

 PDF
PDF Citation
Citation Print
Print



I. INTRODUCTION
Despite the development of medical science, as the complexity of our society increases, various microorganisms that have the potential to be infectious agents constantly threaten humanity. Through accumulated mutation, even well-known microorganisms are becoming new species, resulting in stronger transmission or higher number of fatalities. Korea is also in a situation where management is required of both the interior spread and the foreign inflow of various infectious diseases. For examples of the former in Korea, there are respiratory-mediated infectious diseases, such as tuberculosis, which is known to be endemic, and blood-mediated infectious diseases, such as hepatitis B, hepatitis C, and acquired immune deficiency syndrome (AIDS), which need continuous monitoring.12 Numerous foreign infectious diseases are newly emerging as a result of changes in climate and biological distribution due to environmental degradation, and the collapse of interspecies barriers. As international exchange increases, they can flow into other countries at any time.3
Recently, several respiratory diseases caused by novel viruses, such as severe acute respiratory syndrome (SARS) in 2002, novel influenza A (H1N1) in 2009, and Middle East respiratory syndrome (MERS) in 2015, were introduced worldwide. This year, on March 11, the World Health Organization (WHO) declared a global pandemic of coronavirus disease 2019 (COVID-19). A “highest” level of crisis alert was issued in Korea on February 23 based on the judgment that the spread of the disease within the local community had begun. As of May 27, 2020, about 5 million COVID-19 patients had been reported in 215 countries, resulting in 348,836 deaths, while 11,265 patients and 269 deaths had been reported in Korea.4
In a situation where enormous social and economic losses are caused by the periodic outbreak of novel infectious diseases, the national quarantine system requires improvement to cope with the public health crisis. We believe that autopsy can provide the basic data for establishing appropriate quarantine and preventive measures. The autopsy is the most direct approach to a disease or other medical abnormalities. Historically, a wide range of information on pathogenesis, epidemiology, and the natural course of numerous diseases has been collected through autopsy, leading to the development of medicine. Also, the autopsy identifies legal problems related to death and prevents potential disputes, the necessity for which has been recognized across many sectors of society. It should be considered more important in a death related to an infectious disease.
While the clinical environment is ready for infectious diseases under administrative and financial support, the death investigation system in Korea does not seem to be comparable. Although many infectious diseases are diagnosed only postmortem through autopsy, the personnel related to the autopsy are exposed to the risk of infection, due to insufficient clinical information, lack of facilities or equipment for protection, and injury accidents.
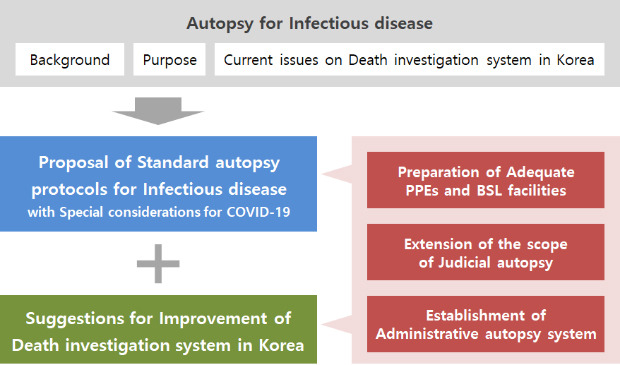
Therefore, a guideline for the standard autopsy for infectious diseases is stated here, which aims to: 1) provide scientific grounds to establish appropriate plans for the prevention and treatment of infectious diseases, 2) contribute to improving national health by controlling the spread of pathogens within the community, and 3) protect human resources engaged in autopsy-related work from the risk of infection. Several autopsy guidelines, including more recent ones focusing on COVID-19, have been adopted here.56789 Most of them suggest that the principles of handling COVID-19 during autopsy are not different from that of the handling of other infectious diseases. This guideline does not present the current modus operandi, but indicates the way in which we need to operate from now on, and which needs our continuous effort dedicated to forensics, as well as support from the related social systems.
Go to : 
II. OVERVIEW OF INFECTIOUS DISEASE AND ITS AUTOPSY
1. Background
1) General classification
The pathogen of infectious diseases includes various microorganisms, such as bacteria, viruses, fungi, parasites, and even prions. Among various routes of transmission, direct contact of blood or body fluids, and aerosol transfer via droplet or its nuclei are considered as important during the autopsy. Patients with active infection could have symptoms of acute, subacute, or chronic status, which is called clinical disease, or have no apparent symptoms, which is called subclinical or occult disease. Infection by some agents could be inactive for a certain period, which is called latent infection.
2) Diagnostic clues during the autopsy
The diagnosis of an infectious disease could be considered based on 1) medical history, from the statements of his or her acquaintances or formal medical records; 2) postmortem tests for the detection of microorganisms, such as serologic, genetic, or culture tests using blood, secretion, fluid, or tissue; 3) pathologic findings, using conventional and special stains; and 4) epidemiologic information about the deceased or his or her close contacts, such as the location of residence and workplace, occupation, travel history, and recent whereabouts.
3) Regulations associated with the infectious diseases in Korea
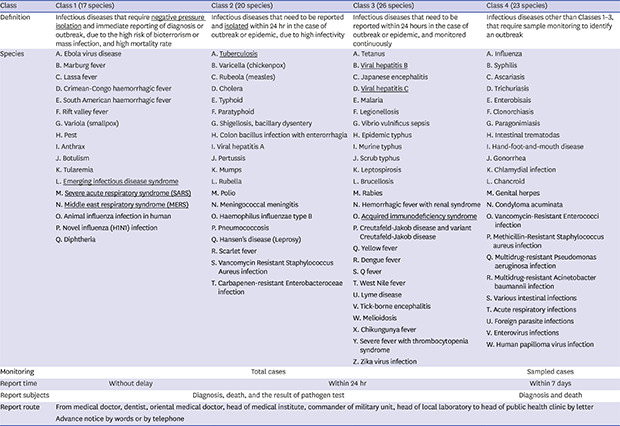
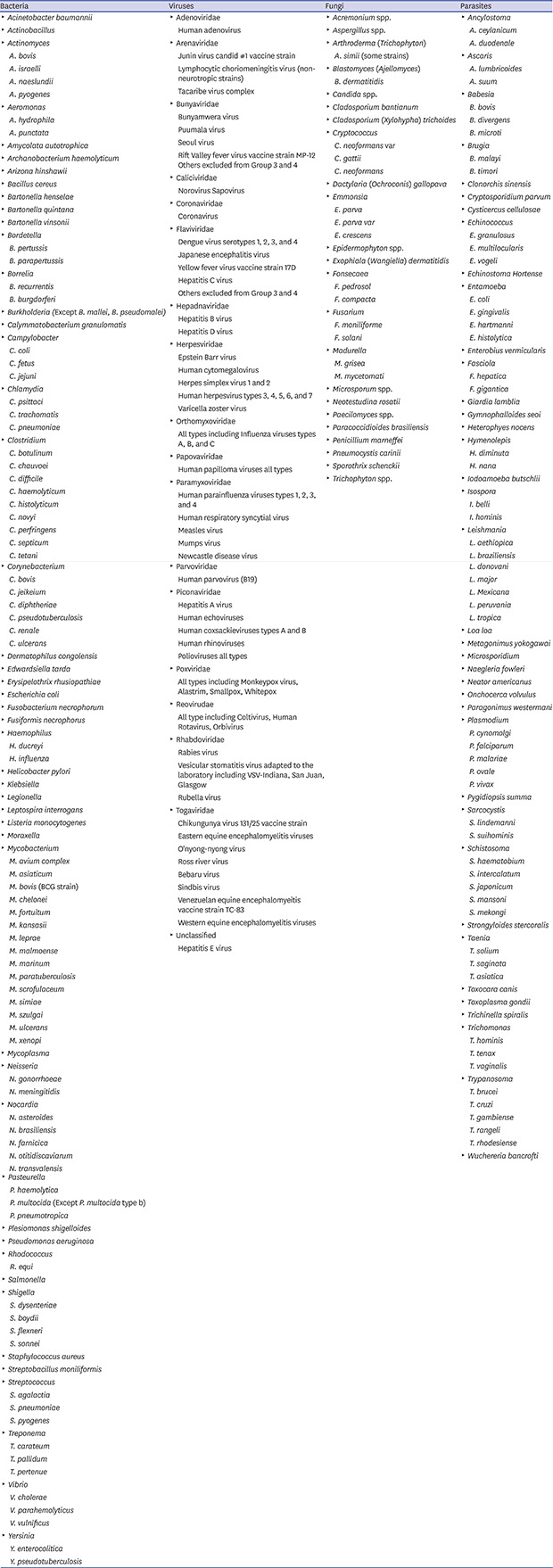
The Infectious Disease Control and Prevention Act of Korea designated some infectious diseases with epidemiologic importance as ‘legal infectious diseases.’ These diseases were classified into four classes according to their severity, infectiousness, and isolation level (Appendix 1). An emerging infectious disease with the possibility of severe symptoms or rapid transmission is considered an ‘emerging infectious disease syndrome’ in Class 1. COVID-19, caused by SARS-CoV-2, is an example of this temporary classification, which should be classified properly after the pathogenesis and clinical features are further revealed.
According to the act, a doctor who identified an infectious disease from a living patient or a dead body should report to the regional public health center. The director of the Korea Centers for Disease Control and Prevention (KCDC) may order an autopsy of the deceased who is suspected of having died from an infectious disease, to confirm the final diagnosis. The autopsy process should be conducted by a specialist in infectious disease, human anatomy, pathology, or forensic medicine, in a facility with an adequate level of biosafety.
4) Risk group classification of the infectious agents
The KCDC has suggested a revised classification of the risk groups of infectious agents (Appendix 2) in 2016, which is based on the classification for the biology laboratory published by the WHO in 2004.10 According to this classification, Risk Group 2 includes the pathogens that are unlikely to be a serious hazard, such as HBV and HCV, while Risk Group 3 includes the pathogens that usually cause serious diseases, such as Mycobacterium tuberculosis, SARS-CoV, and HIV. For both groups, effective treatment and preventative measures are available in general.
5) Biosafety level required for handling high-risk agents
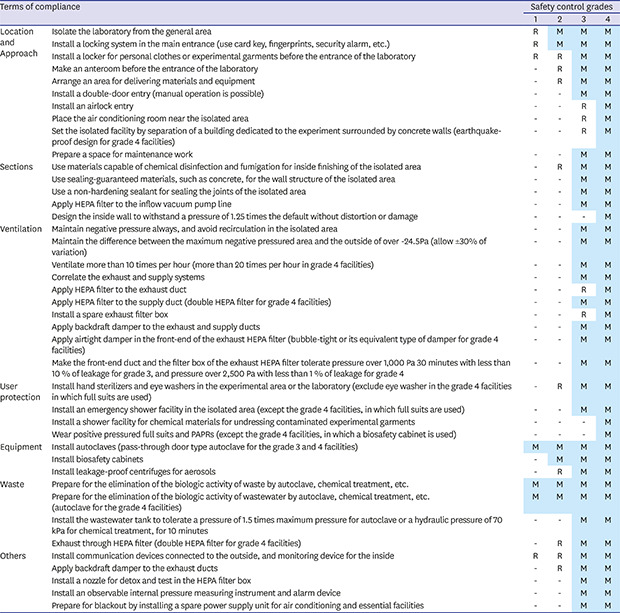
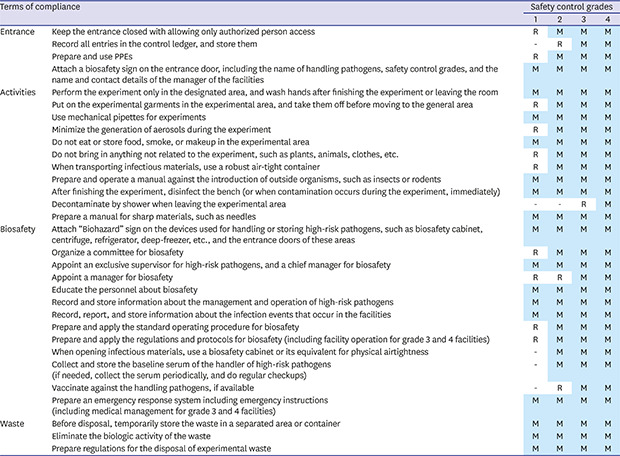
The Infectious Disease Control and Prevention Act of Korea classifies the safety control measures of the facilities handling high-risk pathogens into four grades (Appendix 3), which correspond to the biosafety levels (BSLs or BLs) suggested by the WHO. They could be applied to all the pathogens identified so far. Registration with the KCDC is required for handling high-risk pathogens of Grade 1 and 2, while permission from the KCDC is required for those of Grade 3 or 4. The classification is as follows:
• Grade 1: facilities that handle high-risk pathogens that are unlikely to cause diseases to healthy adults.
• Grade 2: facilities that handle high-risk pathogens that can cause human diseases unlikely to be a serious hazard and for which effective treatment and preventive measures are available.
• Grade 3: facilities that handle high-risk pathogens that usually cause serious human diseases and for which effective treatment and preventive measures are available.
• Grade 4: facilities that handle high-risk pathogens that usually cause serious human diseases and for which effective treatment and preventive measures are not usually available.
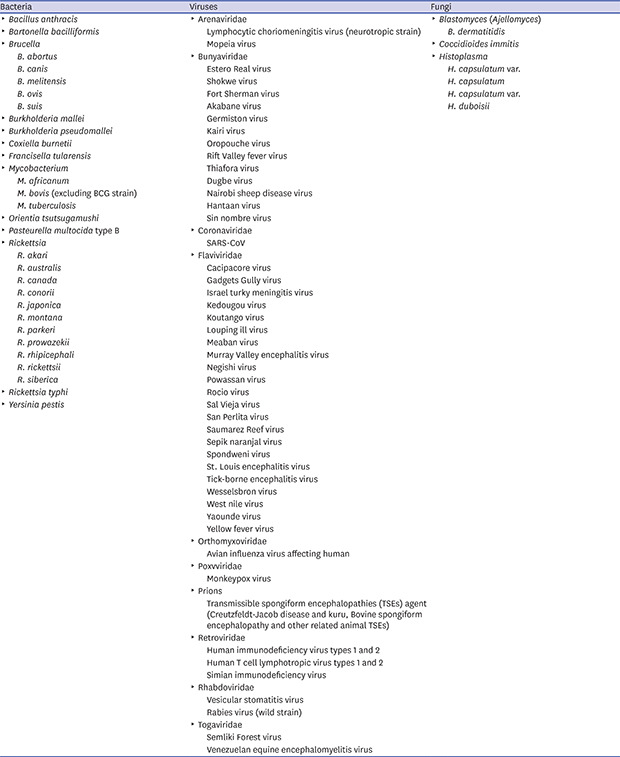
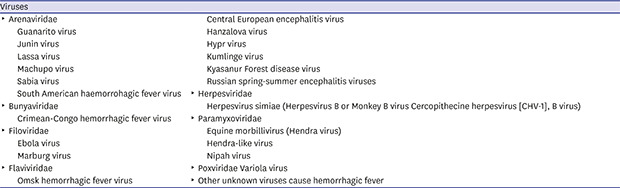
In addition, the same act designates some infectious agents as ‘high-risk pathogens’ that require special attention from the nation and society, because of the potential of serious risk to public health if used for biological terrorism, or spread to the outside by accident (Appendix 4). Some agents in Risk Group 2, 3, and 4 recommended by the WHO and some causative agents of a recent outbreak, such as SARS-CoV and MERS-CoV, are included in this list. It is anticipated SARS-CoV-2 will be added here in the near future by revision of the act.
2. The purpose of the autopsy for infectious diseases
1) Identification of the causal relationship between death and infectious diseases
Autopsy plays a critical role in 1) determining the situation and specific causes of death, 2) excluding other causes of death when a patient dies during treatment or isolation for a confirmed infection, and 3) evaluating the medical relationships between infection and death if the infection is not a direct cause of death.
2) Provide medical and epidemiological information through a final diagnosis based on pathology
Autopsy is able to provide crucial information for 1) the establishment of an appropriate treatment plan based on the pathological mechanisms by confirming the clinical course, symptoms, histology, and prognosis, and 2) scientific evidence to control and prevent the spread of pathogens within the community, by identifying the path of transmission, and the prevalence of the target population.
3) Provide grounds for judgment on potential legal disputes
Since immediately after a particular death, the possibility of legal disputes related to the death are often unclear, and the bereaved family are often confused, the conducting of an autopsy should be decided under careful consideration of the circumstances surrounding the death. Potential legal disputes may be related to the validity and relevance of medical treatment or administrative actions, compensation claims against industrial accident insurance or commercial medical insurance, or professional negligence of a business owner. Most of the situations are already covered by the criteria for the decision of unnatural deaths suggested by the KSLM (Appendix 5), or the instructions for handling unnatural deaths declared by the Korean National Police Agency (Appendix 6).
3. Current issues regarding the autopsy for infectious diseases in Korea
1) Lack of medical history of the deceased
Most of the medical history provided before the autopsy by the police is limited to the statements of bereaved families or acquaintances, or concise data from the National Health Insurance Corporation. Obtaining the medical records of the deceased needs an additional effort of the police or the bereaved families. However, the medical information is mandatory in identifying the health status of the deceased, and preparing against the potential risk of infection. The incidence of tuberculosis among autopsy workers is known to be 100–200 times that of the general population,11 while it has never been investigated in Korea. A small-group survey in Korea indicated that the prevalence of tuberculosis and hepatitis B among medical workers was suspected to be very high.12 Because hepatitis C and AIDS are difficult to cure and have a poor prognosis, serologic tests are performed on all surgical patients to protect medical personnel. But currently in Korea, no particular tests are required to be conducted in the routine for a dead body before the autopsy.
2) A criminal justice-oriented death investigation system
The purpose of the medico-legal autopsy may be divided into a judicial one, to confirm criminal relevance, and an administrative one, to manage public issues related to infectious diseases, accidents, or disasters, while that of the clinical autopsy is usually focused on medical evaluation. In Korea, the legal basis for all forms of autopsy is prepared. For example, in the cases of infectious diseases that are not expected to be related to crime, the autopsy may be conducted by the Minister of Health and Welfare, the mayor, the governor, the Director of the KCDC, or the head of the quarantine office. But in practice, the autopsy is always requested by the police, which inevitably limits its purpose.
3) Regional and institutional deviation of autopsy facilities and equipment
Although autopsy rooms are installed at the National Forensic Service (NFS) and its local branches, and some medical schools having forensic or pathology departments, their BSLs are in different situations. For example, the headquarters of the NFS has a special autopsy room of BSL3, while some medical schools have only BSL1 rooms. In principle, if the deceased is known to be a tuberculosis patient, the autopsy should be conducted in the BSL3 autopsy room, because Mycobacterium tuberculosis belongs to Risk Group 3 with SARS-CoV and HIV.10 But this principle is hard to follow, due to the high prevalence of tuberculosis in Korea, and a lack of medical history, as mentioned above. Each institution is in charge of the management of personal protective equipment (PPE) required for the autopsy, without sharing a standardized protocol.
4) Insufficient health support for autopsy personnel
To assess the risk of infection caused by autopsy, the medical conditions of autopsy personnel should be checked periodically, especially after the autopsy of a high-risk person.5 Throughout the branches of the NFS and the universities, there are no principles for the list of target pathogens, the method and frequency of surveillance test, and the criteria for subjects who need such monitoring.
5) Lack of safety considerations for other facilities and workers related to the autopsy
To conduct an autopsy, the sequence of procedures should be involved, of 1) transfer from the funeral home, 2) receive the body at the autopsy room, 3) check the identity of the body with the police or bereaved family, 4) perform the autopsy, 5) return the body to the funeral home, and 6) transfer the samples for postmortem test to other departments. The workers who will be involved before and after the autopsy should be guided and trained in the use of PPE and hygiene control, because during the wrapping and transporting processes, there is a possibility of contagion from the deceased. Laboratory personnel dealing with samples taken from the body during the autopsy should be aware of the potential risk of infection in all autopsy samples, and receive the same level of health support as the autopsy personnel. In particular, all laboratories dealing with the initial sample that has not been chemically treated or biologically inactivated, must have BSL2 or higher level of facilities and appropriate PPE.10 Throughout the autopsy-related facilities in Korea, there is only a low level of safety considerations for these types of personnel who are not directly involved in the autopsy, and the level is insufficient to deal with a body or samples infected by a high-risk pathogen.
Go to :
III. STANDARD AUTOPSY PROTOCOLS FOR INFECTIOUS DISEASES
1. Target subjects and principles
1) General principles
All bodies should be considered to be infected by unspecified microorganisms, until they are diagnosed as negative by a medically verified examination, using appropriate samples. The autopsy personnel have the right to be protected from infection by the body, for which the affiliated agencies should make appropriate efforts. Even if an infectious disease is newly diagnosed after the autopsy, the risk of infection to the autopsy personnel should be low level. A ‘standard autopsy’ for infectious diseases is defined as an autopsy conducted by an agreed procedure for this purpose, which should always be observed, regardless of the prevalence of the infectious disease. For confirmed cases, some conditions could be added for the optimal protection of the autopsy personnel. In contrast, if any of the facilities, personnel, equipment, or procedure did not meet the standard, an autopsy shall be considered as an ‘ordinary autopsy’.
2) Risk classification
The risk of transmission during an autopsy could be assessed according to the infection status of the body (Table 1). To conduct an autopsy for a confirmed case, the biosafety levels of the facilities for autopsy and laboratory tests should be equivalent to or higher than that of the pathogen. During the prevalence of a certain infectious disease, all the unknown cases should be regarded at least as suspected cases. However, considering the realistic restrictions, if there were reasonable compensations, such as preliminary tests before the autopsy, adequate ventilation and disinfection of the facilities, or additional use of PPEs, the autopsy could be conducted by substandard protocols. Even for the negative cases that are allowed for the ordinary autopsy, a higher level of protection is recommended, because there is always the possibility of a false-negative.

Table 1
Case classification and their definitions
![]()
2. Preparations before autopsy
1) Consideration of preliminary test
Considering the prevalence and biological risks, a list of infectious pathogens should be selected, and periodically evaluated for surveillance. Preliminary tests for these pathogens are recommended. During the prevalence of high-risk pathogens (Appendix 4) or their equivalents, preliminary tests are mandatory for clinically suspected cases to determine the conduct and the coverage of the autopsy.4 The autopsy can be postponed until the results of the preliminary tests are available. Even for the cases in which the preliminary test was negative, if suspicious findings were found during the autopsy, it is recommended to repeat the test with the autopsy samples. The possibility of false-negatives should always be considered, because the results could be affected by the infection period, sampling methods, status of the samples or bodies, or the characteristics of the test itself.
2) Storage and transfer of the body
Place the body in a leak-proof transparent plastic bag with a thickness of 150 μm, and seal it. Do not use pins or clips that can damage the sealing conditions.13 Put the plastic bag into another opaque body bag, and wipe its outer surface with sodium hypochlorite diluted 1:4 (e.g., 5% sodium hypochlorite 100 mL + water 400 mL mix), and dry. Attach an identification tag to both the body and its bag, respectively, and make sure that they are not lost. Refrigerate the body at 4°C. At the beginning of the autopsy, disinfect the outer and inner surface of the body bag and the skin of the body with 70% alcohol or sodium hypochlorite diluted 1:99 (e.g., 5% sodium hypochlorite 5 mL + water 495 mL mix).
2. Management of the facilities and working environment
1) Facility standards
The biosafety standard of the autopsy-related facilities may correspond to the BSL in general, although a little modification is required to reflect the procedure and equipment of the autopsy. The concept of BSL is also adopted in the ‘Standards for the installation and operation of facilities handling high-risk pathogens (Ministry of Health and Welfare Notice No. 2019-59)’ (Appendix 3), which the Korean institutes should follow for handling microorganisms with potential biologic risk.
A BSL2 autopsy room is required for the ordinary autopsy, while a BSL3 or higher level is required for the standard autopsy, according to the risk group of the confirmed or suspected pathogen.10 In an autopsy room that does not meet the above criteria, at least 1) the air inside the autopsy room should not escape to other spaces in the building, 2) the route of exhaust should avoid other intake vent or public spaces, and 3) additional devices or PPEs should be utilized to compensate insufficiently met requirements. Considering the environment of the autopsy room and the prevalence status of the time, the preliminary test of all the requested bodies should be considered for certain pathogens, and be referred to the decision of the conduct and coverage of the autopsy.
2) Waste disposal
Waste generated in all processes related to the body correspond to medical waste. They should be immediately disposed of in a dedicated envelope or containerboard box. In particular, sharp tools, such as injection needles, suture needles, or scalpels, should be discarded in a dedicated plastic container. Waste are sealed, disinfected, and then refrigerated in a dedicated warehouse. They should be transported to a medical waste incinerator within 7 days, and disposed of within 2 days.
3) Disinfection
If a surface is contaminated, wipe it with sodium hypochlorite diluted 1:49 (e.g., 5% sodium hypochlorite 10 mL + water 490 mL mix), and leave it for 15–30 minutes, before wiping it again with water. If a metal surface is to be disinfected, wipe it with 70% alcohol (e.g. 100% alcohol 70 mL + water 30 mL mix). If a surface is visibly contaminated by blood and body fluids, wipe it with sodium hypochlorite diluted 1:4 (e.g., 5% sodium hypochlorite 100 mL + water 400 mL mix), and leave it for 10 minutes, before wiping it again with water. The sodium hypochlorite solution should be newly mixed each time. After disinfection is finished, thorough ventilation is required.
4) Laundry
Reusable surgical garments (e.g., gown, mask) made of cotton could be included in the alternative list of PPEs. The cotton contaminated with blood or body fluids should be washed with hot water at 70°C or higher. If unavailable, soak them in sodium hypochlorite diluted 1:49 (e.g., 5% sodium hypochlorite 100 mL + water 4,900 mL mix), and leave them for 30 minutes before washing. Handle as gently as possible, to avoid aerosols.
3. PPEs
1) General principles
Aiming to protect the whole body of the autopsy personnel, including respiratory tract, eyes, and hands, from the infection, PPE should be selected in consideration of the nature and the infection route of the pathogen, and the expected situation of possible exposure. PPE should in principle be disposable or single-use, but some items (e.g., powered air-purifying respirators (PAPR), goggles, face shields, surgical garments made of cotton, and boots or shoes) may be designed for reuse, which should be disinfected or sterilized according to the manufacturer's instructions. Keep hair from flowing down, and remove personal accessories, like watches, in advance. To prevent unnecessary contamination, each manual of the PPEs, including dressing and undressing orders, should be understood in advance, and properly applied. Once the PPEs are used, they shall be discarded or disinfected, being regarded as contaminated. Hand hygiene shall be carried out before and after dressing or undressing. Damaged or contaminated PPEs should be discarded, without being reused or stored again. Cross-check between the autopsy personnel is recommended of whether the PPEs are worn properly, or not.
2) Selection of PPEs
Table 2 lists the recommended PPEs and their alternatives. The components of PPEs can be adjusted to the extent that their purpose and function are guaranteed to be maintained. According to the expected risk of exposure to the pathogen through working, some parts of PPEs could be applied selectively, as marked in the column ‘Transfer of bodies.’
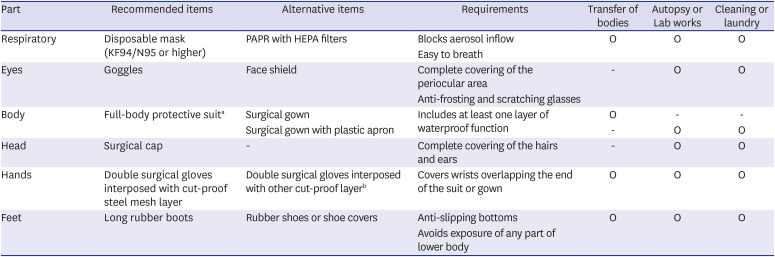
Table 2
Recommended components of PPEs, and their alternatives
PPE = personal protective equipment, PAPR = powered air-purifying respirators, HEPA = high-efficiency particulate air.
aIf a full-body suit is not available, surgical cap and long boots can be used to minimize exposed parts. Also, if the suit or gown is not made of waterproof material, the waterproof function of the PPEs can be supplemented with a plastic apron or arm covers; bAlthough they are not truly cut-proof, work gloves made of cotton may interrupt the movement of blades.
![]()
3) Dressing and undressing orders
The dressing order of PPE should be as follows:
Hand hygiene → Inner gloves → Lower part if full-body suit → Boots or shoes → Mask → Goggles or face shield → Upper part of the full-body suit or surgical gown and cap → Outer gloves
The undressing order of PPE should be as follows:
Outer gloves → Disinfection of inner gloves → Full-body suit or surgical gown and cap → Boots or shoes → Disinfection of inner gloves again → Goggles or face shield → Mask → Inner gloves → Hand hygiene
It is recommended to disinfect inner gloves at each step, as during the undressing they may become contaminated. If PPEs are found to be damaged, these cases should be considered as exposure to the pathogen, followed by proper management for the personnel.
4. Autopsy procedures
1) General principles
All the processes should be supervised by an experienced forensic pathologist. The number of people who participate in the autopsy should be minimized. However, it is recommended that at least two people be present in the autopsy room, in case of an emergency.8 To prevent cutting injuries, the dissection of each body part should be conducted by only one person at a time. A person who is not directly participating in the autopsy, such as the bereaved family member or police, is restricted from entering the autopsy room. During the prevalence of certain infectious diseases or the autopsy for confirmed cases, the access of trainees, such as medical students or residents, is also restricted. If necessary, observation through a window or a monitor is recommended, in a completely separate space from the autopsy room.
2) The main points of autopsy procedures
All the autopsy personnel should be cautious with sharp objects, such as scalpels, knives, needles, or bone sections, which can cause cutting injuries. Damaged or contaminated PPEs should be immediately discarded, and replaced with new ones. In the case of exposure to infection source, disinfect the exposed area immediately in a proper way; and if there is medical evidence, start prophylactic treatment.
If the body is suspected to have an airborne disease, the following should be operated with special caution, to prevent aerosols: 1) cutting bone with electronic saws, for which replacement by manual saws or additional use of vacuum inhalers is recommended, 2) opening the containers or centrifugation of samples, 3) body movement during transportation or postural adjustment during autopsy, which may cause spout of oral and nasal contents, 4) incision of the bronchus or lung parenchyma, which may expose the secretion inside, and 5) washing the body with a showerhead, which may spray its body fluids or adhesives together.
3) Test to confirm the infection
For the suspected cases or the unknown/negative cases with suspicious findings in the autopsy, a medically verified test at the time for each pathogen or disease should be requested, with appropriate samples. In these cases, the autopsy personnel and facilities should be managed as if they participated in the autopsy for confirmed cases, until the test result is assured to be negative.
4) Handling and transport of the autopsy-derived samples
The initial sample, which is not chemically treated nor biologically inactivated, should be handled within the biosafety cabinet installed in the BSL2 laboratory by experienced personnel wearing the PPEs equivalent to that used in the autopsy room. Meanwhile, after chemical treatment or biologic inactivation, the samples can be handled on an ordinary bench. Purified DNA or protein can be handled in the BSL1 laboratory, but the use of a biosafety cabinet or its equivalent is recommended.
To transport the autopsy samples, they should be prepared in the following order: 1) put the samples into the primary container, and seal it, 2) disinfect the outer surface of the primary container with 70% alcohol, and label it with an identification tag, 3) wrap the primary container with an absorbent (e.g., paper towel), 4) put the primary container into the secondary container, and seal it, 5) put the secondary container into the tertiary container and seal it, and then label it with a tag. The personnel who pack or open the containers should wear the PPEs equivalent to that used in the autopsy room or laboratory. Any work that requires contact with the containers, for example, simple transportation in sealed status, requires at least the wearing of gloves.
5. Human resource management
1) General principles
The affiliated agency should recognize the major infection history of all personnel who participate in autopsy or handle postmortem samples, and take necessary measures to prevent infections. If the standard autopsy was conducted without any damage of PPEs, the risk of infection is generally low. However, if the biologic nature of the pathogen or the epidemiology and pathophysiology of the disease are not fully identified, all the participants should be alert during the expected incubation period, even though they are not obviously exposed, with self-monitoring of the symptoms and the minimizing of face-to-face contacts. All the personnel who have accessed the autopsy room should be recorded: not only the direct participants in the autopsy, but also assistants for the maintenance of the facilities.
2) Preparations before autopsy
Considering the prevalence and biological risk, a list of infectious pathogens should be selected, and periodically evaluated for surveillance. If there is clinical evidence, prophylaxis, like vaccination, is recommended. In particular, each participant in the autopsy of confirmed cases should check whether he or she is already infected with the pathogen or not, so that if he or she is infected during the autopsy, the infection source could be traced.
3) Actions for the suspicious exposure
Fig. 1 summarizes the actions needed for the autopsy personnel and his or her affiliated agency after the autopsy, according to the infection status of the body, postmortem test for pathogens and its result, and the presence of suspicious situation for exposure.
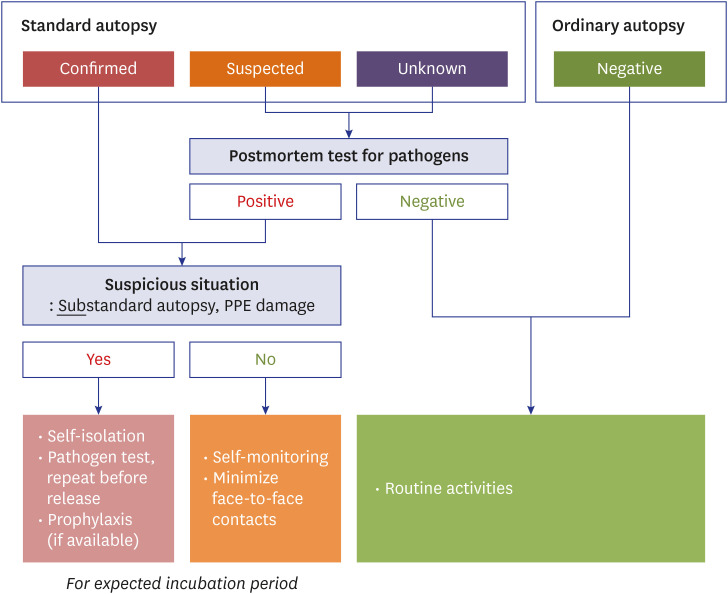
In the case of personnel who participated in the autopsy of a body confirmed to be infected but the standard protocol was followed, there is no possibility of exposure, so only self-monitoring of the symptoms and the minimizing of face-to-face contacts during the expected incubation period are required. However, if the autopsy procedures failed to meet the standard protocol, or the PPEs were damaged, infection should be suspected. In this case, self-isolation during the expected incubation period, and if available, prophylaxis, is required. The relevant personnel should be tested for the pathogen at the time point when related symptoms are shown, or the isolation period is nearly ended. If a test was requested after the autopsy, but the results are pending, the same actions are required in the interim.
If the autopsy procedures failed to meet the standard protocol, or the PPEs were damaged, the forensic pathologist in charge of the autopsy may consider adjusting the participant members, or discontinuing and delaying the autopsy schedule, to protect the autopsy personnel.
If a test for certain infection was requested after the autopsy, the process and the result should be shared with all the personnel who had, or would have, contact with the body, including the police, the bereaved family, the person who has discovered, reported, inspected, or transported the body, and the funeral staff. They are required to minimize face-to-face contacts, until the test result is confirmed.
6. Special considerations for COVID-19
1) Overview
COVID-19 is a respiratory syndrome caused by the infection of SARS-CoV-2, which belongs to the coronavirus family. Currently, in Korea, COVID-19 is regarded as an ‘emerging infectious disease syndrome,’ which is included in Class 1 legal infectious disease (Appendix 1), and SARS-CoV-2 is considered a high-risk pathogen, which needs ‘urgent management’ (Appendix 4). It is known to be transmitted through aerosols, droplets, or direct contact, while the viruses have also been found in tears and feces.1415 The incubation period is up to 14 days, and symptoms were expressed within 12.5 days after exposure in 95% of the infected. According to the studies published so far, the survival period of SARS-CoV-2 is 3 hours in aerosols, 4 hours on copper surfaces, 24 hours on cardboard surfaces, and 2–3 days on plastic or iron surfaces, which indicate that SARS-CoV-2 can survive for a considerable period outside of the host.16
2) Clinical and pathologic findings
SARS-CoV-2 patients show diverse symptoms, ranging from asymptomatic to severe respiratory failure. Major symptoms are fever, fatigue, dry cough, muscle ache, and shortness of breath; and a few cases included sputum, headache, hemoptysis, and diarrhea. Recently, the CDC of the United States and the KCDC added ageusia and anosmia as major symptoms of COVID-19.
The patients are frequently diagnosed with viral pneumonia, regardless of the actual severity of their symptoms. As of yet, there is no specific therapeutic agent or vaccine. Severe patients suffer from respiratory failure, septic shock, and multiple organ failure. The median time to respiratory failure was 8.0 days from symptom onset, while that to mechanical ventilation was 10.5 days.
3) Indication for the diagnostic tests
A diagnostic test for SARS-Cov-2 could be considered based on 1) medical history or symptoms, which are mainly fever or respiratory symptoms, and also include headache, abdominal pain, and fatigue, 2) epidemiologic connection, such as temporal, spatial, or geographical relationships with an epidemic region or confirmed patient, and 3) gross pathologic findings of the lungs, such as consolidation, thick exudates, excessive mucus, or other findings suggestive of acute or severe pneumonia, regardless of the clinical symptoms.
4) Facilities and procedures of the autopsy
The autopsy of confirmed and suspected cases should be conducted at BSL3 or equivalent facilities. For unknown cases, the autopsy could be conducted under BSL3 facilities, but there should be reasonable compensations, such as preliminary tests before the autopsy, adequate ventilation and disinfection of the facilities, or additional use of PPEs. The management of autopsy related facilities follows the standard autopsy protocol as mentioned above. Even though the generation of droplets or aerosols from bodies is unlikely, it is recommended to minimize direct contact with the bodies or postmortem samples, and prevent damage of PPEs.22
5) Sample handling
In the case of samples for virus test, attach the swabs for sample collection to the upper airway (pharynx, larynx) and the lower airway (lung) for a few seconds, so that the secretions or exudates could be absorbed sufficiently. Put the swabs into the transport medium immediately, and seal the caps. Other samples for postmortem tests should be regarded as ordinary cases only after they are confirmed to have an adequate level of biological risk, including the possibility of aerosol generation.23 Toxicology samples, such as blood and gastric contents, should be disinfected by mixture with 100% alcohol for 3 (sample):7 (alcohol) ratios, and left for more than an hour. This method can be applied to various postmortem samples, except for alcohol concentration test.24
For pathologic study, the respiratory system, including proximal and distal trachea, pulmonary hilum, main and segmental bronchi, pulmonary parenchyma, and other organs, such as the heart, the liver, kidney, spleen, and intestines, could be sampled, according to the purpose of the study. Fix them with 10% formalin for 2–3 days.25
6) Actions after the autopsy
(1) The autopsy for confirmed cases
The management of facilities, environment, and human resources follows the standard autopsy protocol suggested above. The initial samples should be sent to the BSL3 laboratory.
If there is a risk of infection due to damage of PPEs, skin exposure, aerosol-prone manipulation, or cutting injuries, the relevant autopsy personnel and his or her contacts should be provided with proper medical treatment, including disinfection and virus test. Also, for 2 weeks from the exposed time point, which is the expected incubation period of COVID-19, they should be isolated and excluded from the work, even though the initial test result is negative. The affiliated agency should monitor his or her symptoms.
(2) The autopsy for suspected or unknown cases
If a virus test for the body is carried out during the autopsy, the participated autopsy personnel should minimize face-to-face contact, until the results are notified.
If the result of the virus test is positive, a postmortem test, such as toxicology (except for alcohol), biochemical, or genetic test should be requested, after the disinfection of the samples by mixing with 100% alcohol for 3 (sample):7 (alcohol) ratios.24 Then the samples should be transported according to the standard protocol above. The management of the facilities, environments, and human resources generally follows the standard protocol above, while the disinfection process of the autopsy room and related facilities should refer to the KCDC guideline. If an infection is suspected, for example, due to a substandard autopsy procedure or damaged PPEs, the autopsy personnel and their contacts should be provided with proper medical treatment, including disinfection and virus test, with isolation and monitoring for 2 weeks, as mentioned above in section 6)-(1). When the body is confirmed to be negative for the virus test, the isolation and monitoring could be discontinued.
Go to :
IV. SUGGESTION FOR THE DEATH INVESTIGATION SYSTEM IN KOREA
Since the autopsy personnel are under constant risk of infection, there should be consistent effort for the implementation of the standard autopsy guidelines. First of all, expecting the periodic spread of infectious diseases in the future, the preparation of adequate level of PPEs and BSL of the autopsy related facilities, and the establishment of a health monitoring and surveillance system are required.
To compensate for the problems of the current death investigation system, which is focused on the judicial purpose, in the short term, the range of unnatural death considered as the subject of judicial autopsy should be expanded as wide as possible, in consultation with the police and the prosecution. In the long term, the autopsy request ordered by the directors of the Ministry of Health and Welfare or the KCDC should be encouraged with systemic supports. Also, the Ministry of Health and Welfare or the KCDC should be in charge of the management of biosafety requirements in the autopsy facilities and the arrangement of the qualified human resources and financial support, so that this guideline could be satisfactorily implemented.
Forensic medicine has developed and gradually improved over a long period, despite all the difficulties such as unfavorable environment and systemic constraints. However, in the upcoming post-COVID-19 era, there should be more integrated and organized provision, especially against the risk of infectious diseases. Health authorities and forensic pathologists should work together to improve the autopsy environment and the death investigation system, so that a better national health system can be established in the near future.
Go to :
 XML Download
XML Download