

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial arrhythmia (AA) is commonly seen in various clinical conditions. Although observational studies have found that traditional and non-traditional cardiovascular risk factors contribute to triggering AA,12 the mechanism causing AA is still unclear. Among risk factors, cigarette smoking may cause cardiac arrhythmias through the combined effects of nicotine, carbon monoxide, and pro-cyclic aromatic hydrocarbons.34 In particular, nicotine may increase susceptibility to catecholamine and consequently cause pro-arrhythmic atrial fibrosis.5
Until now, there has been a paucity of studies related to smoking and AA, other than a study of the association between smoking and supraventricular tachyarrhythmia in myocardial infarction patients with implanted cardioverter defibrillators.5 Meanwhile, there have been several studies assessing the effects of cigarette smoking on atrial fibrillation (AF) that found conflicting results6789 and were mostly based on self-reported questionnaires.567810 Previous studies have reported misclassification of smoking status between self-reported questionnaires and biomarker verification.1112
Cotinine, the main metabolite of nicotine, is extensively used as a biomarker for assessing actual cigarette smoking status. Urinary cotinine concentration offers an easy-to-use screening method of exposure to cigarette smoking that is non-invasive. Furthermore, previous studies have reported that urinary cotinine level is highly correlated with plasma cotinine level.1314
Therefore, this study evaluated the relationship between self-reported and urinary cotinine-verified smoking status and AA in a large Korean population.
METHODS
Study population
A total of 231,051 individuals who participated in the Kangbuk Samsung Health Study (KSHS) between 2011 and 2015 and received urinary cotinine measurement and electrocardiography (ECG) examinations were screened. The KSHS is a retrospective cohort study of adult Korean men and women who underwent a comprehensive annual examination at Total Healthcare Centers of Kangbuk Samsung Hospital. Among them, 29,263 were excluded because of history of atherosclerotic cardiovascular disease or abnormal ECG findings such as premature ventricular complex and bundle branch block. Ultimately, 201,788 individuals (men, 106,375; mean age, 37.4 ± 7.4 years) were enrolled in this study. Among these individuals, 12,803 were excluded from the self-reported smoking analysis because of missing data on their self-reported smoking questionnaires.
Smoking assessment
Data on smoking status were collected through a self-administered questionnaire. Smoking status was categorized as never, former or current smokers. Smoking status was classified according to the answer to this question: ‘How much have you smoked in your life until now in total?’ Never smokers were individuals who answered ‘No, I have not ever smoked’ or ‘I have smoked less than 5 packs in my life but I do not smoke’, former smokers were those who answered ‘I have smoked more than 5 packs but I do not smoke’, and current smokers were those who smoke.
Urinary cotinine concentration was determined using the DRI Cotinine Assay (Microgenics Corp., Fremont, CA, USA) with a modular P800 (Roche Diagnostics, Tokyo, Japan). A cotinine- verified current smoker was defined as having a urinary cotinine level of 50 ng/mL or higher by applying the Society for Research on Nicotine and Tobacco (SRNT) 2002 recommendation.1516 In our previous report, a urinary cotinine cut-off value of 50 ng/mL showed high sensitivity (84.8%) and specificity (98.2%) for distinguishing current from never smokers.15 Procedures of anthropometric and laboratory measurements were the same as those described in our previous studies.17
AA ascertainment
On the day of the urinary cotinine test, a standard supine 12-lead surface ECG was performed and interpreted by experienced cardiologists. AA was defined as atrial premature complex, non-sustained or sustained atrial tachycardia, atrial flutter, paroxysmal supraventricular tachycardia, and AF.
Statistical analysis
Data are expressed as mean ± standard deviation (SD) or median (interquartile range) for continuous variables and as a percentage (%) for categorical variables. Continuous variables were expressed as mean ± SD for normally distributed variables or as median and interquartile range if not normally distributed. Among the variables, serum thyroid stimulating hormone (TSH), triglycerides, high-sensitivity C reactive protein (hs-CRP), daily alcohol consumption (grams), and urinary cotinine were log-transformed for analysis to correct for skewed distributions, but data in tables are expressed as untransformed data for ease of interpretation. The prevalence of self-reported smoking status and cotinine-verified smoking status was determined using descriptive statistics. Characteristics were compared between two groups according to cotinine-verified smoking status and presence/absence of AA using either the Student's t-test or the χ2-test. Characteristics were compared between three groups according to self-reported smoking status using analysis of variance (ANOVA) or χ2 tests. Post hoc comparisons between the three groups were performed with Scheffe's multiple comparison test. Multivariate logistic regression analyses were performed to evaluate the relationship between self-reported and cotinine-verified smoking status, urinary cotinine quartile level (0–49 ng/mL, 50–601 ng/mL, 602–1,290 ng/mL, ≥ 1,291 ng/mL) and AA and AF. The multivariate model was adjusted for age, gender, body mass index, vigorous exercise (≥ 5 times/wk), daily amount of alcohol consumption, blood urea nitrogen, creatinine, uric acid, total cholesterol, high density lipoprotein-cholesterol, triglycerides, hs-CRP, free T4, and presence/absence of hypertension, and diabetes mellitus if variables of which the P value was < 0.05 in univariate analysis or clinical significant risk factors for AA or AF. Furthermore, the associations between daily amount (< 10, 10–19, ≥ 20 cigarettes/day) and duration of cigarette smoking (< 10 years, ≥ 10 years) and AA and AF were analyzed. Statistical analyses were carried out using IBM SPSS statistics version 24 (IBM Corp, Armonk, NY, USA), with a P value less than 0.05 considered statistically significant.
RESULTS
Prevalence of self-reported and cotinine-verified smoking and AA
The prevalence rates of self-reported never, former, and current smokers were 59.2%, 17.0%, and 17.5%, respectively. The prevalence of cotinine-verified current smokers was 18.2%. The prevalence rates of AA and AF were 0.3% and 0.1%, respectively.
Characteristics of self-reported/cotinine-verified smoking groups and AF/non-AF group
There were significant differences in characteristics between the three self-reported smoking groups for all variables (Table 1). The characteristics between cotinine-verified never smokers and current smokers were also significantly different for all variables (Table 2). In particular, self-reported former/current smokers had a higher prevalence of AF compared with self-reported never smokers (0.1% for former smokers, 0.1% for current smokers, and 0.02% for never smokers, P < 0.001), and cotinine-verified current smokers also had a higher prevalence of AF than cotinine-verified never smokers (0.1% vs. 0.06%, P = 0.006). The results of AA were consistent with the above results.
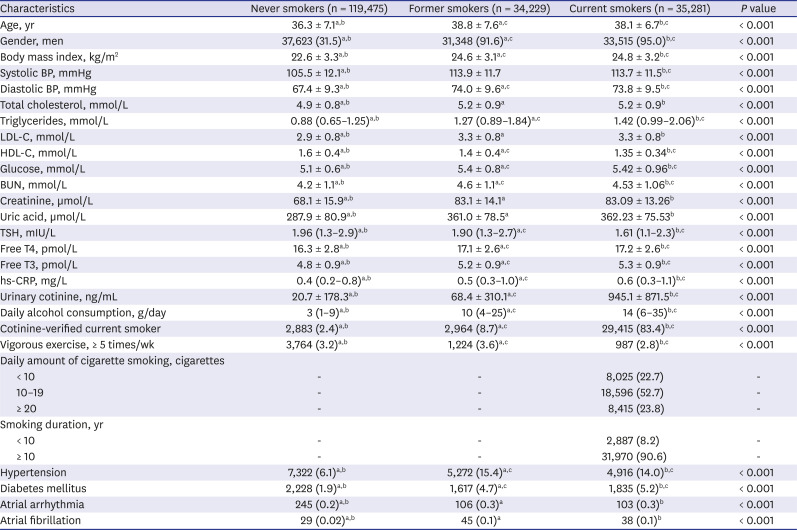
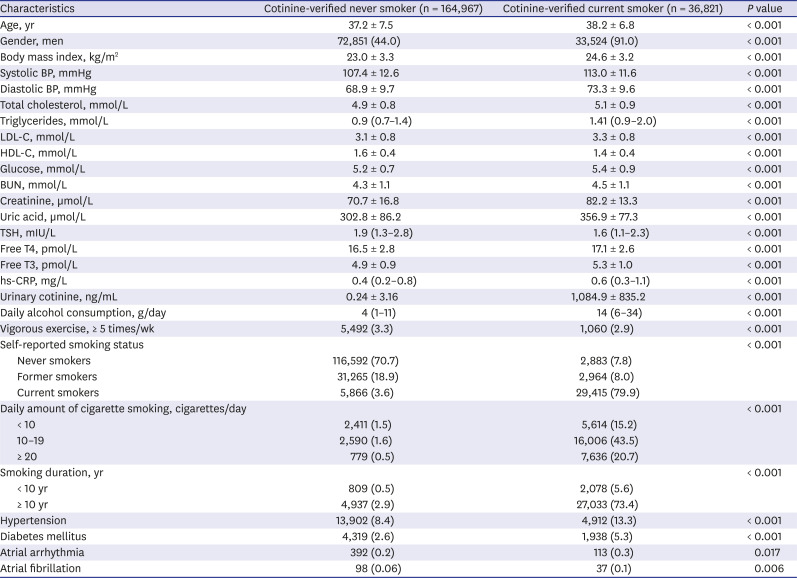
Table 1
Baseline characteristics of self-reported smoking groups
Values are given as mean ± standard deviation for normally distributed, median (interquartile range) if not normally distributed for continuous variables and number (%) for categorical variables. Serum TSH, triglycerides, hs-CRP, daily alcohol amount, and urinary cotinine were log-transformed for analysis.
BP = blood pressure, LDL-C = low-density lipoprotein cholesterol, HDL-C = high-density lipoprotein cholesterol, BUN = blood urea nitrogen, TSH = thyroid stimulating hormone, hs-CRP = high-sensitivity C-reactive protein.
P values based on one-way analysis of variance or χ2 test. Statistically significant (P < 0.05) by Scheffe's multiple comparison: anever smokers vs. former smokers, bnever smokers vs. current smokers, cformer smokers vs. current smokers.
![]()
Table 2
Baseline characteristics of cotinine-verified smoking groups
Values are given as mean ± standard deviation for normally distributed, median (interquartile range) if not normally distributed for continuous variables and number (%) for categorical variables. Serum TSH, triglycerides, hs-CRP, daily alcohol amount, and urinary cotinine were log-transformed for analysis.
BP = blood pressure, LDL-C = low-density lipoprotein cholesterol, HDL-C = high-density lipoprotein cholesterol, BUN = blood urea nitrogen, TSH = thyroid stimulating hormone, hs-CRP = high-sensitivity C-reactive protein.
![]()
Comparisons of characteristics between the two groups according to AF are presented in Table 3. The group with AF was older and had higher glucose levels and less favorable renal profiles, as well as a higher proportion of men, hypertension, and diabetes than the group without AF; they also had a higher proportion of self-reported former/current smokers and cotinine-verified current smokers, longer smoking duration (≥10 year), and greater daily amount of cigarette smoking (≥ 20 cigarettes/day), and higher urinary cotinine levels (329.03 ± 792.89 ng/mL vs. 198.0 ± 549.96 ng/mL, P = 0.023) compared to the group without AF. Comparisons of characteristics between the two groups according to AA are presented in Supplementary Table 1.
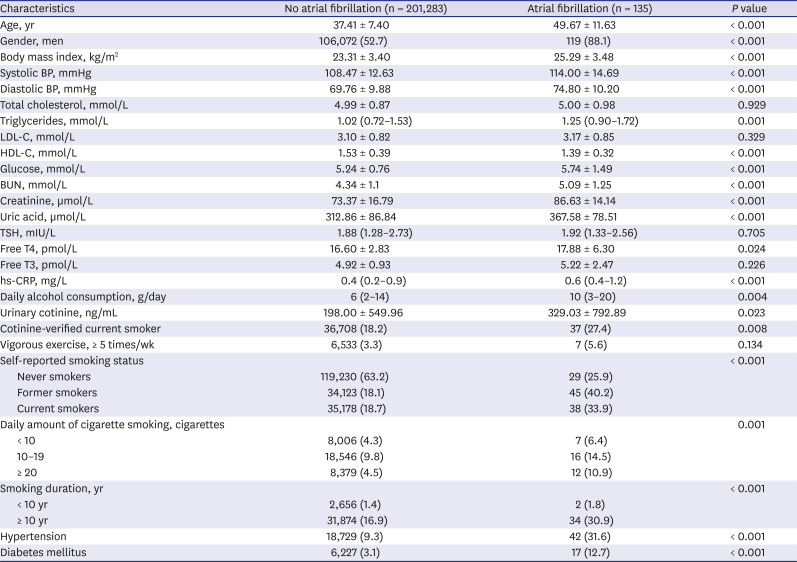
Table 3
Baseline characteristics according to atrial fibrillation
Values are given as mean ± standard deviation for normally distributed, median (interquartile range) if not normally distributed for continuous variables and number (%) for categorical variables. Serum TSH, triglycerides, hs-CRP, daily alcohol amount, and urinary cotinine were log-transformed for analysis.
BP = blood pressure, LDL-C = low-density lipoprotein cholesterol, HDL-C = high-density lipoprotein cholesterol, BUN = blood urea nitrogen, TSH = thyroid stimulating hormone, hs-CRP = high-sensitivity C-reactive protein.
![]()
Association of self-reported/cotinine-verified smoking groups with AA and AF
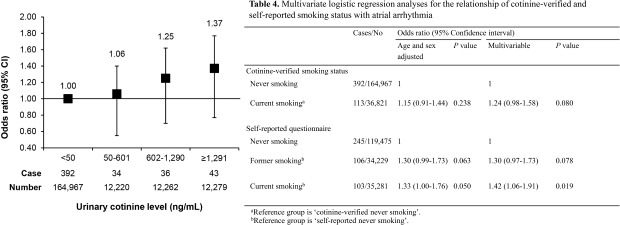
Multivariate logistic regression analyses for the relationship of cotinine-verified and self-reported smoking status with AA was shown in Table 4. Self-reported current smoking was significantly associated with AA compared with self-reported never smoking (odds ratio [OR], 1.42; 95% confidence interval [CI], 1.06–1.91; P = 0.019), whereas self-reported former smoking showed no significant association with AA (OR, 1.30; 95% CI, 0.97–1.73; P = 0.078). In particular, self-reported current smoking with ≥ 20 cigarettes/day and ≥ 10 years increased the risk for AA (P for trend, P = 0.012 and P = 0.035, respectively) and AF (P for trend, P = 0.047 and P = 0.028, respectively) compared with self-reported never smoking.
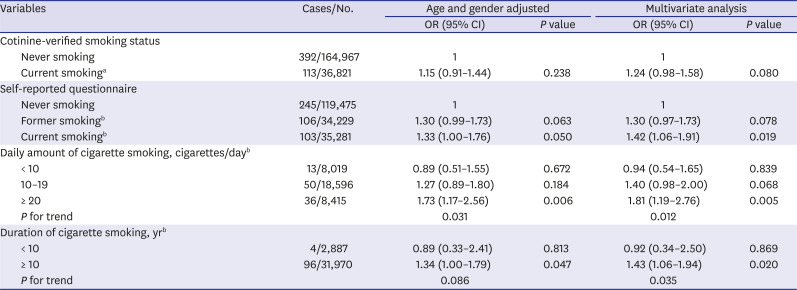
Table 4
Multivariate logistic regression analyses for the relationship of cotinine-verified and self-reported smoking status with atrial arrhythmia
Serum TSH, triglycerides, hs-CRP, daily alcohol amount were log-transformed for analysis. Multivariate model was adjusted for age, gender, body mass index, vigorous exercise (≥ 5 times/wk), daily alcohol amount, blood urea nitrogen, creatinine, uric acid, total cholesterol, high-density lipoprotein cholesterol, triglycerides, high-sensitivity C reactive protein, free T4 (3 groups), and presence of hypertension and diabetes.
OR = odds ratio, CI = confidence interval, TSH = thyroid stimulating hormone, hs-CRP = high-sensitivity C reactive protein.
aReference group is ‘cotinine-verified never smoking’; bReference group is ‘self-reported never smoking’.
![]()
Cotinine-verified current smoking is not significantly associated with AA (OR, 1.24; 95% CI, 0.98–1.58; P = 0.080) compared with cotinine-verified never smoking. However, as the cotinine quartiles increased, the OR for AA tend to increase linearly after multivariate logistic analysis (P for trend, P = 0.046) (Fig. 1). Meanwhile, cotinine-verified current smoking was not associated with the presence of AF compared with cotinine-verified never smoking (OR, 1.20; 95% CI, 0.79–1.83; P = 0.391), but self-reported current smoking showed an increased OR for AF compared with self-reported never smoking (OR, 2.20; 95% CI, 1.24–3.90; P = 0.007) (Table 5).
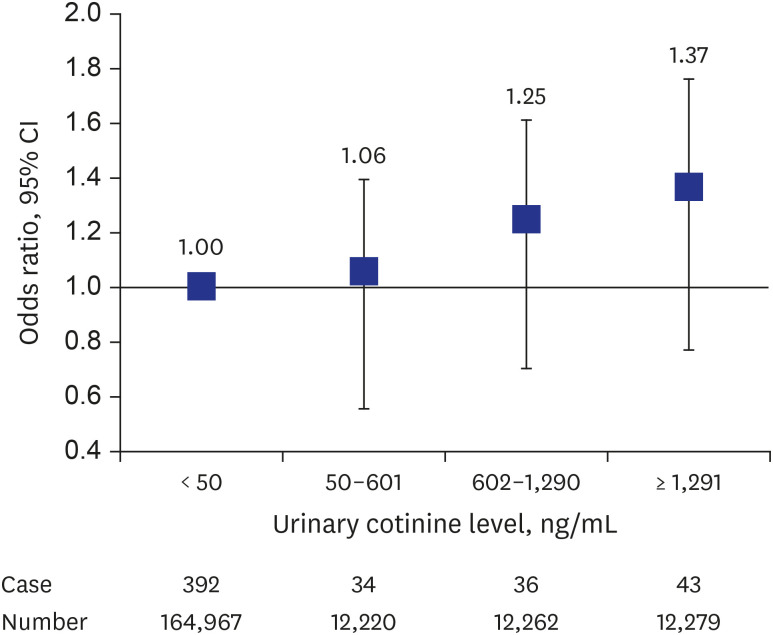
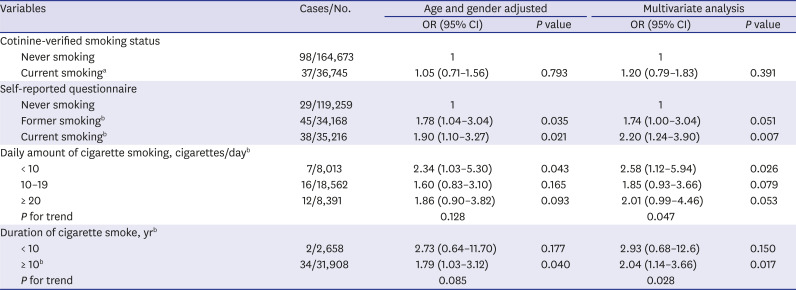
Fig. 1
Multivariate regression analyses for the association between cotinine quartiles and AA.
Multivariate logistic regression analyses showed that the OR for AA tend to increase linearly as the cotinine quartiles increased (P for trend, P = 0.046).
AA = atrial arrhythmia, OR = odds ratio, CI = confidence interval.
![]()
Table 5
Multivariate logistic regression analyses for the relationship of cotinine-verified and self-reported smoking status with atrial fibrillation
Serum TSH, triglycerides, hs-CRP, daily alcohol amount were log-transformed for analysis.
Multivariate model was adjusted for age, gender, body mass index, vigorous exercise (≥ 5 times/wk), daily alcohol amount, blood urea nitrogen, creatinine, uric acid, total cholesterol, high-density lipoprotein cholesterol, triglycerides, high-sensitivity C reactive protein, free T4 (3 group), and presence of hypertension and diabetes.
OR = odds ratio, CI = confidence interval, TSH = thyroid stimulating hormone, hs-CRP = high-sensitivity C reactive protein.
aReference group is ‘cotinine-verified never smoking’; bReference group is ‘self-reported never smoking’.
![]()
DISCUSSION
The main findings of the present study were as follows: 1) self-reported current smoking was significantly associated with AA and AF, but self-reported former smoking showed no significant association with AA and AF compared with self-reported never smoking; 2) cotinine-verified current smoking showed no significant association with AA but an increase in OR for AA as cotinine quartiles increased; 3) self-reported current smoking of ≥ 20 cigarettes/day and ≥ 10 years significantly increased the risk of AA by 81% and 43%, respectively, compared with self-reported never smoking.
Nicotine may promote arrhythmia through various mechanisms including marked elevations in serum catecholamine concentration, pro-fibrotic effects at the atrial level, direct blocking effects on inward KI1 channels, and significant increases in atrial interstitial fibrosis.18 Previous studies about the effect of nicotine on arrhythmia have been investigated in experimental canine models.1920 Supraventricular arrhythmia (83% of the experiments) was observed at increasing doses of intravenous nicotine in healthy anaesthetized dogs.19 In particular, nicotine caused a considerable increase in atrial fibrosis in dogs with experimentally induced myocardial infarction, promoting atrial flutter.20 In a study of myocardial infarction patients with implantable cardioverter defibrillators, inappropriate shock caused by supraventricular tachyarrhythmia was 3-fold higher in current smokers compared with former and never smokers.5
On the other hand, there have been several studies on the relationship between smoking and AF,7910 likely due to the clinical importance of fatal complications of AF, including stroke and heart failure. Although previous studies have shown inconsistent results, most of them have reported that smoking is associated with an increased risk of AF.710 We found that self-reported current smoking was associated with AA, including AF, whereas self-reported former smoking had no significant association with AA and AF. This result was in line with several previous studies that only current smoking, not former smoking, was associated with AF incidence.89 Some authors found that current smoking was associated with a risk of AF of about 40% using validated self-reported current smoking status ascertained by plasma cotinine.9 Another authors assumed that high total smoking consumption associated with AF was due to smoking-related atrial remodeling resulting from atrial fibrosis.8 In a study of 95 patients with known coronary artery disease undergoing bypass surgery, cigarette smoking measured as pack-years was an independent predictor of atrial fibrosis in smokers.18 Our results might represent the chronic effects of smoking on atrial fibrosis and remodeling over long durations (≥ 10 years) or with heavy smoking (≥ 20 cigarettes). This effect could be attenuated in the former smokers, resulting in a insignificant association with former smoking with AA and AF in our study. Therefore, these findings suggest that smoking cessation should be encouraged to prevent AA including AF.
In the present study, cotinine-verified current smoking as a binary variable showed no significant association with AA, which was slightly different from the results of self-reported current smoking. This difference may be attributed to the misclassification of smoking status. As shown in Tables 1 and 2, the prevalence of cotinine-verified never smokers among self-reported current smokers was 16.6%, whereas that of self-reported former and current smokers among cotinine-verified never smokers was 18.9% and 3.6%, respectively. This discrepancy can be caused by inaccurate reporting of actual smoking status, secondhand smoke exposure, or genetic variation of nicotine metabolism. Consequently, these factors could attenuate the association between cotinine-verified current smoking and AA. We further analyzed the association between current smoking and AA in individuals in the same category of smoking status according to self-reported questionnaire and cotinine verification. The group with both self-reported and cotinine-verified current smoking showed an increased risk of AA and AF compared with the group with both self-reported and cotinine-verified never smoking (OR, 1.44; 95% CI, 1.05–1.97; P = 0.021 for AA; OR, 2.05; 95% CI, 1.13–3.73; P = 0.018 for AF) (data not shown). This association was more obvious compared to the results according to each self-reported smoking status or cotinine-verified smoking status, which could suggest the importance of accurate assessment of actual smoking status.
Our study has several limitations. First, we could not establish a causal relationship between smoking and AA because of the cross-sectional design of this study. Second, in this study, the prevalence of AA and AF was relatively low. This is probably because most of our population was relatively young and apparently healthy. This low prevalence of AA and AF could have attenuated the statistical power. Third, a single ECG may have missed cases of paroxysmal or transient AA. Further studies using prolonged ECG monitoring such as 24-hour Holter or event recorder could validate more paroxysmal AF. Fourth, urinary cotinine is a major metabolite of nicotine, but harmful effects of other chemicals from cigarette smoking, including carbon monoxide, thiocyanate, and cyanide, were not evaluated. Fifth, the cut-off value for urinary cotinine to differentiate smokers from never smokers can vary depending on race and region. However, in our previous studies, the urinary cotinine level of 50 ng/mL showed a good sensitivity (98.2%) for the accuracy of self-reported never smokers and the rate of misclassification of actual smoking status was also less than 1.8%.21 Lastly, genetic variation such as CYP2A6 alleles that can affect nicotine metabolism could be potential confounders.
In conclusion, self-reported current smoking significantly increased the risk of AF as well as AA, and these results also showed a dose dependent association. Meanwhile, self-reported former smoking and cotinine-verified current smoking showed no significant association with AA. These findings suggest that quitting smoking could reduce the risk of AA. However, further longitudinal studies using both self-reported questionnaires and biomarker verification will be needed to clarify the risk of smoking status to the development of AA and AF.
 XML Download
XML Download