

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Split liver transplantation (SLT) was developed in the late 1980s to increase the number of donor livers available for transplantation.1 However, early results in patients undergoing SLT were not favorable.2 The European Liver Transplant Registry reported that 3.7% of deceased donor liver transplantation (DDLT) operations between 1968 and 2000 were SLT, and the percentage increased to 6% during the 2000s.34 In the United States, however, fewer than 1% of all liver transplantation (LT) cases performed between 2002 and 2009 were SLT.5 Of the 2,462 patients in Korea who underwent DDLT from 2005 to 2014, 86 (3.5%) adult patients received split extended right liver (ERL) grafts.6 Considering that a small number of donor liver splitting were performed for two adults,7 the proportion of adult recipients undergoing SLT in Korea was estimated to be approximately 4%.
In conventional SLT, the deceased donor liver is divided into two parts, a left lateral section for a pediatric recipient and an ERL graft for an adult recipient. Most SLTs are of the conventional type, which has been shown to shorten the waiting list for pediatric LT candidates.891011 In Korea, a new liver allocation system based on model for end-stage liver disease (MELD) score was introduced in June 2016 to optimize the use of deceased donor livers.12 Introduction of this liver allocation system increased the daily cutoff point of MELD score for adult DDLT, primarily due to profound organ shortage.1314
Because adult DDLT candidates in poor pretransplant conditions frequently experience poor posttransplant outcomes,15 transplant surgeons have been reluctant to perform SLT, as they were concerned that split liver grafts would have poorer function than whole liver grafts. A study using the Korean Network for Organ Sharing (KONOS) database found that MELD score > 30 and graft-recipient weight ratio (GRWR) ≤ 1.0% were risk factors for survival in adult SLT recipients.6 Because that study was a collective review of patients who underwent SLT over 9 years, the study results may not objectively reflect the current reality of SLT in Korea. The present study therefore compared the incidence and prognosis of SLT with those of whole liver transplantation (WLT) by analyzing adult patients who recently underwent DDLT at a high-volume LT center.
Go to : 
METHODS
Study design
This study was a retrospective case-controlled observational analysis evaluating patients who underwent DDLT at the Asan Medical Center. To assess the prognosis of SLT, patients who underwent SLT were regarded as the study group and those who underwent WLT as the control group. In addition, the two groups were subjected to 1:5 propensity score matching (PSM). The SLT group included adult recipients of split ERL grafts, but did not include pediatric recipients of split left lateral section grafts.
To better reflect real-world performance of SLT, the study period was defined as the 42 months between June 2016 and November 2019. To avoid unnecessary bias from patient selection, retransplantation patients who had undergone living donor liver transplantation (LDLT) or DDLT before the study period or LDLT during the study period and then required retransplantation were excluded.
Donor selection
Deceased donors can be selected for SLT if they had stable hemodynamics, are aged ≤ 40 years, have a body weight ≥ 50 kg, and are being treated with low-dose inotropics.6 The KONOS policy requires donor organ splitting as mandatory only for a combination of adult and child recipients. That is, if a candidate deceased donor fulfills the criteria for SLT, the KONOS selects appropriate adult and child recipients on the waiting list. If no proper candidates are available, then the whole liver graft is assigned to an adult recipient candidate. If this whole liver graft appears too large for a single selected adult recipient, it may be utilized for two-adult SLT, both to match the graft size and to expand the donor graft pool.7
Korean MELD score-based allocation system
The Korean MELD score-based liver allocation system is based on the following original calculation: (9.57 × loge [creatinine, mg/dL] + 3.78 × loge [total bilirubin, mg/dL] + 11.2 × loge [international normalized ratio] + 6.43). MELD score status is divided into five categories, with status 1 indicating acute liver failure and early graft failure, status 2 defined as a MELD score of 38–40, status 3 as a MELD score of 31–37, status 4 as a MELD score of 21–30, and status 5 as a MELD score of ≤ 20. Patients with hepatocellular carcinoma within the Milan criteria receive an additional 4–5 points if their MELD score is ≤ 20. In addition to MELD score, recipients having identical blood groups and from the same region of the country as the donors were considered a priority.1314
Surgical techniques
The surgical techniques for adult-child and two-adult SLTs have been described previously in detail.71617 The usual left lateral section graft is actually an extended left lateral section graft, thus the left medial section parenchyma that is attached to the right liver does not function because all inflow vessels and bile duct are totally transected. Right trisection grafts have therefore been replaced by ERL grafts.1819 The left lateral section graft after in situ splitting was often procured in advance, similar to the protocol for pediatric LDLT. Thereafter, the remnant right liver graft was harvested as the same time as other abdominal organs.
SLT-specific complications
The split ERL grafts have the residual portion of the left medial section (segment IV [S4]), which does not function because the inflow vessels and bile duct are transected. The retained S4 parenchyma often undergoes silent atrophy, but retained S4-associated complications such as ischemic parenchymal necrosis and biliary leak can develop. These complications increase morbidity and can sometimes lead to graft loss.202122 These retained S4-related complications were classified as ischemic parenchymal necrosis and biliary leak. These were evaluated with serial posttransplant liver dynamic computed tomography (CT) scans. In accordance with our institutional LT management protocols, posttransplant dynamic CT scans were taken weekly when the patients were in the hospital, and then at 1, 3, 6, and 12 months after the LT operation. The amount of ischemic infarct of the S4 parenchyma was estimated using 1-week CT volumetry and then classified as either large (> 10% of the split ERL graft volume) or small (≤ 10% of the split ERL volume). Biliary leak was defined as the presence of overt bile drainage through the abdominal drain.
Statistical analysis
The 1:5 PSM was performed using a nearest-neighbor matching method.23 The matched parameters in the order of significance were MELD score and KONOS status, primary liver disease, GRWR, pretransplant ventilator and renal support, sex and recipient age. Numerical data are presented as mean ± standard deviation. Continuous variables were compared using Student's t-test or the Mann-Whitney U test. Categorical variables were compared using the χ2 test or Fisher's exact test. Survival rates were estimated using the Kaplan-Meier method and compared with the log-rank test. Cox proportional hazard regression was used for multivariate analysis. A P value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 22 (IBM, New York, NY, USA).
Ethics statement
The study protocol was approved by the Institutional Review Board (IRB) of the Asan Medical Center, which waived the requirement for informed consent due to the retrospective nature of this study (IRB No. 2019-1347).
Go to :
RESULTS
Patient grouping and profiles
During the study period of 42 months, 242 adult patients aged ≥ 18 years underwent a total of 256 DDLT operations, including 14 patients (5.8%) who underwent retransplantation after primary DDLT. Of the 242 cases who underwent primary DDLT, seven patients (2.9%) underwent SLT and 235 (97.1%) underwent WLT. All SLTs involved adult-pediatric recipient matching, with none being two-adult SLT.
Pretransplant total bilirubin concentration, donor age and graft weight differed significantly in the SLT and WLT groups. Following 1:5 PSM, 35 patients who underwent WLT were matched to the seven patients who underwent SLT. Except for donor age, there were no significant differences between the two groups. Detailed profiles of the SLT, WLT and PSM-WLT groups are summarized in Table 1.
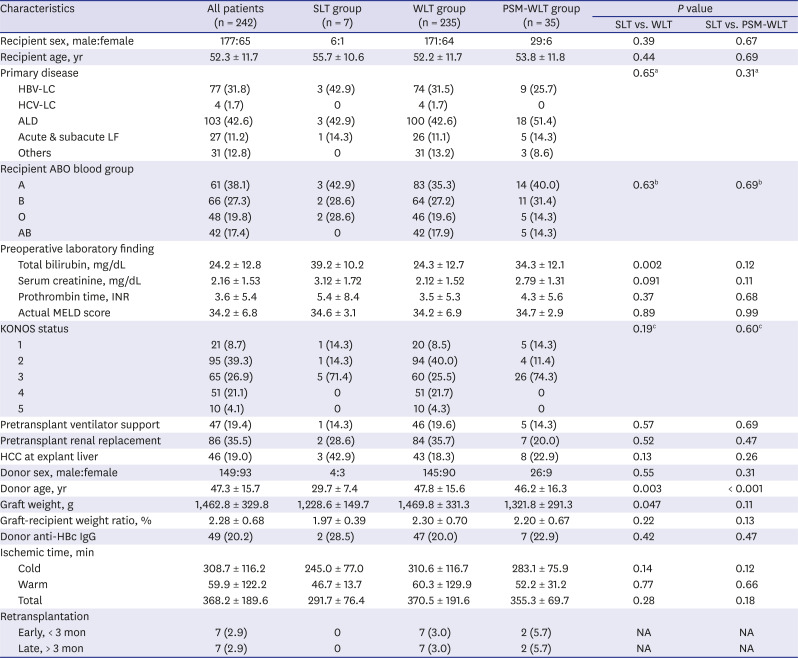
Table 1
Demographics and clinical characteristics of patient groups
Values are expressed as number (%) patients or mean ± standard deviation.
SLT = split liver transplantation, WLT = whole liver transplantation, PSM = propensity score matching, MELD = model for end-stage liver disease, KONOS = Korean Network for Organ Sharing, HBV-LC = hepatitis B virus-associated liver cirrhosis, HCV-LC = hepatitis C virus-associated liver cirrhosis, ALD = alcoholic liver disease, LF = liver failure, INR = international normalized ratio, HCC = hepatocellular carcinoma, anti-HBc IgG = hepatitis B virus core antibody immunoglobulin G, NA = not available.
aComparison between HBV-LC and other groups; bComparison between blood group A and B vs. O and AB; cComparison between status 1 and 2 vs. 3 to 5.
![]()
Comparing with SLT and WLT groups, the mean MELD scores were 34.6 ± 3.1 and 34.2 ± 6.9, respectively (P = 0.89); and GRWR was 1.97% ± 0.39% and 2.30% ± 0.70%, respectively (P = 0.22). Comparing with SLT and PSM-WLT groups, the mean MELD scores were 34.6 ± 3.1 and 34.7 ± 2.9, respectively (P = 0.99); and GRWR was 1.97% ± 0.39% and 2.20% ± 0.67%, respectively (P = 0.13). Requirement for ventilator support and renal replacement therapy before transplantation was 1 patient (14.3%) and 2 patients (28.6%) respectively in the SLT group; 46 patients (19.6%) and 84 patients (35.7%) respectively in the WLT group; and 5 patients (14.3%) and 7 patients (20%) respectively in the PSM-WLT group (all P > 0.47). The posttransplant hospital stay was 43.5 ± 34.6 days in the SLT group, 44.4 ± 47.2 days in the WLT group, and 44.1 ± 42.1 days in the PSM-WLT group (all P > 0.94).
Detailed profiles of SLT donors (Table 2) and recipients (Table 3) are presented separately. Donor age in the SLT group was 29.7 ± 7.4 years, which was significantly younger than that in the WLT (47.8 ± 15.6 years, P = 0.003) and PSM-WLT group (46.2 ± 16.3 years, P < 0.001).
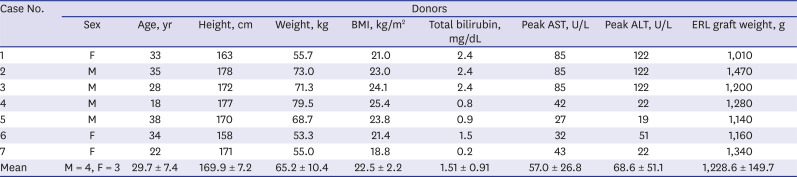
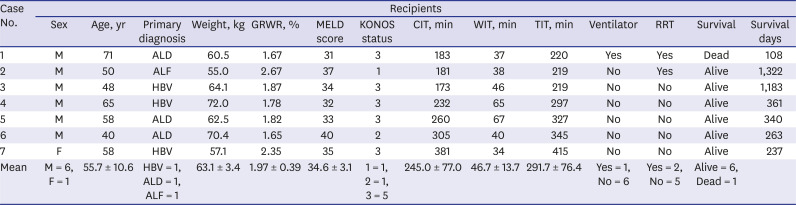
Table 2
Detailed profiles of the deceased donors of the split liver transplantation
BMI = body mass index, AST = aspartate transaminase, ALT = alanine transaminase, M = male; F = female, ERL = extended right liver.
![]()
Table 3
Detailed profiles of the adult recipients of split liver transplantation
GRWR = graft-recipient weight ratio, MELD = model for end-stage liver disease, KONOS = Korean Network for Organ Sharing, CIT = cold ischemic time, WIT = warm ischemic time, TIT = total ischemic time, RRT = renal replacement therapy, M = male, F = female, ALD = alcoholic liver disease, ALF = acute liver failure, HBV = hepatitis B virus-associated liver cirrhosis.
![]()
Fates of the retained S4 parenchyma
On the liver CT scans taken within 1 week after SLT, the retained S4 parenchyma showed a small or scant amount of ischemic necrosis in 5 patients (71.4%) in the SLT group, whereas the remaining 2 patients (28.6%) showed a relatively large amount of S4 ischemic necrosis. Follow-up CT scans taken 3-6 months after SLT showed that the retained S4 parenchyma was markedly atrophied, making typical ERL grafts (Fig. 1). The posttransplant peak levels of serum liver enzymes within the first week in the patients with large and small ischemic necrosis were aspartate transaminase 2,468.2 ± 1,101.7 U/L and 930.4 ± 492.8 U/L respectively (P = 0.039) and alanine transaminase 2,037.3 ± 1,001.3 U/L and 578.2 ± 318.8 U/L respectively (P = 0.023). The 6-month to 1-year follow-up abdomen CT scans showed complete disappearance of the S4 parenchyma in all survived patients.
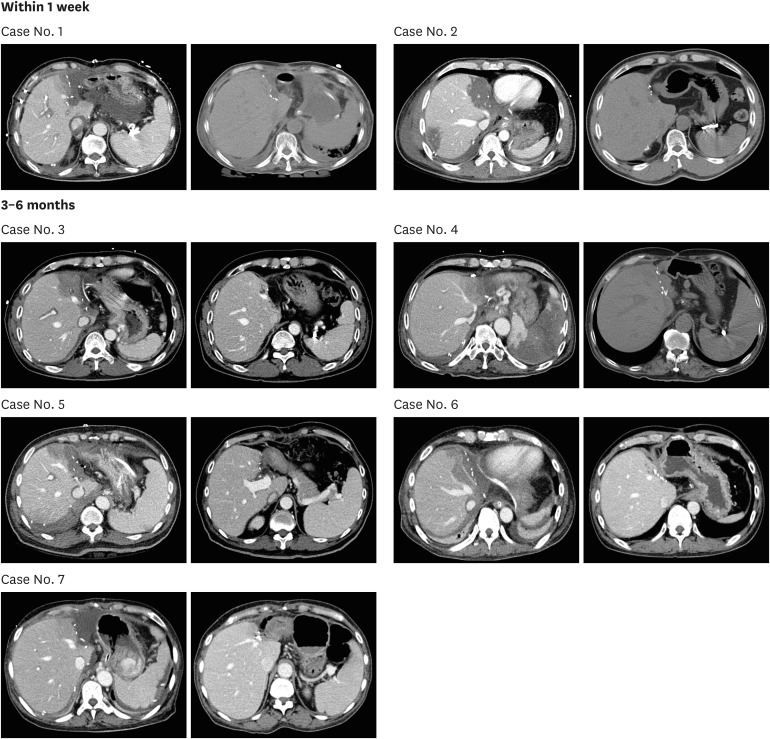 | Fig. 1Comparison of the posttransplant liver CT images taken within 1 week and 3–6 months after split liver transplantation. Case No. 2 and 3 were classified as having a large ischemic area at the retained segment IV portion and other 5 cases were regarded as having a small ischemic area. Contrast-non-enhanced CT scans were taken in 3 cases because of renal dysfunction.CT = computed tomography.
|
Comparison of posttransplant survival
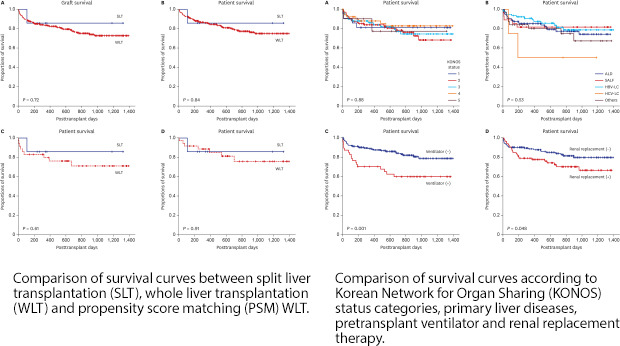
The graft survival rates in the SLT and WLT groups were 85.7% and 83.5% at 1 year, 85.7% and 76.6% at 2 years, and 85.7% and 72.6% at 3 years, respectively (P = 0.72) (Fig. 2A). In the SLT group, early graft dysfunction occurred in one patient (14.3%) in the SLT group, but no patient required retransplantation. In contrast, in the WLT group, early graft dysfunction and primary non-function developed in 27 patients (11.5%) and 4 patients (1.7%) respectively. Seven of them underwent retransplantation within 2 months after transplantation and another 7 patients underwent late retransplantation during 4 months and 4 years after transplantation.
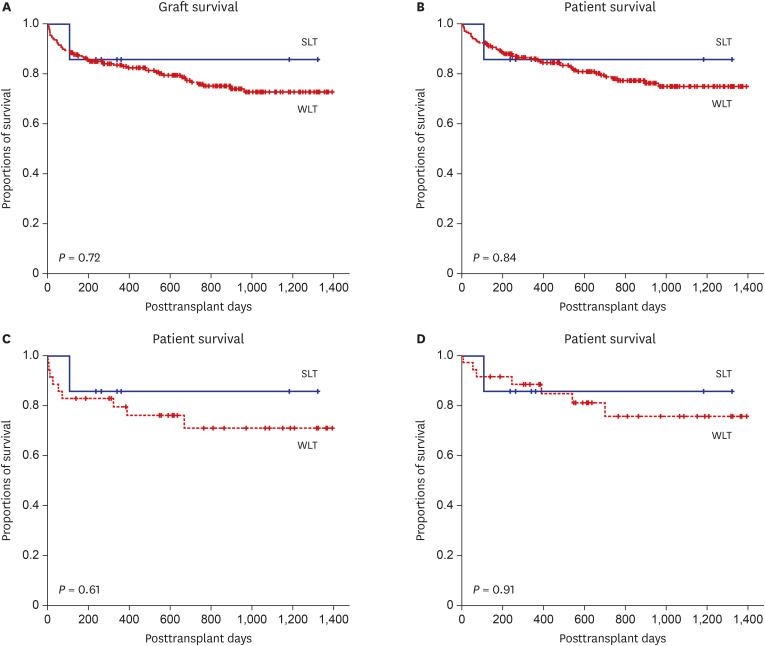 | Fig. 2Comparison of the survival curves. Comparison of the (A) graft and (B) patient survival curves between the SLT group and WLT control group. Comparison of the (C) graft and (D) patient survival curves between the SLT group and PSM-WLT control group.SLT = split liver transplantation, WLT = whole liver transplantation, PSM = propensity score matching.
|
The overall patient survival rates in the SLT group and WLT control group were 85.7% and 86.0% at 1 year, 85.7% and 78.7% at 2 years, and 85.7% and 74.9% at 3 years, respectively (P = 0.84) (Fig. 2B). One patient in the SLT group died of sepsis at 108 days after transplantation. One patient in the SLT group experienced bone metastasis, thus receiving radiotherapy currently. In the WLT group, in-hospital mortality within 3 months and 6-month all-cause death were 23 patients (9.8%) and 30 patients (12.8%), respectively. The causes of patient death in the WLT group included sepsis in 25 (10.6%), hepatocellular carcinoma recurrence in 5 (2.1%), various brain diseases including brain death in 7 (3.0%), chronic graft failure in 3 (1.3%), bowel infarct in 2 (0.9%), each one case (0.4%) of hepatic artery occlusion, intractable bleeding and sudden cardiac arrest, and unknown causes in 3 (1.3%).
Graft and overall patient survival rates in the PSM-WLT group were 79.5% and 88.4% at 1 year, 71.0% and 75.6% at 2 years, and 71.0% and 75.6% at 3 years, respectively. In the PSM-WLT group, in-hospital mortality within 3 months was 3 patients (9.8%) due to early graft dysfunction (n = 1) and sepsis (n = 2). Rates of both graft survival (P = 0.61) (Fig. 2C) and patient survival (P = 0.91) (Fig. 2D) were similar between the PSM-WLT and SLT groups.
Risk factor analysis for patient survival
The overall patient survival of all 242 patients according to the 5 categories of KONOS status showed similar survival outcomes (P = 0.88) (Fig. 3A). Survival analysis according to the primary liver diseases for DDLT showed similar overall patient survival rates (P = 0.53) (Fig. 3B), although patients with hepatitis C virus-associated liver disease had noticeably poorer outcomes. Donor age at a cutoff of 40 years did not affect patient survival (P = 0.31). Requirement for pretransplant ventilator support was significantly associated with inferior patient survival outcomes (P = 0.001) (Fig. 3C), and pretransplant renal replacement therapy also showed marginally inferior survival outcomes (P = 0.048) (Fig. 3D).
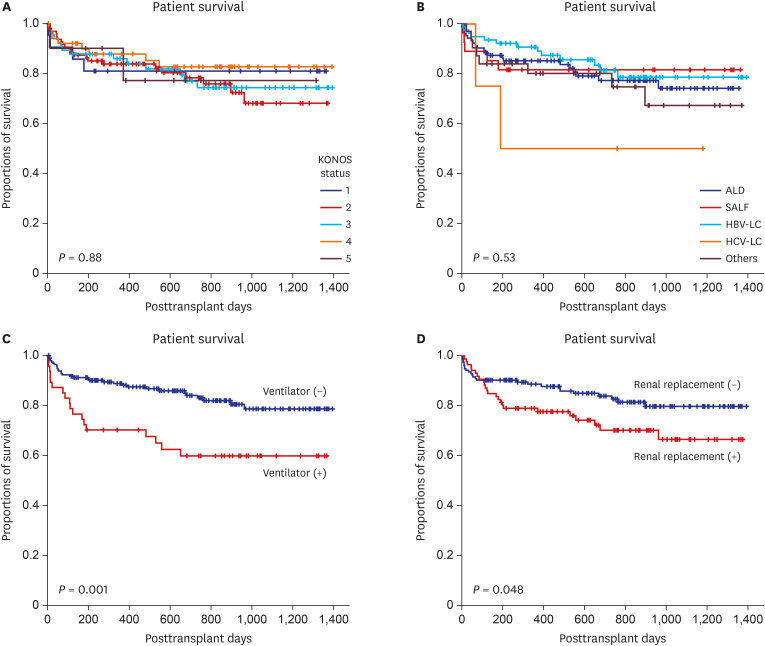 | Fig. 3Comparison of the survival curves. (A) Comparison of the patient survival curves according to the KONOS status categories, (B) the primary liver diseases for transplantation, (C) pretransplant ventilator support, and (D) pretransplant renal replacement therapy.KONOS = Korean Network for Organ Sharing, ALD = alcoholic liver disease, SALF = subacute liver failure, HBV-LC = hepatitis B virus-associated liver cirrhosis, HCV-LC = hepatitis C virus-associated liver disease.
|
Multivariate analysis showed that pretransplant ventilator support was significantly prognostic for overall patient survival (hazard ratio [HR], 2.26; 95% confidence interval [CI], 1.22–4.18; P = 0.009), whereas pretransplant renal replacement therapy was not statistically significant (HR, 1.39; 95% CI, 0.77–2.53; P = 0.27) (Table 4).
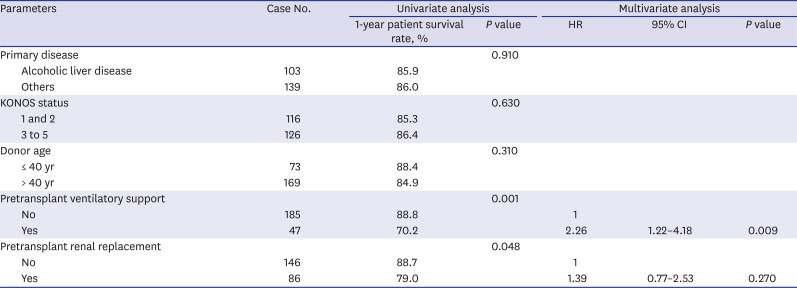
Table 4
Univariate and multivariate analyses of factors associated with patient survival
![]()
Go to :
DISCUSSION
The first child-adult SLT in Korea was performed in 1998 and the first two-adult SLT in 2003.1724 Since then, the number and proportion of SLTs have increased, although both remain small to date. There are two major reasons for the increase of SLT in Korea. The first is the increase in the number of deceased donors, thereby increasing the number of donor candidates for SLT.12 However, this increase has not been maintained in recent years, with the number decreasing due to various medico-social issues.1425 The second reason was the changes in KONOS SLT policy. Until 2012, a child recipient candidate for SLT could be listed as a candidate for SLT only when the parents were unsuitable liver donors.26 Since 2013, all pediatric candidates for DDLT are considered eligible for SLT.6
The major concern of transplant surgeons regarding adult SLT recipients is that the outcomes of ERL-SLT would be similar to those of WLT. The graft liver remaining after removal of the left lateral section is functionally comparable to an ERL graft.1827 Thus, the reserved graft function would be reduced according to the remained size of the right liver mass. Implantation of such a reduced liver graft to a high-risk patient may worsen posttransplant outcomes. A Korean multicenter study found that the risk factors for patient survival of SLT recipients were GRWR ≤ 1.0% and MELD score > 30.6 Because deceased donor grafts are subject to preservation and reperfusion injuries, a GRWR ≥ 1% is highly recommend for adult SLT recipients.728 The mean GRWR of the SLT group in this study was 1.97% ± 0.39% with a range of 1.67%–2.67%. By contrast, the majority of patients undergoing DDLT in Korea have MELD scores > 30, thus such as cutoff in MELD scores is not a critical parameter for deciding SLT. The mean MELD score of the SLT group in this study was 34.6 ± 3.1 with a range of 31–40.
We previously reported that there were no significant changes in the short-term outcomes of DDLT before and after introduction of the MELD score-based allocation system.13 The overall outcomes of adult DDLT in this study were comparable to those before adoption of the MELD score-based allocation system, but the survival outcomes of adults undergoing SLT in this study were better than those reported in the KONOS database analysis.6 Even after PSM, the outcomes of SLT in this study were comparable to those of WLT, suggesting selection bias in choosing patients to undergo SLT. Because many adult DDLT candidates were in very poor condition with very high MELD scores, and because the number of deceased donor livers had not increased, many critically ill patients had to receive marginal liver grafts. By contrast, the deceased donor livers selected for SLT were of high quality, resulting in a low risk of severe early graft dysfunction or primary non-function. Although the graft liver mass was reduced through splitting, the GRWR for adult recipients definitely exceeded 1.0%. In addition, the candidates for adult SLT were prudently selected after consideration of MELD score, application of renal replacement therapy and ventilator care. Thus, adult SLT candidates were in generally better condition and received higher-quality liver grafts of reduced size than in patients in the WLT group. These findings suggest that the outcomes of adult SLT would be comparable to those of LDLT using ERL grafts.
With regard to the GRWR in cases of ERL-SLT, the amount of S4 ischemia is known to be an important factor for determining actual GRWR. Since nearly all of the retained S4 parenchyma will undergo ischemic necrosis, it is reasonable to extract the volume of the S4 parenchyma from the ERL graft volume to estimate the actual GRWR. In addition, ischemic necrosis of the S4 parenchyma generates an additional metabolic burden on graft liver function, and a larger retained S4 parenchyma can therefore increase the risk of patient morbidity. Consequently, some authors have proposed the preemptive removal of the S4 parenchyma during SLT operation.2930 It is reported that ERL grafts with a larger retained S4 showed a greater elevation of their liver enzyme levels.27 Biliary leak from the graft liver cut surface has also been reported to be one of the retained S4-associated major complications.212227 We did not experience such S4-associated biliary leak among our present study series, probably due to ligation of the middle hepatic artery to the retained S4 and secure ligation of the S4 glissonian branches. If a patient survives after SLT operation, the retained S4 parenchyma will undergo progressive ischemia-inducing parenchymal atrophy during the first few months after SLT. However, the potential negative prognostic impact of large S4 ischemia cannot be ignored, especially during the early posttransplant period.27
Appropriate recipient selection is essential to optimize the outcomes of SLT in adult patients as higher recipient medical risk can increase the split-graft failure rate. A survey in the United States found that urgent LT was associated with high mortality rate in the right-liver graft recipients.31 Under the “sickest first” MELD-based allocation system, splitting a liver graft that can be allocated as a whole liver graft to urgent recipients with high MELD scores raises ethical questions.5
This study has several limitations. This is a retrospective, single-center study with a relatively small number of patients. Choice to perform SLT was decided on case-by-case basis, as there are no established guidelines for SLT. Further high-volume multicenter studies are necessary to validate the results of this study.
In conclusion, this study showed that survival outcomes were comparable in adult SLT and WLT recipients, probably due to the selection of high-quality liver grafts and low-risk recipients for SLT. Prudent selection of donors and adult recipients for SLT may expand the liver graft pool for pediatric patients without affecting the outcomes of adult recipients undergoing SLT.
Go to :
 XML Download
XML Download