This article has been
cited by other articles in ScienceCentral.
Abstract
Coronavirus disease 2019 (COVID-19) is a respiratory syndrome caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and emerged in Wuhan, China, in late 2019. It resulted in a worldwide pandemic, and spread through community transmission in the Republic of Korea (ROK). In the ROK, SARS-CoV-2 is categorized as a first-degree infectious disease of the legal communicable disease present. The Korean Society for Legal Medicine (KSLM) is the sole official academic association of forensic professionals in the ROK. As such, this society has played an important role in forensic medicine and science in the ROK. Therefore, KSLM suggests a standard operating procedure for the postmortem inspection in a focus on COVID-19. This article includes the background of this suggested standard operation procedure, basic principles for postmortem inspections of individuals suggested of having an infectious disease, and specific procedures according to the probability level of SARS-CoV-2 infection.
Go to :

Graphical Abstract
Go to :
Keywords: SARS-CoV-2, Postmortem Inspection, Standard Operating Procedure, Republic of Korea
INTRODUCTION
Post-mortem inspection is an external examination of a dead person and is performed to determine the cause and manner of death. Although identifying unnatural death is the main objective of a post-mortem inspection, natural death also accounts for a large percentage of actual post-mortem inspection cases. In general, patients who die from infectious diseases, including coronavirus disease-19 (COVID-19), are not subject to post-mortem inspection because they passed away while being treated in medical institutions. However, if the cause and manner of death of the patient with confirmed COVID-19 cannot be determined, the cause and manner of death needs to be clarified, and post-mortem inspection should be conducted. Furthermore, patients with suspected COVID-19 or limited clinical information and a history of exposure to COVID-19 may be subject to post-mortem inspection, and quarantine and preventive measures should be taken to prevent infection and transmission from latent COVID-19.
As COVID-19 has become a global pandemic, and community transmission continues, undiagnosed or latent COVID-19 cannot be ruled out in post-mortem inspection cases. Vulnerable groups, such as those with chronic diseases, those living alone, and the elderly, account for a large proportion of the post-mortem inspection cases. Therefore, post-mortem inspection guidelines for infection prevention, including COVID-19, should be prepared in advance.
The Korean Society for Legal Medicine, a highly specialized organization responsible for post-mortem examination and death investigation, aims to protect multiple staff-related post-mortem examinations and prevent the spread of COVID-19 in medical institutions and communities to improve social stability through this guideline for COVID-19 post-mortem inspections.
Go to :
BASIC PRINCIPLES
Risk of infection during post-mortem inspection
Currently, in the Republic of Korea, post-mortem inspection is conducted at the death scene, emergency room, or morgue. The risk of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection during post-mortem inspection of a dead body is relatively lower than that in the case of medical procedures or treatments because dead bodies do not cough and spread droplets. However, an examination of the nostrils and oral cavity is essential during post-mortem inspection. Infectious materials like body fluids can be spilled from nostrils, mouth, and anus of the dead body, and can be existing around it. The house of a dead person and the field at which post-mortem inspection is performed can be contaminated. Furthermore, doctors who perform post-mortem inspections interview the family or the persons who closely contacted the deceased, so the risk of infection surely exists during post-mortem inspection.
Infectability of SARS-CoV-2 in post-mortem cases
Infectivity persists for a certain period after the death of the host in most infectious diseases. For example, HIV-infected bodies should be considered infectious for at least two weeks after death. Hepatitis B virus (HBV) in the environment is also hardy. HBV in human plasma retains infectivity one week after drying and exposure to an ambient environment.
1 Post-mortem infection of SARS-CoV-2 has not been reported; however, the exact post-mortem infectivity remains unknown. Furthermore, the stability of SARS-CoV-2 was similar to that of SARS-CoV-1 when tested under experimental conditions. SARS-CoV-2 remained viable in aerosol for three hours. It was more stable on plastic and stainless steel than on cooper and cardboard, with a viability of 72 hours after application to these surfaces. Thus, aerosol and fomite transmission of SARS-CoV-2 is plausible since the virus can remain viable and infectious in aerosol for hours and up to days on surfaces (depending on the inoculum shed).
2 Moreover, SARS-CoV-2 can be detected in anal swabs and blood. The number of positive anal swabs was more than the number of positive oropharyngeal swabs in the later stage of the infection, suggesting shedding and thereby transmission through the oral-fecal route.
3 The persistence of SARS-CoV, which belongs to the family
Coronaviridae, the same as SARS-CoV-2, was observed in feces, urine, and water. In vitro experiments showed that the virus was viable for two days in hospital wastewater, domestic sewage, and dechlorinated tap water, three days in feces, fourteen days in phosphate buffer saline (PBS), and seventeen days in urine at 20°C.
4 Middle East respiratory syndrome coronavirus (MERS-CoV) can be detected in the nasal swab of an infected human cadaver (three days following death). In the case of patient death, the deceased should be treated as infectious and as having the ability to transmit the infection.
5 The analysis of 22 studies reveals that human coronaviruses such as SARS coronavirus, MERS coronavirus or endemic human coronaviruses can remain viable on inanimate surfaces such as metal, glass, or plastic for up to nine days.
6 Therefore, the possibility of infection during post-mortem inspection of a dead person who is suspected to be infected by SARS-CoV-2 should be kept in mind and is important to prevent a post-mortem transmission of SARS-CoV-2 considering the principles for living patients of SARS-CoV-2.
Review of previously reported guidelines
COVID-19 has spread worldwide, and major international organizations and health authorities in developed countries have prepared and reported guidelines for post-mortem examination of dead bodies with a high risk of infection.
7891011 However, the post-mortem investigation system differs among countries. The principles and methods of both the clinical approach and post-mortem investigation of COVID-19 are also different among countries. Therefore, it is impossible to accept these guidelines for the Republic of Korea, and these guidelines should be used as a reference. We used both guidelines for living patients of SARS-CoV-2 and international guidelines for the post-mortem investigation of SARS-CoV-2 as references.
General suggestions for the safe post-mortem inspection of a dead body due to infectious diseases
In almost all cases of unnatural death, medical history and traces of the past activity are unknown. The doctor is at risk of getting infected while performing a post-mortem inspection. Therefore, post-mortem inspection should be performed under the following basic principles to protect human resources and the local community from post-mortem infection resulting from post-mortem inspection procedures. For all unnatural deaths during an epidemic or a pandemic, a post-mortem caretaker wearing personal protective equipment (PPE) must cover the body following corpse handling guidelines. The external surfaces of the body bag must be sanitized and placed into a second bag for double sealing, and the bodies must be transported to the public morgue, which has safe facilities for protecting the local community from infection. Before post-mortem inspection is performed, infectious diseases must be diagnosed. Post-mortem inspection is performed by professionals according to the result of the diagnosis of infection.
This standard operating procedure distinguishes bodies according to the possibility of infection, considering the current situation in which human resources, systems, and facilities are inadequate in the Republic of Korea. The laboratory test for diagnosis of COVID-19 was conducted according to the decision of the doctor and investigating professionals. However, the following conditions should be fulfilled to protect the post-mortem caretaker and the local community from post-mortem infection; a public morgue which has safe facilities; diagnosis of infection for all unnatural deaths before post-mortem inspection; right to inquire the past medical history of the deceased from the doctor who performs a post-mortem inspection.
Go to :
PRACTICE GUIDELINES ON POST-MORTEM INSPECTION OF BODIES RELATED TO COVID-19
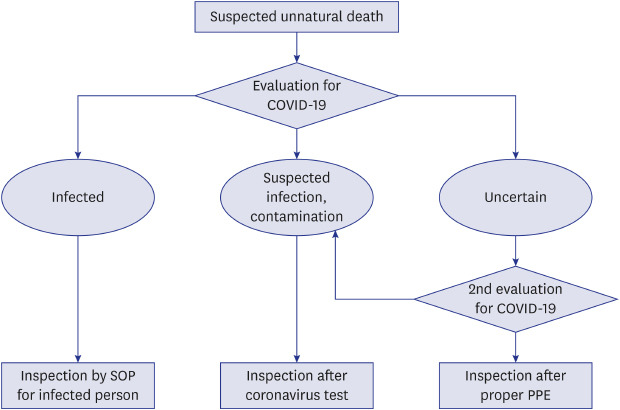
Bodies related to COVID-19 can be divided into three categories: bodies confirmed as COVID-19; bodies that may be infected; and bodies with no or insufficient information related to death, including COVID-19 (
Fig. 1). To classify patients according to the likelihood of infection, SARS-CoV-2 evaluation must first be performed. Due to the nature of post-mortem inspection, in most cases, there is no or insufficient ante-mortem information, so collaboration with investigative agencies, local governments, and relevant public health centers is essential to determine the possibility of SARS-CoV-2 infection. Identification of the deceased should be preceded, and based on this, it is necessary to check whether he or she was registered as a subject to manage patients in a local health center. Additionally, investigations of the past and current medical history, as well as the people who surrounded the deceased, should be conducted.
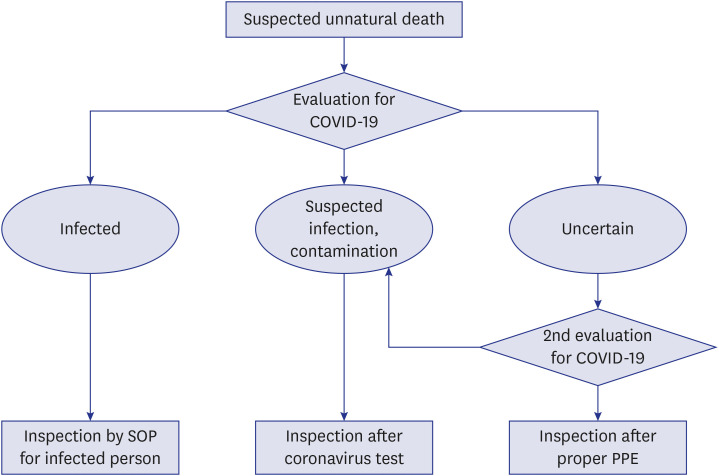 | Fig. 1
Flowchart for the post-mortem inspection of the deceased with a suspected unnatural cause of death related to COVID-19.
SOP = standard operating procedure, COVID-19 = coronavirus disease 2019, PPE = personal protective equipment.

|
Post-mortem inspection of bodies confirmed as COVID-19
If a diagnosed patient dies from COVID-19, it is not subject to post-mortem inspection. However, if it is not possible to determine whether the patient died of COVID-19, or if the patient died from a cause of death other than COVID-19, especially if the death was following the unusual death guidelines published by the Korean Society for Legal Medicine, post-mortem inspection should be carried out. The following are the types of death that require detailed investigation according to the unusual death guidelines of the Korean Society for Legal Medicine:
- Crime-related or suspected deaths
- Any accidental deaths
- Suicidal or suicide-suspected deaths
- Decomposed or unidentified bodies
- Underwater bodies and deaths associated with fire accidents
- Death in custody, including taking to a police station, detention, interrogation, detention centers and prisons
- Deaths in collective welfare accommodations such as mental health facilities and orphanages
- Deaths of young and old people who seemed to be healthy but died suddenly
- Deaths of infants, children, and adolescents who are not being treated by medical institutions
- Deaths suspected due to acute poisoning
- Deaths of unknown cause at a medical institution
1) Subject: The deceased who was confirmed according to the diagnostic criteria for COVID-19 (virus isolation and SARS-CoV-2 gene polymerase chain reaction test) regardless of clinical features.
2) Post-mortem inspection should be conducted with minimum manpower, comprising one medical doctor and one member of an investigative agency, and the additional necessary personnel is decided according to the situation.
3) Wear appropriate PPE before entering the site of post-mortem inspection.
A. Required PPE (Level D): KF94 (or N95) mask, gloves, goggles (or face shield) and full body protective clothing (including shoe covers, boots if wearing disposable gowns)
B. Disinfect your hands with hand sanitizer (containing 60%-95% alcohol) before and after wearing PPEs.
4) If necessary, conduct interviews with related persons (family, witnesses, reporters, etc.), and minimize contact with those at risk of infection (call interviews, interviews in separate spaces, interviews after keeping safe distance [more than 2 m]).
5) Perform post-mortem inspection according to standard procedures.
6) After completing the postmortem inspection, the body is packed in a leak-proof plastic bag by specialists, put back into the body bag, followed by sterilization of the body bag surface.
12
7) Wastes such as PPEs are disposed off in a previously prepared waste collection bag according to the prescribed procedures (see section 4. Waste management).
8) Fill out and submit the ‘Death (post-mortem inspection) report for infectious patient’.
13
Post-mortem inspection of bodies that may be infected with COVID-19
1) Subject: The deceased who was managed as a suspected patient, a patient under investigation and a person in contact with suspected patients before death. Each definition is as follows.
A. Suspected patient: A person who displayed clinical symptoms (fever of more than 37.5°C or respiratory symptoms such as cough and dyspnea) within 14 days of contact with a confirmed COVID-19 patient
-
B. Patient under investigation:
• A person suspected of having COVID-19 according to a physician's opinion based on clinical symptoms of COVID-19
• A person with an overseas travel history displaying clinical symptoms of COVID-19 within 14 days upon entry in Republic of Korea
• A person exhibiting clinical symptoms of COVID 19 within 14 days of an epidemiological link to a domestic COVID-19 cluster
C. Person in contact with confirmed patients: A person who has been in contact with a confirmed patient, and has been confirmed through an epidemiological investigation at the local public health center.
2) After confirming the identity of the deceased, if it is necessary to confirm whether he or she has the possibility of infection with COVID-19, request confirmation to the public health center.
3) In principle, a coronavirus test is referred to the local public health center and post-mortem inspection should be performed according to the results.
Post-mortem inspection of bodies with no or insufficient information related to death
1) After confirming the identity of the deceased, if it is necessary to confirm whether he or she has the possibility of infection with COVID-19, request confirmation to the public health center through the police in charge, and proceed with the post-mortem inspection.
2) Before the post-mortem inspection is started, the possibility of infection should be confirmed through interviews with relatives and close contacts of the deceased.
3) If COVID-19 cannot be ruled out reliably, the deceased should always be considered as a corpse that may be infected with COVID-19, and post-mortem inspection should be carried out while wearing appropriate PPE.
A. Wear equipment for appropriate respiratory protection (medical mask), full body protection (gloves, a disposable waterproof long sleeve gown), and eye protection (goggles or a face shield).
B. Be cautious about wearing PPE, as there is a possibility of self-containment through epidemiological investigations if the deceased is found to be an infected person after postmortem inspection (based on the work standard of medical staff contacting COVID-19 patients, the recommended monitoring is self-monitoring level because medical personnel wearing all the recommended protective equipment have a low exposure risk when handling or contacting the patient's secretions and feces).14
-
C. In the process of post-mortem inspection, if the body is found to be or seem to be infected, immediately report it to the public health center through the police in charge and, if necessary, fill out an infectious disease report.13
• If you did not wear adequate protective equipment, report it to the public health center and enter quarantine.
• If the test result of the deceased is negative, immediately discontinue the quarantine, and if positive, maintain quarantine for 14 days (even if there are no symptoms, the test is conducted on the 13th day of containment to confirm that it is negative, the person is released on completion of the 14-day containment).
Go to :
TESTING FOR COVID-19
(1) If it is determined during the post-mortem inspection that testing for COVID-19 is necessary, report it to the public health center for cooperation with the health authority and the investigative agency.
(2) If samples are to be taken from the corpse, follow the COVID-19 guidelines for safe sampling and handling of samples published by the Korea Centers for Disease Control and Prevention (KCDC).
15
Go to :
WASTE MANAGEMENT
(1) Medical wastes such as protective equipment should be disposed off in a separate waste bag and notified to the public health center if post-mortem inspection and specimen sampling are performed in the residence of a deceased person.
(2) Use the waste disposal facility within the medical institution, if the post-mortem inspection and specimen sampling are performed at a hospital (example, an emergency room or a morgue).
(3) Waste should be handled according to the general guidelines of the KCDC.
17
Go to :
CONCLUSION
It is reasonable to focus primarily on the prevention, diagnosis and treatment of living patients when new infectious diseases are prevalent. However, to improve the quarantine and preventive system, proper management of the deceased person with known or suspected COVID-19 should be done, and appropriate protection and diagnosis should be taken during the post-mortem inspection. In Republic of Korea, unusual death cases are managed by the judiciary system, not by medical professionals or the health authority, and quarantine is overlooked during the post-mortem examination process. Therefore, these guidelines will improve the preventive and quarantine process.
Go to :
ACKNOWLEDGMENTS
This article is based on a study first reported in the Korean Journal of Legal Medicine, volume 44, 2020, as “Na JY, Noh SJ, Choi MS, Park JP. Standard Operating Procedure for Postmortem Inspection in a Focus on Coronavirus Disease-19: The Korean Society for Legal Medicine”.
Go to :
Notes
Go to :
References
1. Nolte KB, Taylor DG, Richmond JY. Biosafety considerations for autopsy. Am J Forensic Med Pathol. 2002; 23(2):107–122. PMID:
12040252.

2. van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020; 382(16):1564–1567. PMID:
32182409.
3. Zhang W, Du RH, Li B, Zheng XS, Yang XL, Hu B, et al. Molecular and serological investigation of 2019-nCoV infected patients: implication of multiple shedding routes. Emerg Microbes Infect. 2020; 9(1):386–389. PMID:
32065057.
4. Wang XW, Li JS, Jin M, Zhen B, Kong QX, Song N, et al. Study on the resistance of severe acute respiratory syndrome-associated coronavirus. J Virol Methods. 2005; 126(1-2):171–177. PMID:
15847934.
5. Mahallawi WH. Case report: Detection of the Middle East respiratory syndrome corona virus (MERS-CoV) in nasal secretions of a dead human. J Taibah Univ Med Sci. 2017; 13(3):302–304. PMID:
31435338.
6. Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect. 2020; 104(3):246–251. PMID:
32035997.
7. World Health Organization. Infection prevention and control for the safe management of a dead body in the context of COVID-19 (Interim guidance). Updated 2020. Accessed March 30, 2020.
https://apps.who.int/iris/handle/10665/331538.
10. Finegan O, Fonseca S, Guyomarc’h P, Morcillo Mendez MD, Rodriguez Gonzalez J, Tidball-Binz M, et al. International Committee of the Red Cross (ICRC): General guidance for the management of the dead related to COVID-19. Forensic Sci Int. 2020; 2:129–137.
13. National Law Information Center. Enforcement Decree of Infectious Disease Control and Prevention Act. Updated 2020. Accessed May 1, 2020.
http://www.law.go.kr/.
16. National Law Information Center. Korea Centers for Disease Control and Prevention Test Request Regulation. Updated 2020. Accessed May 1, 2020.
http://www.law.go.kr/.
Go to :


 PDF
PDF Citation
Citation Print
Print



 XML Download
XML Download