

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Blood pressure (BP) is a well-known risk factor for cardiovascular (CV) complications and renal progression in chronic kidney disease (CKD).1 The 2017 American College of Cardiology/American Heart Association (ACC/AHA) hypertension (HTN) guidelines recommend a target BP in CKD patients less than 130/80 mmHg for complicated HTN associated with CKD or diabetes mellitus (DM) and for uncomplicated HTN.2 The 2018 European Society of Cardiology/European Society of Hypertension (ESC/ESH) guidelines recommend that systolic BP (SBP) in both the high- and low-risk groups be below 140 mmHg.3 Reference studies on these HTN guidelines were mainly conducted from the perspective of CV morbidity and mortality, and renal progression has received comparatively little attention.4
In recent years, several studies have analyzed the effect of maintaining SBP below 120 mmHg on the preservation of renal function, and meaningful comparisons of the results against protocols using existing HTN guidelines are available.5678910 The authors used a national health screening database, which are rare in other countries, to investigate the effects of BP on renal function decline by tracking for 6 years more than 5 million Korean adults with normal renal function (NRF) and no proteinuria at the beginning of the study.
METHODS
Data
This retrospective observational study uses big data from the national health screening database provided by the Korean National Health Insurance Service (NHIS) through the National Health Insurance Sharing Service (http://nhiss.nhis.or.kr). The NHIS is a government-affiliated agency and the only insurance provider of the national health insurance system operated by the Korean government. It provides health screening every other year to all citizens older than 20 years through verified hospitals and clinics nationwide. However, national health screening is an option and not mandatory although it is free. The health screenings provide researchers with standardized and encrypted epidemiologic and laboratory databases covering 41 major items.
Study population
Korean adults older than 20 years in 2009 who participated in the national health screenings provided by the NHIS in both 2009 and 2015 were included in this study. Subjects with estimated glomerular filtration rate (eGFR) less than 60 mL/min/1.73 m2 or proteinuria exceeding a trace amount were excluded, as were those for whom data were missing.
Definitions and measurements
Health screening was conducted in Korean hospitals and clinics certified by the NHIS. The baseline data for this study were obtained from screenings conducted in 2009. A questionnaire was used to obtain epidemiological data on age, sex, smoking, drinking, exercise, income, and history of medical illnesses, such as HTN, DM, and dyslipidemia. The age of the subjects, based on the resident registration number, was used to divide the subjects into 3 age categories: 20–39 years (youth), 40–64 years (middle-aged), and 65 years or older (old age). The physical examinations measured SBP, diastolic BP (DBP), height, weight, and waist circumference (WC). BP was measured in the brachial artery using an automatic sphygmomanometer with the subject in a sitting position after 2 to 5 minutes of rest. Trained medical practitioners such as nurses guided and supervised the entire BP measurement process. We repeated a measurement when the first exceeded 120/80 mmHg. WC was measured at a point equidistant from the lowest position of the ribs and the highest position of the pelvis. Body mass index (BMI) was calculated by dividing the subject's weight (kilograms) into the square of height (meters). Blood tests for serum creatinine, glucose, total cholesterol, and urinary protein were performed after fasting for at least 8 hours. eGFR was calculated by the Modification of Diet in Renal Disease formula (175 × serum creatinine−1.154 × age−0.203 × 0.742 for female).
Smoking status was defined based on a current smoking habit regardless of amount, and over-drinking was defined as an intake of 30 g or more of alcohol per day. Income level was divided into quartiles and then divided into 2 categories of quartile (Q) 1 and Q2–4. HTN, DM, and dyslipidemia status were defined based on indications of such past medical histories; related medication status on the survey; or a BP of 140/90 mmHg or higher, fasting sugar of 126 mg/dL or higher, and total cholesterol of 240 mg/dL or higher in the 2009 health screening. Exercise was divided into existence and absence of regular exercise, which was defined as more than 20 minutes of intense exercise more than 3 days a week or more than 30 minutes of moderate exercise more than 5 days a week. Obesity was defined as a BMI of 25 kg/m2 or higher. Abdominal obesity was defined by a WC greater than 85 cm for female and 90 cm for male.
To confirm impairment of renal function in the same subjects, eGFRs were measured again using the serum creatinine value in 2015, 6 years after the start of the study. The subjects were divided into an impaired renal function (IRF) group and a NRF group according to the eGFR in 2015. NRF was defined as cases in which eGFR was 60 mL/min/1.73 m2 or more, and IRF was defined as cases in which eGFR was less than 60 mL/min/1.73 m2. The effects of epidemiological factors, BP, and laboratory findings on renal progression were investigated. The subjects were categorized according to BP status in 10 mmHg intervals. SBP was divided into 8 categories (< 100, 100–109, 110–119, 120–129, 130–139, 140–149, 150–159, and ≥ 160 mmHg), DBP was divided into 7 categories (< 60, 60–69, 70–79, 80–89, 90–99, 100–109, and ≥ 110 mmHg), and pulse pressure (PP) was divided into 4 categories (< 45, 45–54, 55–64, and ≥ 65 mmHg).
Statistical analysis
To analyze the underlying characteristics of all subjects and to compare those characteristics according to occurrence of IRF, study subjects were divided into IRF and NRF groups. Significance verification for correlation between occurrence of IRF and age group was indicated by number of people (%) and P value through analysis of variance. Correlation between occurrence of IRF and variables other than age was indicated by number of people (%) and P value through a χ2 test. The result of comparison between the two groups was presented as mean ± standard deviation and P value through Student's t-test. The comparison of IRF and total population according to BP after correcting other variables was indicated by number of people and odds ratio (OR) (95% confidence interval [CI]) by logistic regression. To analyze the relationship between BP and IRF occurrence in depth, a multivariate logistic regression analysis was performed for 11 confounding variables of age, sex, smoking, drinking, exercise, income, BMI, DM, HTN, dyslipidemia, and eGFR. Subgroup analysis was performed on 8 variables of age, sex, DM, HTN, obesity, abdominal obesity, eGFR, and smoking. Statistical analysis was performed using SAS, version 9.4 (SAS Institute, Inc, Cary, NC, USA) at The Catholic University of Korea.
RESULTS
Baseline characteristics
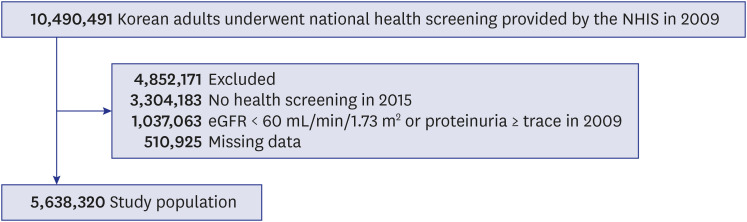
In the health screening conducted in 2009, 10,490,491 subjects were older than 20 years. Among them, 1,037,063 did not meet the eGFR or proteinuria criterion, 510,925 had missing data, and 3,304,183 were not examined in 2015. A total of 5,638,320 subjects was selected as the study population (10,490,491 − 1,037,063 − 510,925 − 3,304,183 = 5,638,320) (Fig. 1).
The baseline characteristics for the 5,638,320 subjects at the beginning of the study were as follows: mean age, 46.29 ± 12.52 years; female, 42.60%; smoker, 26.37%; HTN prevalence, 23.13%; DM prevalence, 7.17%; mean BP, (121.99 ± 14.36)/(76.24 ± 9.76) mmHg; and eGFR, 90.86 ± 42.98 mL/min/1.73 m2. Other baseline characteristics are presented in Table 1.
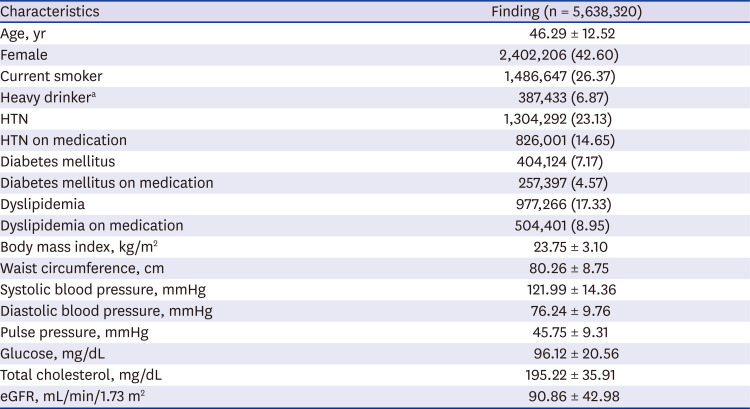
Table 1
Baseline characteristics
Data are presented as mean ± standard deviation or number (%).
HTN = hypertension, eGFR = estimated glomerular filtration rate.
aHeavy drinking is defined as alcohol consumption ≥ 30 g/day.
![]()
Comparison between IRF and NRF groups
After 6 years of study, 161,044 (2.86%) of the original subjects had IRF (Fig. 2). All subjects were divided into IRF and NRF groups, and the clinical factors at baseline were compared between two groups (Table 2). The IRF group showed larger proportions of both elderly (65 years or older) and female compared with the NRF group (P < 0.001), and the prevalence of HTN, DM, and dyslipidemia was also higher (P < 0.001). In addition, eGFR was lower in the IRF group than in the NRF group (79.42 ± 36.02 mL/min/1.73 m2 vs. 91.2 ± 43.17 mL/min/1.73 m2, P < 0.001), and smoker and over-drinker proportions were lower (smoker, 16.4% vs. 26.66%, P < 0.001; over-drinker, 4.38% vs. 6.94%, P < 0.001). Values for SBP, DBP, and PP were compared between the two groups without considering whether an antihypertensive drug has been administered, and the IRF group had higher SBP, DBP, and PP compared with the NRF group (P < 0.001).
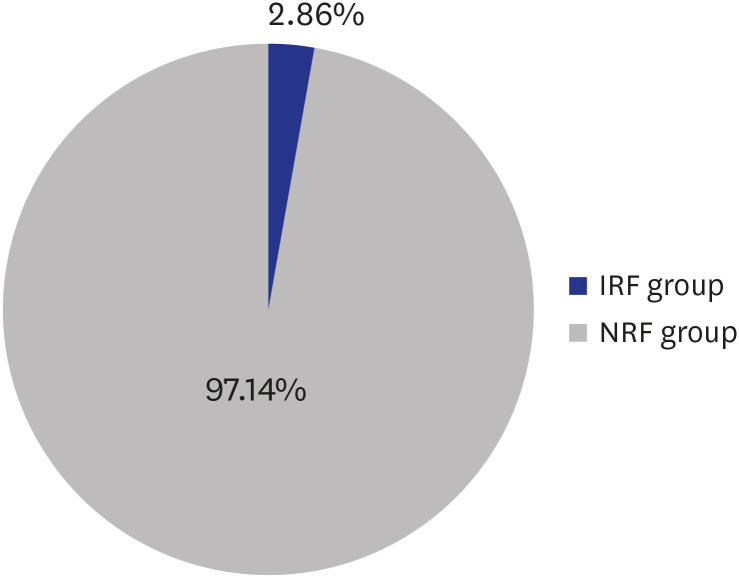
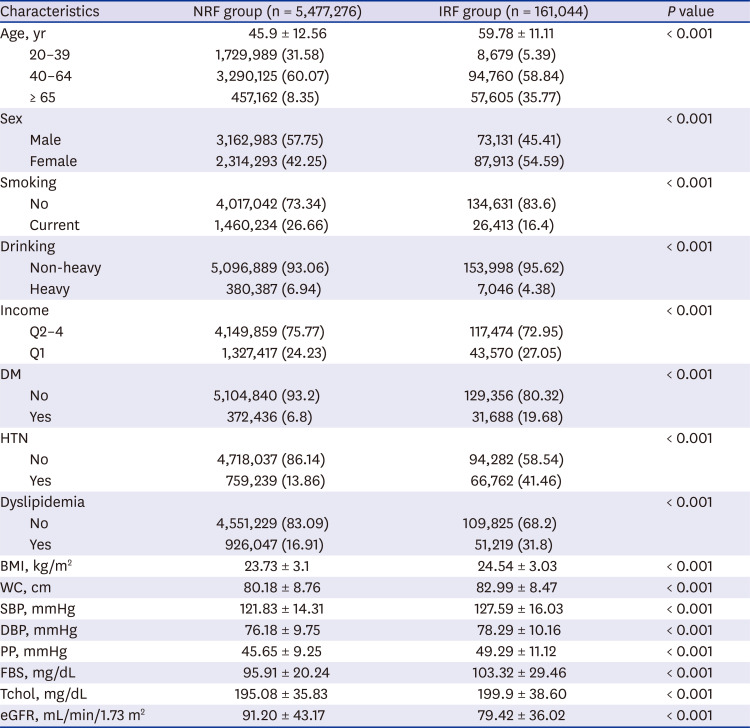
Fig. 2
IRF incidence in 2015 after 6-years of follow-up.
IRF = impaired renal function, NRF = normal renal function.
![]()
Table 2
Comparison between IRF and NRF groups
Data are presented as mean ± standard deviation or number (%).
IRF = impaired renal function, NRF = normal renal function, Q = quartile, DM = diabetes mellitus, HTN = hypertension, BMI = body mass index, WC = waist circumference, SBP = systolic blood pressure, DBP = diastolic blood pressure, PP = pulse pressure, FBS = fasting blood sugar, Tchol = total cholesterol, eGFR = estimated glomerular filtration rate.
![]()
Renal progression according to BP
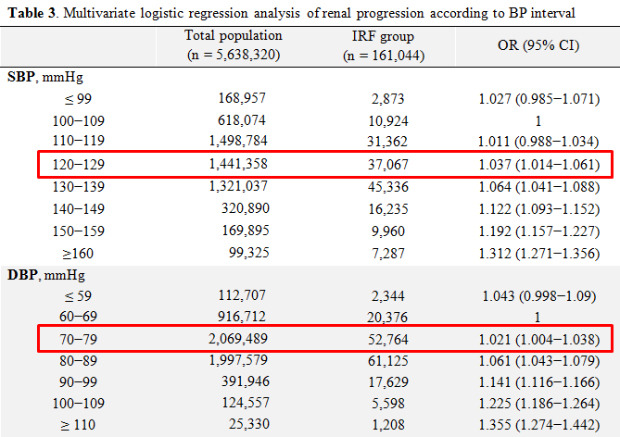
To investigate the effects of SBP, DBP, and PP on occurrence of IRF, the three pressures were divided into 8, 7, and 4 categories, respectively (Table 3). Adjustments were made for 11 confounding variables of age, sex, smoking, drinking, exercise, income, BMI, DM, HTN, dyslipidemia, and eGFR. The reference intervals were set as 100–109 mmHg for SBP, 60–69 mmHg for DBP, and 45–54 mmHg for PP, and the ORs of IRF occurrence at each BP category were calculated.
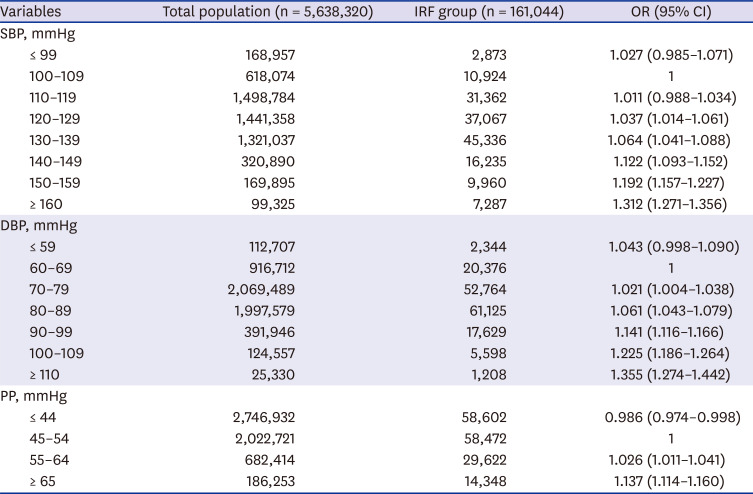
Table 3
Multivariate logistic regression analysis of renal progression according to blood pressure interval
Data are presented as OR (95% CI) or number.
Adjusted by age, sex, smoking, drinking, exercise, income, body mass index, diabetes mellitus, hypertension, dyslipidemia, and estimated glomerular filtration rate.
IRF = impaired renal function, OR = odds ratio, CI = confidence interval, SBP = systolic blood pressure, DBP = diastolic blood pressure, PP = pulse pressure.
![]()
The OR of IRF occurrence according to SBP was not statistically different in either the ≤ 99 mmHg interval or the 110–119 mmHg interval compared with the reference interval of 100–109 mmHg. The OR was statistically significant (OR, 1.037; 95% CI, 1.014–1.061) from the 120–129 mmHg interval, and as SBP increased, the OR increased (130–139 mmHg, OR, 1.064, 95% CI, 1.041–1.088; 140–149 mmHg, OR, 1.122, 95% CI, 1.093–1.152; 150–159 mmHg, OR, 1.192, 95% CI, 1.157–1.227; ≥ 160 mmHg, OR, 1.312, 95% CI, 1.271–1.356).
The OR of IRF occurrence according to DBP was not statistically different in the ≤ 59 mmHg interval compared with the reference level of 60–69 mmHg. The OR was statistically significant (OR, 1.021; 95% CI, 1.004–1.038) for the 70–79 mmHg interval, and as DBP increased, the OR increased (80–89 mmHg, OR, 1.061, 95% CI, 1.043–1.079; 90–99 mmHg, OR, 1.141, 95% CI, 1.116–1.166; 100–109 mmHg, OR, 1.225, 95% CI, 1.186–1.264; ≥ 110 mmHg, OR, 1.355, 95% CI, 1.274–1.442).
On the other hand, for PP, the OR of IRF occurrence was statistically significantly lower in the ≤ 44 mmHg interval compared with the reference interval of 45–54 mmHg, and the OR was statistically significantly higher (55–64 mmHg; OR, 1.026; 95% CI, 1.011–1.041) for the 55–64 mmHg interval. As PP increased, the OR increased (≥ 65 mmHg; OR, 1.137; 95% CI 1.114–1.16).
The risk of IRF occurrence was measured by subgroup analysis of 8 significant risk factors for CKD of age, sex, DM, obesity, abdominal obesity, eGFR, and smoking according to SBP, DBP, and PP intervals (Supplementary Fig. 1). The risk of IRF occurrence gradually increased with SBP, DBP, and PP intervals in most subgroups but was significantly higher in some subgroups at the highest blood pressure (≥ 160 mmHg of SBP, ≥ 110 mmHg of DBP). The risk of IRF occurrence in the 20–39 year age group was significantly higher at SBP ≥ 160 mmHg and DBP ≥ 110 mmHg (SBP OR, 1.917, 95% CI, 1.609–2.285; DBP OR, 1.725, 95% CI, 1.357–2.193), and risk for smokers was also significantly higher (SBP OR, 1.518; 95% CI, 1.402–1.644). In addition, the male subgroups showed very high risks (OR, 1.580; 95% CI, 1.458–1.712) in the DBP ≥ 110 mmHg interval, although there was no statistical significance in female (OR, 1.099; 95% CI, 0.995–1.215).
DISCUSSION
This study investigated the incidence of IRF over a 6-year period according to the initial BP status of 5.6 million Korean adults who had no proteinuria and NRF, using national health screening data. Although 6 years of follow-up is a relatively brief period, this is the first study to investigate the effect of BP on IRF in more than 5 million adults with NRF. The results show that the incidence of IRF was 2.86% after 6 years. Subjects with an SBP of 120 mmHg or more had a higher risk of IRF than those with an SBP of less than 120 mmHg, and members of the group with a DBP of 70 mmHg or more had higher risk of IRF than those with DBP less than 70 mmHg. In addition, the incidence of IRF increased as SBP and DBP increased regardless of DM, obesity, smoking, and dyslipidemia, which are known risk factors for CKD. Therefore, BP is an important factor for IRF in Korean adults who maintain NRF. If BP is actively controlled, it may be possible to reduce the incidence of CKD. Research is needed to explore this issue.
The target BP for HTN treatment is somewhat different according to HTN guideline. To summarize, the 2017 ACC/AHA guidelines2 recommend a target BP < 130/80 mmHg, and the 2018 ESC/ESH guidelines3 recommend a target SBP < 140 mmHg. These guidelines are based largely on studies conducted from a CV rather than a renal perspective.23 This study used national health screening data for 5.6 million healthy adults, and in the initial data collection, only HTN, DM, dyslipidemia, and obesity were investigated, while history of heart disease was not identified. In addition, CV morbidity and mortality were not investigated during the study period. Of course, this could not preclude the BP effect on CV events in our study. However, we tried to focus more on the renal effects than the CV effects of BP through these controls.1112
There is some disagreement in the literature concerning the effect of BP on development of CKD in adults who maintain NRF. In a study by Yu et al.,5 14,854 adults with baseline eGFR ≥ 60 mL/min/1.73 m2 were followed up for 30 years to investigate the effect of the initial BP on CKD. The result was similar to that of the present study, as baseline HTN was associated with faster decline in renal function compared with normal BP (SBP < 120 mmHg and DBP < 80 mmHg). However, Beddhu et al.6 reported different results. They extracted 11,026 adults with baseline eGFR ≥ 60 mL/min/1.73 m2 from the Systolic Blood Pressure Intervention Trial (SPRINT)13 and the Action to Control Cardiovascular Risk in Diabetes trial14 and divided them into an intensive target group with SBP < 120 mmHg and a standard target group with SBP < 140 mmHg and compared the risk of CKD by BP control. Their conclusion was that intensive lowering of SBP increased the risk of CKD in people with and without DM, and the absolute risk was higher in DM.
In the present study, the frequencies of elderly; female; and those with HTN, low income, dyslipidemia, obesity, and DM, which are established risk factors for CKD, were significantly higher in the IRF group than in the NRF group. However, drinking and smoking frequencies were significantly lower in the IRF group than in the NRF group. The exact reason is unknown, but drinking and smoking are more commonly reported in young male who maintain NRF.
The first limitation of this study is that the data were collected only at the beginning and end of the study to maximize the size of study population, because the number of subjects who received regular screenings consecutively was lower than expected. Second, some subjects with glomerulonephritis or polycystic kidney disease may be misclassified into the NRF group because the national health screening database does not include hematuria and renal structural abnormality data. Third, some subjects, especially those with borderline results, can be misclassified because all laboratories participating in the national health screening at various hospitals and clinics nationwide have slightly different normal ranges and are not validated uniformly as with a central laboratory evaluation. Fourth, it was not possible to confirm various events and deaths that cause acute renal failure, such as heart disease and acute infectious disease, during the study period.
One of the most important considerations, although easy to overlook, is that BP measurement methods affect BP values; manual BPs are usually higher than automated BPs.15 In the SPRINT study that had a major impact on the 2017 ACC/AHA guidelines, the average of several BP values measured by the patient alone using an automated BP device was used, which was not the standard method in most clinics. This was one of the reasons why the 2017 ACC/AHA Guidelines Committee chose an SBP goal of < 130 mmHg rather than < 120 mmHg, the intensive goal of the SPRINT study. As our research was based on automatic BP measurements, we recommend considering a difference of about 10 mmHg when applying manual BP measurements.
In conclusion, HTN is an important risk factor for renal progression in Korean adults who maintain NRF, and a normal range of BP may reduce the incidence of CKD in the general population. A prospective randomized controlled study should be carried out to verify this conclusion.
 XML Download
XML Download