

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Saliva samples have merits compared with nasopharyngeal/oropharyngeal (NP/OP) swabs for developing a rapid self-diagnosis kit, and tests in resource-poor countries or overwhelming outbreak settings lacking well-trained healthcare workers (HCW). No HCW or personal protection equipment is needed to collect saliva, which can reduce the infection risk, time, cost and effort of HCW. Therefore, the US Food and Drug Administration (FDA) authorized a saliva test for emergency use for diagnosing severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in mid-April 2020 based on limited data.1
Regarding the diagnostic value of saliva samples for SARS-CoV-2 infection, few clinical data are available and the results are inconsistent2345678; moreover, the viral load and kinetics of SARS-CoV-2 in saliva are not clear, because recent comparative studies of the viral kinetics at multiple body sites did not include the oral cavity or saliva.910
This study was performed to evaluate the viral load in saliva and to compare the viral load and kinetics of SARS-CoV-2 in saliva with those in standard NP/OP swabs.
METHODS
Patients
Fifteen patients with SARS-CoV-2 infection who were admitted to Chonnam National University (CNU) Hospital (3 patients), CNU Hwasun Hospital (2 patients), CNU Bitgoeul Hospital (7 patients), and Keimyung University Dongsan Hospital (3 patients) from March 19 to April 10, 2020 in Korea were enrolled prospectively.
Sample collection and laboratory examination
Matched samples of NP/OP swab, saliva, sputum (if the patient had sputum) were collected at Day 1 of admission and every other day till consequently negative for two times. Saliva was collected by asking the patient to spit from the oral cavity in accordance with the recent study approved by FDA.1 Sputum was collected by asking the patient to cough from the throat. NP/OP swabs were collected in the same tube containing 2.5 mL of universal transport medium (Asan Pharmaceutical, Seoul, Korea). In patient's room, 1–2 mL of saliva or sputum was collected in sterile containers, and then diluted using same volume of sterile saline or universal transport medium in the Laboratory.
Real-time reverse transcription polymerase chain reaction (rRT-PCR) was performed at laboratory department of CNU hospital. First, 200 μL was taken from each sample and RNA was extracted using an automated nucleic acid extraction system (AdvanSure™ E3 System; LG Chem, Seoul, Korea). The extracted RNA was amplified using a commercial rRT-PCR kit (PowerChek™ 2019-nCoV Real-time PCR Kit; Kogenebiotech, Seoul, Korea) and detection system (CFX96™ Real-time PCR detection system; Bio-Rad, Hercules, CA, USA) to detect the envelope (E) and RNA-dependent RNA polymerase (RdRP) genes. Forty cycles of PCR were performed and cycle threshold (Ct) values were determined for each gene. A positive rRT-PCR result was defined when the Ct values of both the E and RdRP genes of SARS-CoV-2 were 35 or less. The Ct value of RdRP of each sample was used for further statistical analyses.
Statistical analyses
Continuous variables were expressed as means ± standard errors of the means or median and interquartile range (IQR). Mann–Whitney U test or Kruskal–Wallis test were used to compare statistical differences in continuous variables and χ2 test was used in categorical variables. All tests of significance were two-tailed, and P values ≤ 0.05 were deemed to indicate statistical significance. SPSS (version 26.0; IBM Corporation, Armonk, NY, USA) and GraphPad Prism (version 8.4.3; GraphPad software, San Diego, CA, USA) were used for statistical analyses.
Ethics statement
The study was approved by the Institutional Review Board (IRB) of CNU Hospital (IRB no. CNUH-2020-149) and Keimyung University Dongsan Hospital (IRB No. 2020-03-027). CNU Hwasun Hospital (2 patients) and CNU Bitgoeul Hospital (7 patients) belong to the same group as CNU Hospital. Informed consent was waived for observational study design. IRB approval for these two hospitals was jointly conducted by IRB of CNU Hospital. Informed consent was waived for the observational study design.
RESULTS
Median age of 15 patients was 59 (range, 17–91; IQR, 25–62) years and 5 (33%) were male. Two (11%) patients were asymptomatic, 8 (53%) patients had upper respiratory symptoms without pneumonia, and 7 (47%) patients had pneumonia. Three (20%) patients required oxygen therapy.
The overall sensitivity of rRT-PCR using saliva was 64% (34/53), which is lower than the 77% (41/53) using NP/OP swabs (Table 1). The sensitivities of rRT-PCR using NP/OP swabs, sputum, and saliva were 74% (23/31), 68% (21/23) and 71% (22/31) in patients with sputum. The sensitivity of rRT-PCR using saliva (8/15, 53%) was especially significantly lower than that using the NP/OP swab specimen (14/15, 93%) in early stage (1–5 days after symptom onset; P = 0.013) (Table 1). The sensitivity of rRT-PCR using saliva was especially lower in patients without sputum (12/22, 55%) (Table 1).
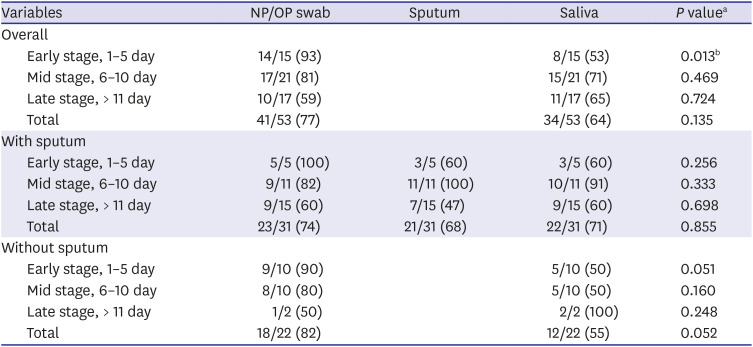
Table 1
Comparison of RdRP gene positive rate among NP/OP, sputum and saliva according to the time period after symptom onset and in patients with or without sputum
Data were expressed as number of positive samples/number of total samples (%).
NP/OP = nasopharyngeal/oropharyngeal.
aχ2 test was used to compare the positive rate; bP values ≤ 0.05.
![]()
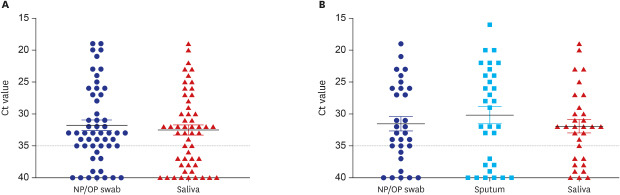
The Ct values of saliva (median, 32; IQR, 28–38) were comparable to those of NP/OP swabs (median, 33; IQR, 27–35) (P = 0.753) (Fig. 1A) in overall 53 samples from 15 patients. In 8 patients with sputum, the Ct values of saliva (32; IQR, 29–37) were also not different to those of NP/OP swabs (33; IQR, 26–36) and sputum (29; IQR, 24–38: P = 0.664) (Fig. 1B).
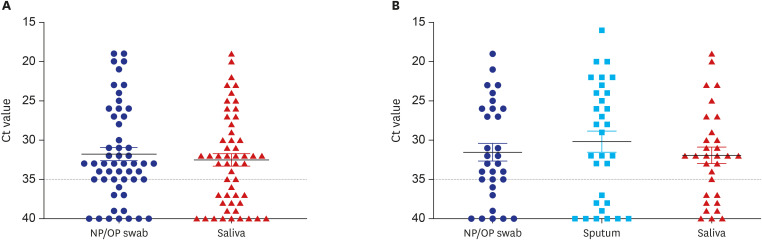
Fig. 1
The Ct values of the RdRP gene. (A) In saliva and NP/OP swabs in 53 pairs of samples from 15 patients, excluding negative samples (Ct value > 35 for both). P = 0.720 by Mann-Whitney U-test. (B) In saliva, NP/OP swabs, and sputum in 93 samples from eight patients who had sputum, excluding negative samples (Ct value > 35 for all three). P = 0.664 by Kruskal–Wallis test. Lines are the mean ± standard error of the mean.
Ct = cycle threshold, NP/OP = nasopharyngeal/oropharyngeal.
![]()
Fig. 2 shows the Ct values of saliva and NP/OP swabs according to the symptom onset. No statistically significant difference in Ct values was found in all stage between the saliva and NP/OP swab. However, although it was not statistically significant, the Ct values of saliva (33; IQR, 24–40) was higher in early stage compared to NP/OP swabs (32; IQR, 21–35, P = 0.267, Fig. 2A).
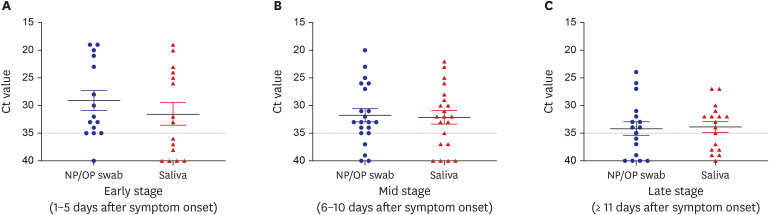
Fig. 2
The Ct values of the RdRP gene in saliva and NP/OP swabs in 53 pairs of samples from 15 patients according to the time periods from symptom onset. (A) Early stage (1–5 days after symptom onset). (B) Mid stage (6–10 days after symptom onset). (C) Late stage (≥ 11 days after symptom onset). Lines are the mean ± standard error of the mean. P = 0.267, 0.960 and 0.586 in each period respectively, by Mann-Whitney U test.
Ct = cycle threshold, NP/OP = nasopharyngeal/oropharyngeal.
![]()
The viral load kinetics of SARS-CoV-2 in each samples were shown in Fig. 3. Ct values of SARS-CoV-2 in saliva seemed to be higher in early phase compared to those in NP/OP swabs, however, the slope was not statistically significant between the two (Fig. 3A). Viral load kinetics are similar between saliva and NP/OP swabs in patients who had sputum (Fig. 2B); however, Ct values of SARS-CoV-2 in saliva seem higher in early phase and lower in late phase compared to those in NP/OP swabs in patients without sputum (Fig. 3, Supplementary Figs. 1 and 2).
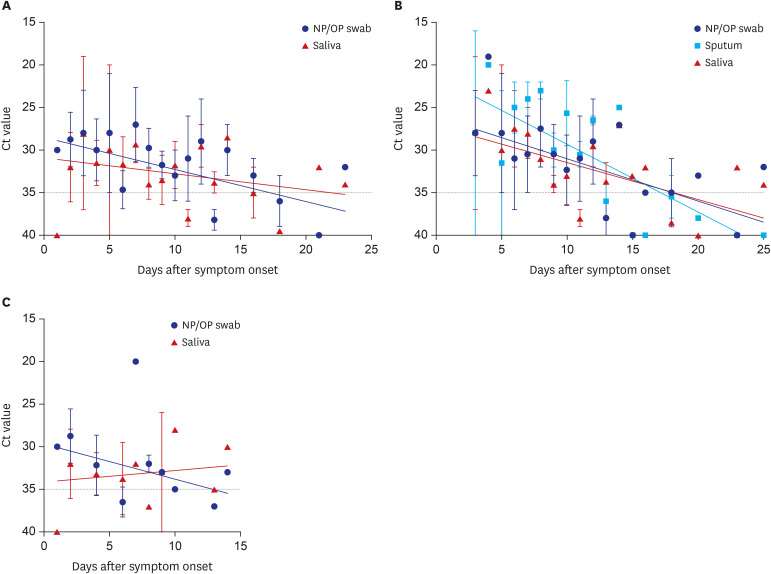
Fig. 3
Viral kinetics of each sample from (A) fifteen patients overall, (B) eight patients who had sputum, and (C) patients without sputum production. Expressed as the mean ± standard error of the mean. Slopes were calculated by simple linear regression. Slope were (A) −0.3754 (95% CI, −0.6924 to −0.0584) in NP/OP swabs, −0.1859 (95% CI, −0.5080 to 0.1362) in saliva; (B) −0.4330 (95% CI, −0.7922 to −0.0738) in saliva, −0.4958 (95% CI, −0.8746 to −0.1169) in NP/OP swabs, and −0.7950 (95% CI, −1.201 to −0.3894) in sputum (C) −0.4119 (95% CI, −1.157 to 0.3329) in NP/OP swabs, 0.1345 (95% CI, −0.6535 to 0.9225) in saliva.
Ct = cycle threshold, NP/OP = nasopharyngeal/oropharyngeal.
![]()
DISCUSSION
The detection rates of virus particle in saliva and in NP/OP swabs differ according to the respiratory virus species; influenza virus was better detected in NP/OP swabs, but adenovirus was better detected in saliva, compared to other respiratory viruses.11
Recent studies by one investigator group suggested that SARS-CoV-2 is detected consistently in samples of posterior oropharyngeal secretion coughed by patients.1213141516 However, the samples are similar to pharyngeal secretions or sputum rather than saliva considering the anatomical site and method of collection.
Several studies evaluated the diagnostic value of saliva samples for SARS-CoV-2 infection; however, the results are inconsistent. In SARS-CoV-2 assay by Rutgers Clinical Genomics Laboratory,1 there was 100% positive and negative agreement between the results obtained from testing of saliva and those obtained from NP/OP swabs, suggesting that saliva samples can completely replace NP/OP swabs. Additional studies showed that SARS-CoV-2 is also detected consistently in saliva samples, similar to the NP/OP samples in three peer-reviewed studies with limited sample sizes and two non-peer reviewed studies.23456 In contrast, lower sensitivity of rRT-PCR using saliva sample compared to NP/OP swabs were reported in other studies; one peer reviewed8 and one non-peer reviewed.6
A recent study suggested that the positive rate rRT-PCR using NP swab was 6% higher than that of using saliva in the first week from symptom onset and 20% higher in the second week.8 In contrast to the study, the sensitivity of rRT-PCR using saliva was significantly lower than that using NP/OP swabs in 1–5 days from symptom onset in this study. Several studies have shown that even in the case of saliva, a large amount of virus was detected in the early stages and gradually decreased over time. However, in these studies on SARS-CoV-2 kinetics of saliva, the posterior oropharyngeal saliva sample, which is easy to mix with sputum, was used to increase sensitivity. There is a study in Korea that reported SARS-CoV-2 kinetics of saliva in two cases, but the sample size are not enough to make a conclusion and they were patients who had sputum. The viral load kinetics of saliva in patients who had sputum was similar to NP/OP swabs in this study; however, the viral load kinetics of saliva in patients who did not have sputum was rather similar to viral kinetics of samples from gastrointestinal tract including stool17 than respiratory specimens in this study; Our data suggest that passive contamination of sputum affect the kinetics of saliva. Additional studies in patients who do not have productive sputum or pharyngeal secretion are needed to make a conclusion on the viral load kinetics of SARS-COV-2 in saliva.
The Ct value of the NP/OP and sputum in this study was lowest in the early stage of disease and it was reached around cut-off value within 2 weeks which was similar to previous Korean cases.1819 The positive rate of NP/OP swab was significantly higher than that of saliva in early stage of disease and the difference was disappeared in the mid and late stage of disease.
Our study suggests that saliva samples can be used for a rapid screening test or a complementary test to NP/OP swabs. However, it has been shown in this study that saliva samples cannot replace NP/OP swabs collected by HCW especially in early stage and in patients without sputum.
Our study have several limitations. First, saliva was not collected under direct observation, although it was collected from every admitted patient after education to minimize contamination of sputum. Second, in this study, no mechanism studies have been conducted on how viruses are detected in saliva. Additional study is needed to evaluate whether SARS-CoV-2 is secreted from oral mucosa or salivary glands or passively contaminated by pharyngeal secretion.20
In conclusion, saliva sample itself is not appropriate for initial diagnosis of COVID-19 to replace NP/OP swabs, especially for the person who does not produce sputum. COVID-19 cannot be excluded when the test using saliva is negative, and it is necessary to retest using NP/OP swabs.
 XML Download
XML Download