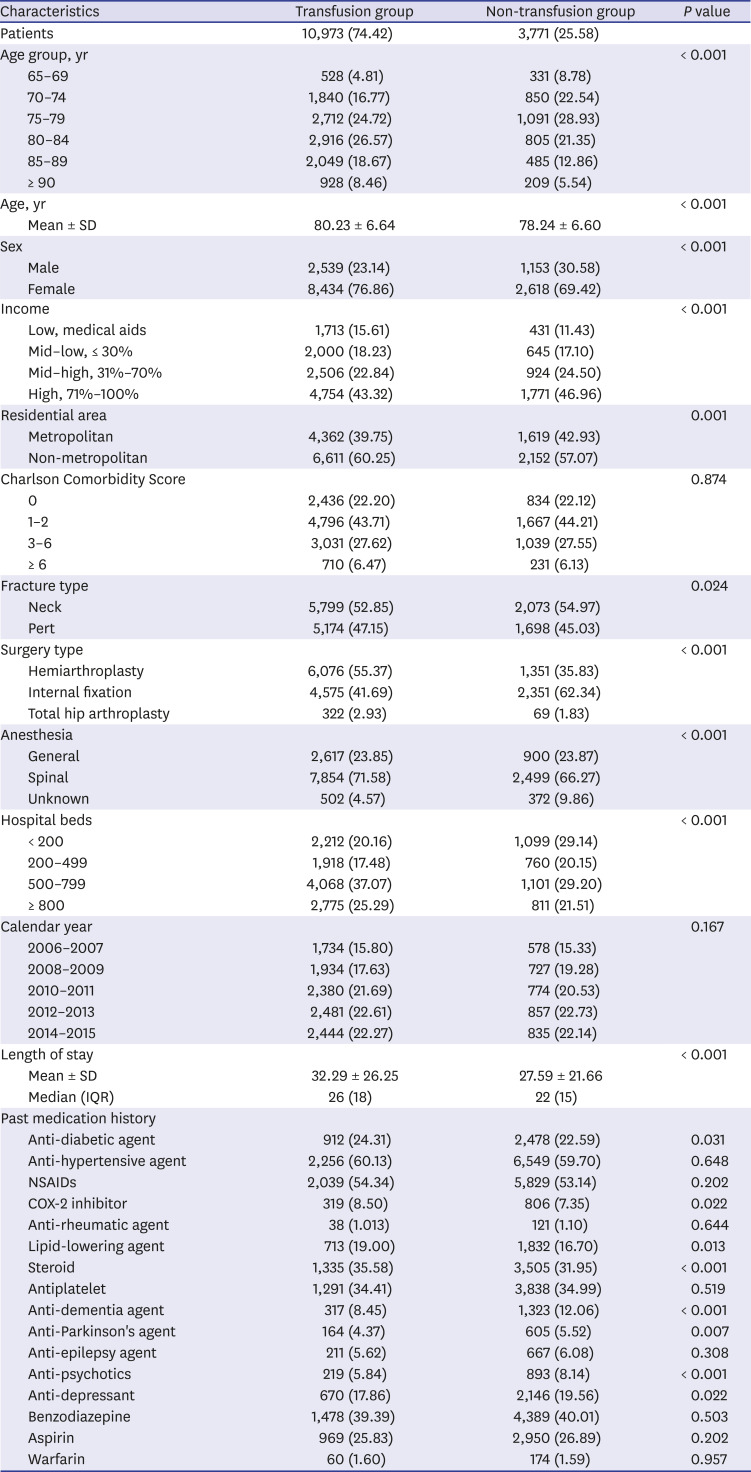
Table 1
Baseline characteristics of study participants
Data are presented as number (%) unless otherwise indicated.
SD = standard deviation, IQR = interquartile range, NSAID = nonsteroidal anti-inflammatory drug, COX-2 = cyclooxygenase-2.
![]()
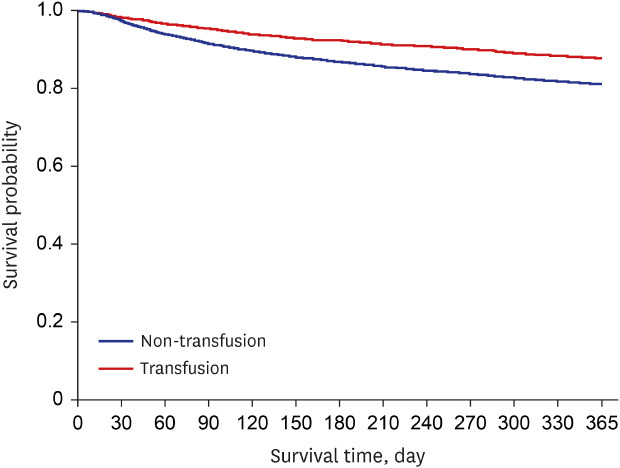
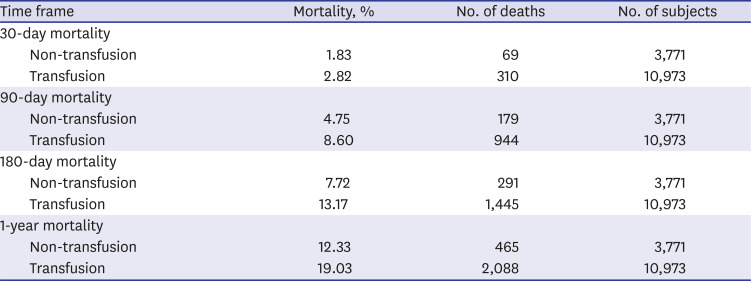
Mortality rates in the transfusion group and non-transfusion group were 15.24 and 10.31 per 100 person-years, respectively (Table 2). In the multivariable-adjusted Cox proportional hazard model, the transfusion group had 1.34-fold more hazard of all-cause mortality than the non-transfusion group (adjusted HR, 1.34; 95% CI, 1.26–1.42). The difference in the mortality rate between the two groups occurred rapidly within 1 year after surgery (Fig. 1). Median survival time was 1,714 days for the transfusion group and 2,532 days for the non-transfusion group. Three-hundred and ten (2.82%) patients in the transfusion group died within 30 days versus 69 (1.83%) patients in the non-transfusion group (Table 3).

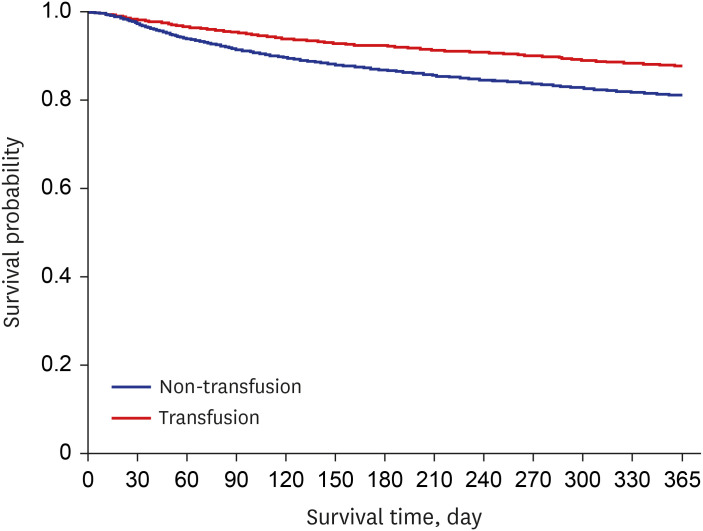 | Fig. 1Kaplan-Meier curve of hip fracture patients according to transfusion status. The P value of the log-rank test was < 0.001.
|
Table 2
Mortality rate and comparison of hazard for death according to transfusion
aHR = adjusted hazard ratio, CI = confidence interval.
Adjusted for age group, sex, income level, residential area, Charlson Comorbidity Score, surgery type, fracture type, anesthesia type, hospital beds, and calendar year.
aCases per 100 person-years.
![]()
Table 3
Cumulative mortality according to the presence of transfusion
![]()
Go to :
DISCUSSION
The incidence of hip fracture is increasing worldwide, along with the increase in the osteoporotic elderly population.2122 Most hip fractures require surgery and more medical resources for recovery compared to other orthopedic surgeries.23 Anemia may delay functional recovery and lead to longer hospital stays and greater cost for elderly patients.242526 Thus, blood transfusions are commonly administered to treat bleeding and anemia after surgery.27 However, it does not always produce good results. Transfusion may increase the rate of complications such as risk of tumor recurrence, post-operative infection, and acute lung injury.28
The principle finding of this study was that 74.42% of all hip fracture patients received transfusions during hospitalization. The mean hospital stay in the transfusion group was significantly longer than that in the non-transfusion group. The risk of death increased as the amount of blood transfusion increased during the hospital stay. The mortality risk in the transfusion group was higher than that in the non-transfusion group within 1 year after hip surgery.
However, several previous studies on the relationship between transfusion and death reported contrasting results to this study. Engoren et al.27 reported a small cohort study of 229 hip fracture patients. They showed that transfusion was not a predictor of 30- and 90-day mortality, but transfusion patients who survived at 90 days after surgery had higher mortality than non-transfusion patients. Also, among transfused patients in a retrospective cohort study of 8,787 consecutive hip fracture patients, mortality was 5.3% at 30 days compared with 4.0% in the non-transfused patients.29 An HR of 1.34 was found at 90 days; however, after multivariable adjustment, transfusion was not a significant predictor of 30- or 90-day mortality. In addition, in the study of Johnston et al.,30 mortality was higher at 120 and 365 days by univariable analysis, but not at 30 days, in patients receiving transfusion. After multivariable adjustment, transfusion was no longer a statistically significant predictor of death. However, these studies seem to be limited by small cohorts, retrospective study design, or selection bias. Differences between Western and Asian populations also may have affected the relationship between mortality and transfusion.
Morris et al.2 reported transfusion rates of 39.4% for intertrochanteric fracture and 22.5% for neck fracture. Carson et al.29 reported a 42.1% blood transfusion rate in hip fracture patients over 60 years of age. Kadar et al.13 reported that 39% of hip fracture patients received transfusions within 72 hours after surgery, and additional blood transfusion was performed in 20% of the patients after 72 hours. Although these studies reported high blood transfusion rates, this study showed the highest rate at 75%. Various factors can influence the amount of blood transfusion. A high blood transfusion rate can be seen if the operation time is long, preoperative anemia is severe, or the period before surgery is long. The amount of transfusion may also be altered by fracture type (neck fracture, intertrochanteric fracture), surgery type (internal fixation, hemiarthroplasty, total hip arthroplasty), or implant type (dynamic hip screw, intramedullary nail).2 Most studies have not analyzed preoperative anemia and patient demographic data also differed. Morris et al. reported a mean operation time of about 30 minutes, but Kadar et al.13 reported an average operation time of 107.4 minutes. These differences may be the cause of the variations in blood transfusion rates.
The study involved several limitations. First, preoperative anemia status was not considered, because the study was based on the National Claims Registry. Second, mortality due to a specific medical condition or non-medical usage was not analyzed. However, we tried to overcome these two problems through multivariate-adjusted regression models including age, gender, Charlson Comorbidity Index, etc. Third, the use of other transfusion agents such as platelet concentrates or fresh frozen plasma was not considered. However, since platelet concentrates and fresh frozen plasma are transfused without pRBCs only in patients with a specific disease, pRBCs may be used as representative data for presenting the amount of blood transfusion in elderly hip fractures. Fourth, we were unable to adjust for hemoglobin levels after hip fracture surgery in this study. Patients who received blood transfusions had more blood loss during the operation, so they could not explain the direct causal relationship between death and blood transfusions. Large well-designed randomized controlled trials need to be implemented to analyze the causal relationship between blood transfusion and death. Fifth, we did not analyze the effects of blood transfusion before and after surgery, respectively. Finally, there was no evidence that the blood transfusion affected postoperative clinical condition. Therefore, prospective large cohort studies will be needed because that analysis was performed with a disease code.
In this nationwide representative cohort study, RBC transfusion was performed in 75% of hip fracture patients. Even after adjusting for comorbidity and anticoagulant use, the postoperative results (hospitalization, mortality) of the transfusion group did not show significantly better results than the non-transfusion group. Therefore, adequate patient blood management can only improve the patient's outcome after hip fracture surgery.
Go to :
 XML Download
XML Download