

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Carbapenem-resistant Enterobacteriaceae (CRE), especially carbapenemase-producing Enterobacteriaceae (CPE), are emerging as a major threat due to limited treatment options and rapid spread.123 Since 2001, when the first CRE was detected, CRE have spread worldwide leading to 13,100 cases in the United States in 2017 and causing 68,000 serious infections in Europe.45 Increase in CRE is a global trend affecting many countries including Korea.6789 In addition to CRE outbreaks reported in several hospitals, reported CRE cases have increased from 5,717 in 2017 to 15,364 in 2019, and the proportion and number of CPE cases has also increased accounting for 68.8% of the CRE cases in 2018 in Korea.101112
CPE is especially a problem in long-term care facilities (LTCFs). History of admission, previous antibiotic exposure, and high Charlson comorbidity index scores are thought to be risk factors for CPE colonization.131415 Because patients in LTCFs generally have these risk factors, they are more vulnerable to CPE colonization.131516 This population has high risk of colonization as well as true infection leading to higher mortality. Furthermore, LTCFs play a central role in transmission to and from acute care hospitals.17 For this reason, infection control for CPE in LTCFs is emphasized and several countries have nationwide interventions including active surveillance in LTCFs.1819 Despite the importance of active surveillance, it is not mandatory to surveil patients admitted to LTCFs for CPE in Korea. The lack of insurance coverage makes CPE surveillance difficult in LTCFs even in patients exposed to CPE.
Previous studies investigating CRE including CPE prevalence and acquisition in Korea targeted acute care hospitals, especially intensive care units (ICUs).14202122 There is no data on CPE in LTCFs in Korea. In this study, we investigated the positivity of CPE in patients who were exposed to CPE positive patients in LTCFs. Environment has a crucial role in CPE transmission, and consequently we also investigated the environment around CPE positive patients.
Go to : 
METHODS
Setting and patient selection
This retrospective study was conducted as a part of the project of Seoul Metropolitan Government to evaluate CPE status. This study was performed in patients exposed to CPE in LTCFs in Seoul from December 2018 to April 2019. Patients were enrolled when they were admitted and placed in a room with a CPE positive patient or newly admitted to a room where a CPE positive patient stayed in a LTCF where CPE was detected in clinical samples and more than two cases of CPE were detected. The status of CPE colonization was investigated in patients along with the environment in which the CPE occurred.
Data collection
We collected rectal swabs from patients who had been admitted in the same patient room as the patients who were positive for CPE. Index cases were defined as those in the LTCFs with positive tests for CPE in the clinical samples. The specimens were examined for CPE along with genotyping. If the results of all the collected specimens in one LTCF were negative, further examination in that LTCF was stopped. If the results were positive, further rectal swabs were required from patients who were in the same room as the CPE positive patient as well as newly admitted patients in that room. Further surveillance was performed only at a weekly interval in this study, we did not perform repeated tests within the week for detecting false negatives. Further sampling was performed until no newly positive patient was detected for three weeks or all patients were transferred to isolation rooms. The infection control practitioners visited each LTCF. They provided swabbing materials and educated the nurses about the standardized method of rectal swabbing in each LTCF.23
Environmental sampling was coordinated and performed by infection control practitioners and epidemiologists at first visit. Environmental specimens were obtained by swabbing surfaces with 3M™ Pipette Swab Plus (3M, Saint Paul, MN, USA). Environmental samples were taken from different sites according to the ward structure in each hospital. Sites were classified as private patient space (side rails, side tables, buttons on monitor, urine bag, O2 circuit, hemodialysis machine, personal cabinet, and ventilator), common space in the patient room (rest room, washstand, refrigerator, blood pressure cuff, common chair, cart, air conditioner, radiator, window, remote control, medical waste container, entrance door, hand sanitizer in entrance), common space other than the patient room (rail bar in the hallway, medical waste container, refrigerator, dressing cart, water purifier, rest room, shower room, physical therapy room, treatment room, pantry), and nursing station (sink, prescription counter, telephone, mouse, keyboard, refrigerator, medicine cabinet).
Microbiological methods
Rectal swab specimens were obtained by inserting a Copan swab (Transystem™, COPAN, Brescia, Italy) and transferred in an icebox to the laboratory at Kangnam Sacred Heart Hospital for culturing. Each sample was inoculated onto Chrom Klebsiella pneumoniae carbapenemase (KPC) agar for screening CRE followed by matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) mass spectrometry (Bruker, Billerica, MA, USA) for identification. Polymerase chain reaction assays by SimpliAmp™ Thermal Cycler (ThermoFisher Scientific, Waltham, MA, USA) were used to identify the presence of blaKPC, blaVIM, blaIMP, blaOXA-48, and blaNDM and determine CPE genotypes. The Thermal Cycler method consists of the following steps: initial denaturation at 95°C for 2 minutes, 35 thermal cycles of denaturation at 95°C for 30 seconds, annealing at 55°C for 30 seconds and extension at 72°C for 90 seconds. The final extension was performed at 72°C for 7.5 minutes. Environmental specimens obtained by infection control practitioners and epidemiologists were transferred to the Seoul Institute of Health and Environment for detection of CPE.
Ethics statement
The study was approved by the Institutional Review Board (IRB) of Hallym University Kangnam Sacred Heart Hospital in Korea and informed consent was waived for the research conducted as a part of the project of Seoul Metropolitan Government (IRB No. 2020-02-119-002).
Go to :
RESULTS
From the 65 index cases, a total of 24 hospitals and 481 patients were enrolled. The 24 participating hospitals accounted for 19.0% (24/126) of all LTCFs in Seoul. Characteristics of enrolled hospitals are shown in Table 1. Median bed size was 194.5 beds (range, 131–404) and the median number of healthcare workers was 46 (range, 12–127). Nineteen hospitals (79.2%) had infection control committees and 13 hospitals (54.2%) had infection control physicians. Infection control nurses existed in 19 hospitals (79.2%) and 21.1% of them were nurse practitioners. One hospital refused to collect specimens from patients and only agreed to collect specimens from the environment.
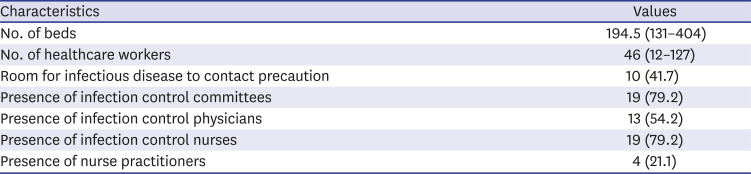
Table 1
Characteristics of the enrolled hospitals (n = 24)
![]()
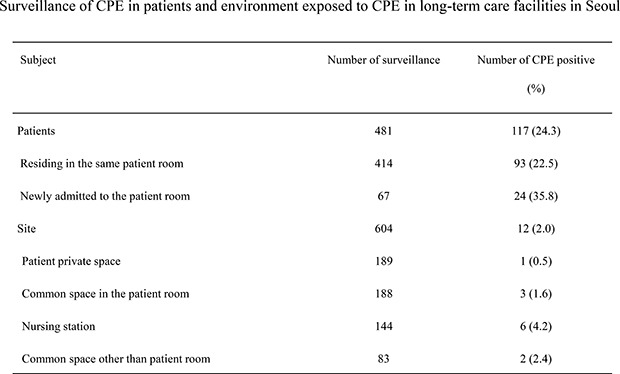
From 23 hospitals, 414 patients who had resided in the same patient room as a patient with confirmed CPE and 67 patients who were newly admitted to that patient room were screened (Table 2). All screened patients in 10 hospitals showed negative results. In 13 hospitals, a total of 117 (24.3%) patients had positive results for CPE among which 93 (22.5%, 93/414) were already admitted patients and 24 (35.8%, 24/67) were newly admitted patients. Among the positive cases, 89 (76.1%) were detected in the first screening and 28 (23.9%) were detected on the second screening. Among the newly admitted patients, seven patients were known to be CPE colonized patients. Sixty patients were screened as unknown CPE status and 17 (28.3%) showed positive results.
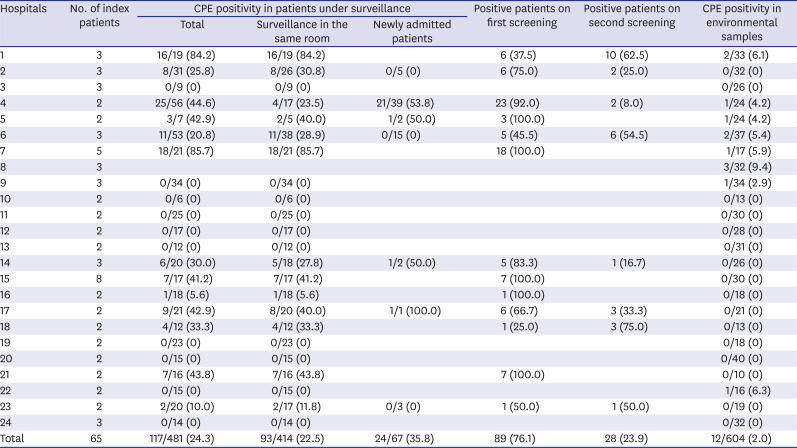
Table 2
Positivity rates of CPE among newly admitted and residing patients with a CPE confirmed patient and environment
![]()
From the 117 CPE positive patients, 163 CPE bacterial types were detected. Klebsiella pneumoniae (n = 104, 63.8%) was the most commonly detected bacteria followed by Escherichia coli (n = 43, 26.4%), Citrobacter koseri (n = 11, 6.7%), and Enterobacter aerogenes (n = 3, 1.8%) (Table 3). The most commonly detected CPE genotype was KPC which accounted for 90.8% (n = 148), followed by New Delhi metallo-β-lactamase (NDM) (n = 7, 4.3%), and oxacillinase-48 (OXA-48) (n = 7, 4.3%).

Table 3
Principal pathogens and associated carbapenemase type in the detected carbapenemase-producing Enterobacteriaceae
Values are presented as number (%).
KPC = Klebsiella pneumoniae carbapenemase, NDM = New Delhi metallo-β-lactamase, OXA = oxacillinase, IMP = imipenemase.
![]()
Table 4 shows the results of environmental sampling. Environmental sampling was performed in 24 hospitals. Environmental samples from 8 (33.3%) hospitals tested positive for CPE; among the samples from 13 hospitals where additional CPE infection-positive patients were identified, environmental samples from 5 (38.5%) hospitals tested positive. A total of 604 sites were sampled, which were classified as private space around the patients (n = 189, 31.3%), common space in the patient room (n = 188, 31.1%), nursing station (n = 144, 23.8%), and public space outside the patient room (n = 83, 13.7%). Overall, 12 sites demonstrated positive results for CPE accounting for 2.0% of the sampled sites. Nine out of 12 sites tested positive for KPC producing K. pneumoniae and three tested positive for Enterobacter cloacae; at one of sites the Enterobacter cloacae produced KPC while at the others, the bacteria produced Guiana extended-spectrum (GES)-5. The CPE positivity was highest in the nursing station (6 sites, 4.2%). All CPE detected in the nursing station were discovered in the sink. CPE were detected in three sites (1.6%) in the public space outside the patient rooms and one site each in the public space inside the patient room and private space around the patient (2.4% and 0.5%, respectively). Although all the screened patients exhibited negative results, environmental samples were positive in three hospitals.

Table 4
Results of environmental sampling for carbapenemase-producing Enterobacteriaceae
Values are presented as number (%).
aSide rail, side table, button in monitor, urine bag, O2 circuit, hemodialysis machine, personal cabinet, and ventilator; bRest room, washstand, refrigerator, blood pressure cuff, common chair, cart, air conditioner, radiator, window, remote control, medical waste container, entrance door, hand sanitizer at entrance; cSink, prescription counter, telephone, mouse, keyboard, refrigerator, medicine cabinet; dRail bar in the hallway, medical waste container, refrigerator, dressing cart, water purifier, rest room, shower room, physical therapy room, treatment room, pantry.
![]()
Go to :
DISCUSSION
We discovered that the proportion of CPE colonization in patients who were exposed to CPE positive patients in LTCFs was 24.3%. Despite the importance of infection prevention in LTCFs, there is no data pertaining to CPE colonization and acquisition in LTCFs in Korea.17 To the best of our knowledge, this is the first report about this issue in Korea.
The prevalence of CRE is between 0.3% to 7.5% in acute care hospitals in Korea and the proportion of CPE has been increasing steadily accounting for 68.6% of the CRE in 2018.122021222425 Previous studies performed in acute care hospitals almost always targeted ICUs and utilized clinical samples. This differs from our study, since we investigated CPE colonization by rectal swabs in exposed patients in LTCFs. In a study examining CPE acquisition rates among close contact patients who were inpatients in a tertiary hospital in Korea, the acquisition rate was 3.2%.26 In comparison, except for newly admitted patients, the positive rate was 22.5% in our study for patients sharing the same patient room. Therefore, it was higher in LTCFs than after exposure in a tertiary acute care hospital. This suggests a situation in which infection control measures, such as maintaining distance between beds and hand hygiene, are poorly implemented in LTCFs compared to acute care hospitals. In a study conducted on patients transferred from LTCFs to tertiary hospitals, active surveillance for CRE was performed but only 1.4% patients were found to be CRE positive. In addition, none of them were CPE positive.27 Consequently, it is thought that screening all patients transferred from LTCFs is ineffective in terms of cost-effectiveness. The results of our study show that there was a high proportion of CPE colonized LTCFs patients who may potentially be hospitalized in acute care hospitals. Further studies on surveillance methods and their efficiency should be conducted. Since this study did not compare the molecular type of the index patients and the patients who became positive after exposure, it is not clear whether the condition was acquired after exposure in the LTCFs or if existing bacteria were confirmed during testing. However, our study findings confirmed that a significant proportion of patients in LTCFs in Korea are already colonized with CPE.
LTCFs act as a bridge to acute care hospitals and are a potential reservoir for CPE. By preventing CPE infections in LTCFs, CPE transmission can be blocked not only in LTCFs but also in acute care hospitals. Several countries have enforced infection prevention measures in LTCFs which include active surveillance.1819 As a result, the prevalence of CPE has declined in LTCFs as well as in acute care hospitals. For nationwide CPE infection prevention, LTCFs should be targeted as a policy. However, there was lack of a policy targeting LTCFs for infection prevention in Korea. Moreover, active surveillance is difficult in LTCFs because of cost and a time-consuming detection technique. Even in patients exposed to CPE infected patients, surveillance was not routinely performed in LTCFs. However, as 24.3% of patients exposed to CPE demonstrated positive CPE colonization, there is a risk of CPE transmission increasing explosively if these patients are not well controlled. In addition, 28.3% of newly admitted patients were positive for CPE. We could not determine whether samples were obtained at the time of admission or a few days after admission. Among newly admitted patients, most cases of CPE except for two, were detected on the first screening. Considering the evaluation intervals, the sampling was conducted within a week of admission. This could mean that, possibly, many patients were either CPE carriers at the time of admission (acquired from other hospitals/sites), or acquired the infection within a week from a CPE positive patient in this hospital. This indicates the importance of management of newly admitted patients since there was a risk of colonization even in newly admitted patients. This suggests extra precautions are needed to avoid contamination in the ward where the patients with CPE are placed. Overall, infection prevention measures targeting LTCFs should be more concrete and strictly enforced.
Environment was another reservoir for this multidrug-resistant organism and thought to be one of the routes of hospital transmission.28 Bedside was considered contaminated with these bacteria in infected patients and the space near the patients was also easily contaminated. In this study, environmental contamination rate was 2.0%. Most of the contaminated area was in the nursing station, especially in the sink, which was not close to the patient. After patient care, any bodily fluids were discarded in the sink in the nursing station and therefore this may have been the cause of sink contamination. As this study could not analyze molecular types and factors that affect patient colonization, it could not be determined whether environmental contamination leads to patient transmission and colonization. In addition, although there were no CPE colonized patients, CPE was detected in the environmental samples from three LTCFs. Our results suggest that environmental contamination does not necessarily induce patient colonization and cross-contamination. However, CPE was detected in the environment of hospitals; these hospitals comprised 38.5% of the hospitals where additional positive patients were identified. Although the role of environmental contamination on CPE transmission was not clear, it appears the surrounding environment was a reservoir for CPE. Therefore, environmental contamination should be reduced by proper sterilization and the relationship between surrounding environments and CPE transmission should be further studied.
Among the patients positive for CPE colonization, 23.9% were not detected in the first sampling but were only detected after the second sampling. This indicates that the detection of positive patients could be either because of infection prevention not being properly performed in that patient room or owing to the presence of other risk factors such as antibiotics exposure. Since we could not assess the risk factors, we could not make a conclusion. However, because of this risk, infection prevention and antibiotic usage monitoring should be properly performed. After CPE detection, proper infection prevention can be achieved with patient cohorting, periodical surveillance, and repeated education.
K. pneumoniae was the most prevalent pathogen among the detected CPE accounting for 63.4%, followed by E. coli (26.2%). This was similar to the Korean national surveillance report.12 In the report, K. pneumoniae was the most common pathogen (65.2%), followed by E. coli (17.2%) and Enterobacter spp. KPC was the most common genotype (90.8%). In the national survey, KPC was also the most common genotype but the proportion was slightly lower (73.3%).
This study has some limitations. Firstly, we could not collect the patient characteristics. There are many factors that can affect CPE colonization. However, we could not analyze the risk factors. Secondly, since this study only included LTCFs in Seoul, it is difficult to interpret and generalize the results to the entire region of Korea. Therefore, a national survey of LTCFs is necessary. Thirdly, as already mentioned, the molecular type was not confirmed. Consequently, it was difficult to confirm whether a positive result obtained was after exposure, or if the patient was already a carrier and confirmed positive through testing in this study. Finally, environmental sampling was performed only once at the initial visit and because repeated environment sampling could not be performed, the effect of cleaning on CPE is unclear. In addition, we could not analyze the association between environmental contamination and CPE colonization.
In conclusion, the CPE colonization rate in patients exposed to CPE in LTCFs was higher than that at acute care hospitals. Proper infection control measures for detecting and reducing CPE in patients residing in LTCFs are needed. Newly admitted patients could be carriers; therefore, infection control for newly admitted patients needs to be thorough.
Go to :
 XML Download
XML Download