

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT-lymphoma) is a rare type of lymphoma that originates from the heterogenous small B-cells, including marginal (centrocyte-like) cells, centroblast-like cells, monocyte-like cells, small lymphocytes, and immunoblasts.1 MALT-lymphoma accounts for 24%–48% of all lymphomas and exhibits geographical variations.2 MALT-lymphoma, which is associated with the lymphatic system, develops in body organs that are devoid of organized lymphoid tissue.3 Persistent and chronic exposure to inflammation and infection can cause MALT in any part of the body.456 MALT-lymphoma is reported to occur at various sites, including the stomach, lung, skin, thyroid gland, salivary gland, and eye. The most common anatomical site of MALT-lymphoma development is the stomach, which accounts for 50%–70% of all MALT-lymphomas.78 Therefore, MALT-lymphoma is unofficially categorized into gastric MALT-lymphoma and non-gastric MALT-lymphoma. Infection with Helicobacter pylori is reported to be closely associated with the development of gastric MALT-lymphoma.9 In most cases, MALT-lymphoma is diagnosed at an early (localized) stage. However, the clinical treatment of MALT-lymphoma varies.1011
There are limited population-based studies on the incidence and survival rates of MALT-lymphoma, which may be attributed to the rare incidence of this type of lymphoma. One study reported the nation-wide incidence rates of MALT-lymphoma in the United States. However, the study did not provide any data on patient survival rates.8 Most studies reporting the survival rates of patients with MALT-lymphoma at various sites include small population sizes, such as a single-institute study.12131415 An understanding of the incidence and survival rates of MALT-lymphoma may aid in improving its therapeutic and preventive strategies. In this study, we analyzed the incidence and survival rates of MALT-lymphoma between 1999 and 2017 using data from the Korea Central Cancer Registry (KCCR), which supplied whole number of reported patients in Korea.
Go to : 
METHODS
The data were retrieved from the KCCR of the National Cancer Center (Goyang, Korea) after obtaining the necessary approval. The KCCR established the Korean National Cancer Incidence Database (KNCIDB), a population-based database of cancer occurrence.16 This database classifies cancer according to the International Classification of Disease for Oncology, third edition (ICD-O-3).17 The ICD code C88.4 was used to retrieve the registry data of MALT-lymphoma from the KNCIDB. The C88 code is used to define malignant immunoproliferative diseases and other B-cell lymphomas, including Waldenstrom macroglobulinemia (C88.0), heavy chain disease (C88.2), immunoproliferative small intestinal disease (C88.3), MALT-lymphoma (C88.4), other malignant immunoproliferative diseases (C88.8), and unspecified malignant immunoproliferative disease (C88.9).
The ICD code C88.4 was used to retrieve the data of 11,128 patients who were diagnosed with MALT-lymphoma between 1999 and 2017 from the KNCIDB. The primary site of MALT-lymphoma was not coded in this registry. The registry data included the age and sex of patients and the Surveillance, Epidemiology, and End Results (SEER) summary stages of the tumor. The SEER summary stages include localized, regional, distant, and unknown stages, which are used for categorizing the tumor stage in the KNCIDB.
The crude incidence rate was defined as the total number of newly diagnosed cases in a year divided by the mid-year population in Korea.18 The age-standardized incidence rate, which is the weighted average of the age-specific rates, was calculated using Segi's world standard population.1819 Relative survival is defined as the ratio of the survival rates of people who have a specific disease to the survival rates of those who do not have the disease. The relative survival rate (RSR) was adjusted for the expected mortality of the general population of the same age and sex. The RSRs were calculated using the Ederer II method.1820 The 5-year RSRs were calculated for the following time periods: 1996–2000, 2001–2005, 2006–2010, and 2011–2015. The 10ear RSRs were calculated for the following time periods: 1996–2000, 2001–2005, and 2008–2012. SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA) was used for statistical analysis.
Ethics statement
This study was approved by the Institutional Review Board of Wonju Severance Christian Hospital (CR319145), and the requirement of obtaining informed consent from individual patients was waived.
Go to :
RESULTS
Incidence
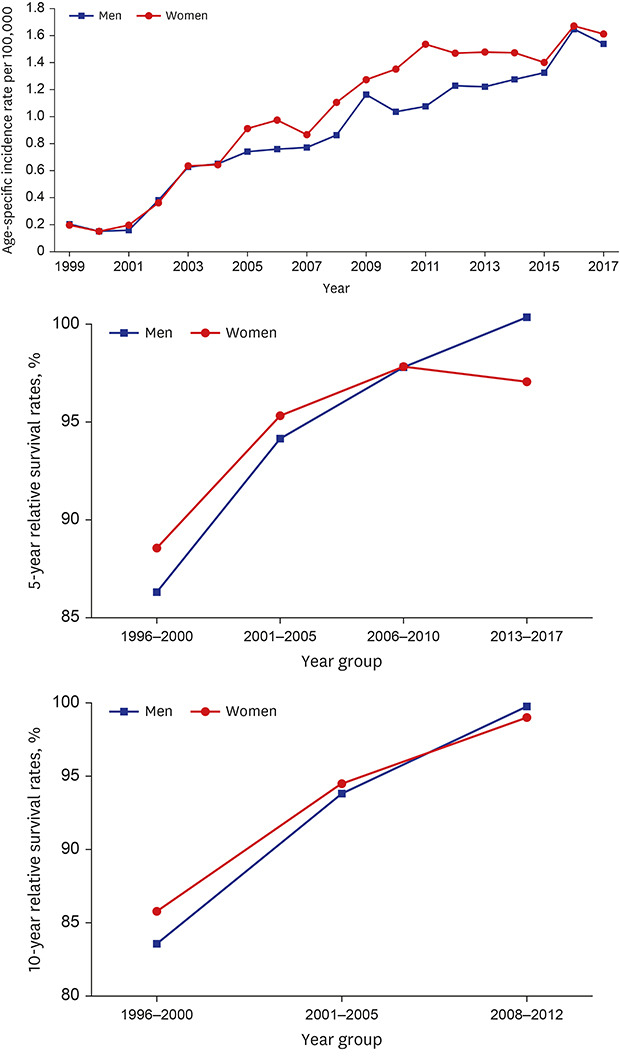
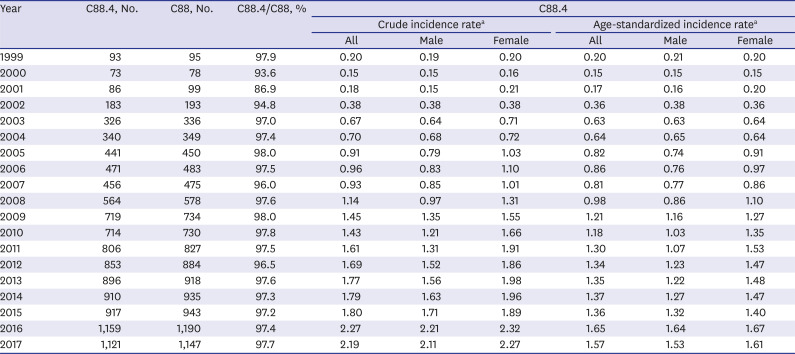
In Korea, the number of patients diagnosed with MALT-lymphoma (C88.4) increased gradually from the year 1999 (93 cases out of 46.4 million individuals) to the year 2017 (1,121 cases out of 51.4 million individuals) (Table 1). In 2017, the age-standardized incidence rates of MALT-lymphoma among males and females were 1.53 and 1.61 per 100,000 individuals, respectively. The number of affected patients, crude incidence rate, and age-standardized incidence rate increased during 1999–2017. The age-standardized incidence rate among female was slightly higher than that among males (Fig. 1). The incidence of MALT-lymphoma was the highest among patients aged 40–59 years (47.6%) (Fig. 2). Among the patients in the C88 group, the majority were patients with MALT-lymphoma (C88.4, 86.9%–98.0%).
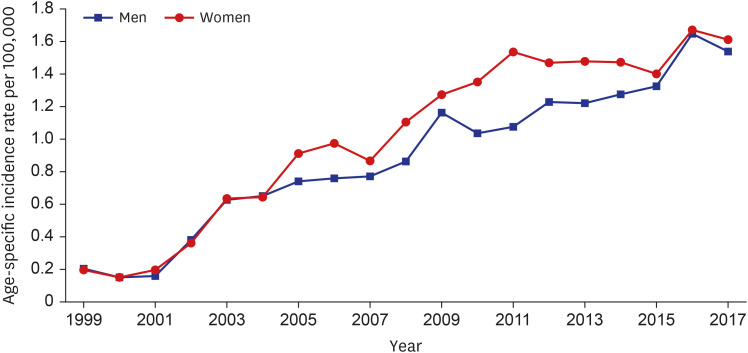 | Fig. 1The age-standardized incidence rate of extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue per 100,000 individuals between 1999 and 2017.
|
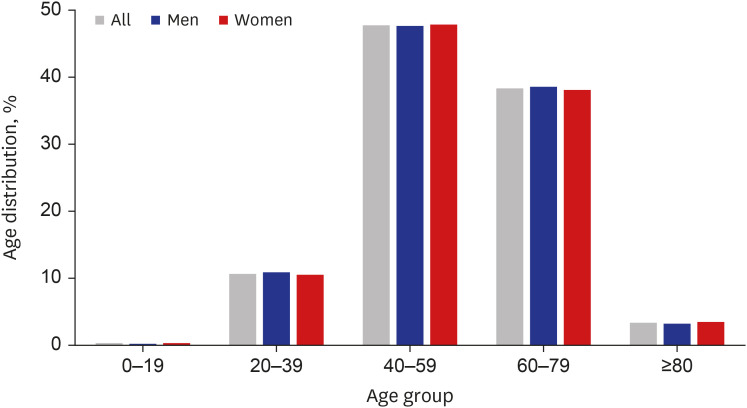 | Fig. 2The distribution of patients with extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue based on age groups (0–19, 20–39, 40–59, 60–79, and ≥ 80 years) in 2017.
|
Table 1
Incidence of patients with MALT-lymphoma between 1999 and 2017 in Korea
MALT-lymphoma = extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue.
aPer 100,000 person.
![]()
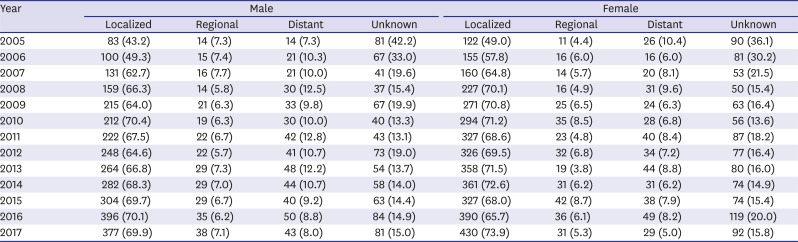
SEER summary stage of the tumor between 2005 and 2017
Based on SEER summary staging, most patients were diagnosed with localized stage MALT-lymphoma between 2005 and 2017 (Table 2). The proportion of patients with localized stage MALT-lymphoma among all the MALT-lymphoma cases increased gradually from 46.4% in 2005 to 71.9% in 2017 (Fig. 3). However, the proportion of patients with regional and distant stages of MALT-lymphoma among all the MALT-lymphoma cases was constant between 2005 and 2017.
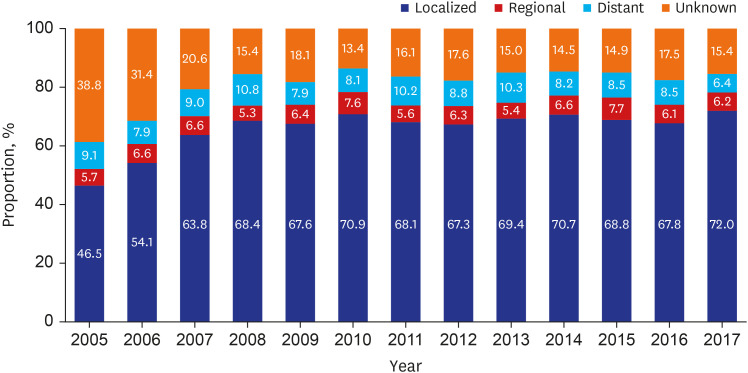 | Fig. 3The proportion of patients with various Surveillance, Epidemiology, and End Results summary stage extranodal marginal zone B-cell lymphomas of mucosa-associated lymphoid tissue between 2005 and 2017.
|
Table 2
SEER summary stage of MALT-lymphoma between 2005 and 2017
Data are presented as number (%).
SEER = Surveillance, Epidemiology, and End Results, MALT-lymphoma = extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue.
![]()
RSRs
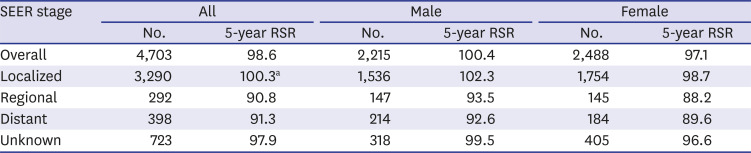
The RSRs decreased slightly from the year 1993 (99.1% in male and 98.9% in female at 1 year after diagnosis) to the year 2017 (98.1% in male and 97.0% in female at 10 years after diagnosis). The 5-year RSRs were 87.4%, 94.8%, 97.8%, and 98.6% in the specific time periods of 1996–2000, 2001–2005, 2006–2010, and 2013–2017, respectively. The 10-year RSRs were 84.7%, 94.2%, and 99.3% in the specific time periods of 1996–2000, 2001–2005, and 2008–2012, respectively. The 5-year RSRs gradually increased between the time periods of 1996–2000 and 2013–2017 in both male and female (Fig. 4), whereas the 10-year RSRs increased between the time periods of 1996–2000 and 2008–2012 (Fig. 5). The 5-year RSRs in females were higher than those in males in the time periods of 1996–2000, 2001–2005, and 2006–2010. However, males exhibited a higher RSR than females (100.4% vs. 97.1%) during 2013–2017. The 5-year RSR of patients with overall SEER summary stage lymphomas was 98.6% between 2013 and 2017. The 5-year RSR of patients with distant SEER stage lymphoma was 91.3% (Table 3). Among the patients with various SEER summary stage lymphomas, male exhibited a slightly better 5-year RSR than female.
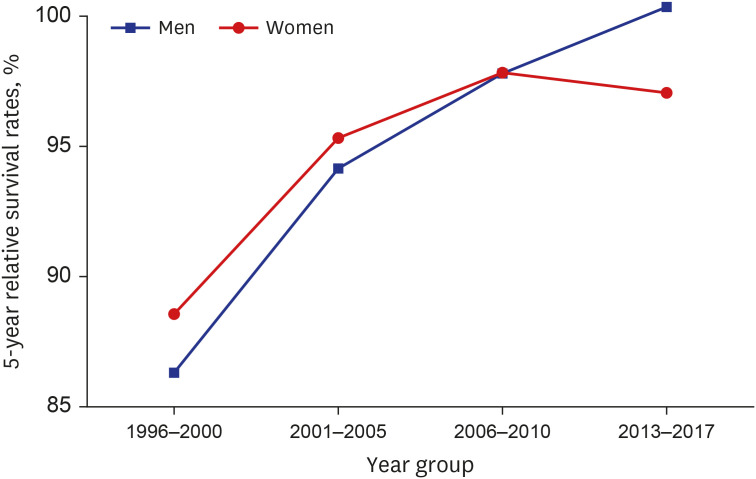 | Fig. 4The five-year relative survival rates of patients with extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue in different time periods (1996–2000, 2001–2005, 2006–2010, and 2013–2017).
|
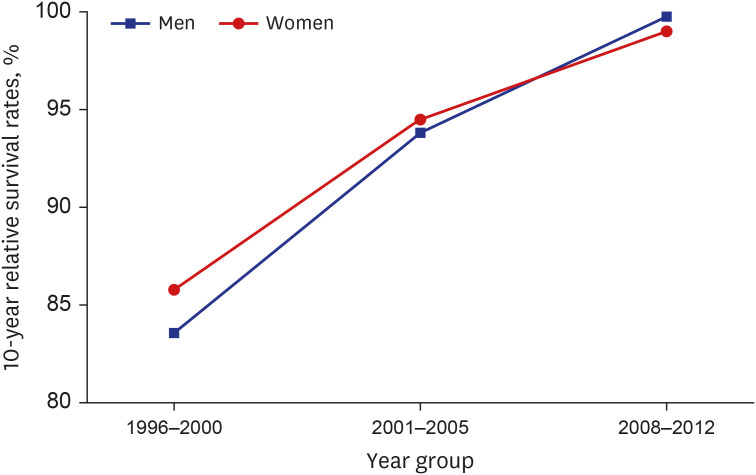 | Fig. 5The ten-year relative survival rates of patients with extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue in different time periods (1996–2000, 2001–2005, and 2008–2012).
|
Table 3
Five-year-RSR of patients with MALT-lymphoma by sex and SEER summary stage between 2013 and 2017
SEER = Surveillance, Epidemiology, and End Results, RSR = relative survival rate, MALT-lymphoma = extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue.
aCalculated RSR can be more than 100%.
![]()
Go to :
DISCUSSION
This study demonstrated that the incidence of MALT-lymphoma among the Korean population is low. Of the 51.4 million population in Korea in 2017, only 1,121 patients were diagnosed with MALT-lymphoma. Additionally, this study demonstrated that the age-standardized incidence rate of MALT-lymphoma increased gradually from the year 1999. In 2017, the age-standardized incidence rates of MALT-lymphoma among the general population, males, and females were 1.57, 1.53, and 1.61 per 100,000 individuals, respectively.
In the United States, 8,821 patients were diagnosed with MALT-lymphoma between 2001 and 2009, and the age-adjusted incidence rate of MALT-lymphoma was 12.3 per 100,000 individuals.8 Although the data on the age-standardized incidence rates of MALT-lymphoma in other countries were not available, the age-standardized incidence rates of marginal zone lymphoma were reported to be 0.5, 0.74, 1.53, and 0.79 in Japan (2008), Hong Kong (2000–2001), the United States (2001–2010), and Korea (1999–2012), respectively.2122232425 The approximate incidence of MALT-lymphoma can be estimated from these data.
Additionally, MALT-lymphoma is reported to be associated with good prognosis. In Korea, the 5-year RSR of patients with distant stage MALT-lymphoma was 91.3% between 2013 and 2017. MALT-lymphoma has varied clinical presentations as it is a heterogenous disease.91026 However, the natural course of MALT-lymphoma is indolent. Consistent with the results of the present study, a study reported that patients with MALT-lymphoma exhibit prolonged survival.27 At diagnosis, 62%–68% of patients exhibited localized MALT-lymphoma, and the site of MALT-lymphoma was bone marrow in approximately 17%–22% of patients.1028 In the present study, localized MALT-lymphoma was observed in 67%–72% of cases between 2008 and 2017; this may partially explain the high 5-year RSR among patients with MALT-lymphoma.
The overall incidence of MALT-lymphoma in female was higher than that in male. This may be because female aged 40–59 years exhibited a higher incidence of disease than male, especially in 2017. The results of the present study are consistent with those of previous studies, which reported high incidence of MALT-lymphoma among females (female:male ratio, 1.2).10293031 In contrast to the findings of our study, the results of a recent study in the United States revealed high incidence of MALT-lymphoma among males (male:female ratio, 1.01).8 This sex disparity in the incidence of MALT-lymphoma can be attributed to the affected anatomical sites. The predominant sites of MALT-lymphoma in males were the stomach, skin, kidney, and small intestine, whereas those in females were the salivary glands, thyroid, and soft tissue.832 These disparities may be explained by the differential prevalence of infection or autoimmune disorders between males and females. Further studies are needed to evaluate the correlation between age and MALT-lymphoma site.
MALT-lymphoma accounts for 16.7% of all non-Hodgkin lymphoma cases in Korea.33 The stomach is the most common site of MALT-lymphoma. The other sites of MALT-lymphoma include the lung (14%), head and neck (14%), skin (11%), thyroid gland (4%), salivary gland (6%), and eye (12%).2734 A single center study in Korea estimated that gastric MALT-lymphoma accounts for 50% of all MALT-lymphoma cases.35 The incidence of gastric MALT-lymphoma has been increasing in the last few decades and accounts for approximately 2%–8% of all gastric neoplasms.236 The results of the present study provide useful insights into the incidence and survival rates of gastric MALT-lymphoma. This study initially aimed to investigate the incidence and survival rates of MALT-lymphoma. However, data on the primary organs affected by MALT-lymphoma were not available in the KNCIDB. Thus, the incidence and survival rates of gastric MALT-lymphoma were inferred based on the data of MALT-lymphoma in the KNCIDB. The incidence of gastric MALT-lymphoma was assumed to be 30% of the incidence of MALT-lymphoma according to a population-based study in the United States, which reported that the stomach was the site of MALT-lymphoma in 2,702 (30.6%) patients out of 8,821 patients.8 Several studies in Korea demonstrated that the 5-year survival rates of patients with MALT-lymphoma were in the range of 87%–94%.3738 This study demonstrated that the 5-year RSRs of male and female patients with distant stage MALT-lymphoma were 92.6% and 89.6%, respectively. Thus, the 5-year survival rate was arbitrarily estimated to be approximately 90%. These findings indicate that patients with gastric MALT-lymphoma exhibit a good prognosis. However, these findings should not be universally extrapolated to the general population because some Korean studies were performed with a small number of patients: one study included only 185 patients (5-year survival rates for H. pylori infection-positive and H. pylori infection-negative patients were 90.2% and 87.0%, respectively).38
In clinical practice, patients with MALT-lymphoma are treated based on the etiology, risk factors, lymphoma site, lymphoma stage, clinical characteristics, and physician's experience and preference. Various therapeutic strategies, such as antibiotics, chemotherapy, radiotherapy, and surgery, are used to obtain good clinical outcomes.926 Nevertheless, there is no definite consensus on the optimal treatment strategy for MALT-lymphoma. The mechanisms underlying the pathogenesis and prognostic index are unknown. Therefore, there is a need to minimize these variations. Further studies are needed to investigate the etiologies, risk factors, pathogenesis, clinical characteristics, and prognostic factors of the different sites of MALT-lymphoma. One critical limitation of this study is that there were no data on the primary sites of MALT-lymphoma. In the KNCIDB, the code C88.4 does not have information on the primary sites. However, MALT-lymphoma was the most common disease among the C88 diseases in the nation-wide data, which represented the entire South Korean population.
In conclusion, although the incidence of MALT-lymphoma in Korea is low, it has been increasing in recent years. In Korea, the prognosis of MALT-lymphoma is good even at an advanced stage. These findings will provide invaluable insights on MALT-lymphoma to clinicians as well as useful information on survival rates to patients. In the KNCIDB, the code C88.4 does not provide data on the primary lymphoma site. Therefore, the KNCIDB should be modified to identify the primary sites of MALT-lymphoma (C88.4) in the future.
Go to :
 XML Download
XML Download