

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Rifampin-resistant (RR) and multidrug-resistant (MDR) tuberculosis (TB) are diseases that are difficult to treat, with high case fatality rates. Early diagnosis and prompt treatment initiation can increase the chances of cure, reduce mortality, and prevent transmission and acquisition of additional resistance.12 The phenotypic drug susceptibility testing (pDST) was the only diagnostic test available for drug-resistant TB (DR-TB) for a long time. However, pDST took months to confirm MDR-TB, inevitably leading to delayed treatment and thus poor outcomes.3 Rapid molecular drug susceptibility testing (mDST) such as the Xpert MTB/RIF (Xpert)4 and MTBDRplus line probe assay (LPA)5 were endorsed by the World Health Organization in 2008 and 2011, respectively. Numerous studies have shown that mDST could shorten the time to diagnose MDR-TB, thereby reducing the time to MDR-TB treatment initiation and improving the outcomes of MDR-TB patients.678910111213141516
As new diagnostics and new drugs become available, the paradigm of MDR-TB treatment is changing from a hierarchical drug combination based on pDST to the immediate initiation of a new regimen based on mDST.17 mDST has become a critical element of MDR-TB management, and its coverage is one of the indicators used to evaluate the National TB Control Program.18
In Korea, LPA and Xpert were introduced in 2007 and 2012, respectively, and have been integrated into routine clinical practice. The 2017 Korean TB guidelines recommended mDST only for patients at risk of drug resistance,19 but the 2020 guidelines have recently been revised to recommend mDST for all suspected TB patients.20 However, there has been little nationwide data on mDST coverage and the impact of these tests on the time to MDR-TB treatment initiation. The purpose of this study was to evaluate the current status and trends in mDST coverage and the impact of mDST on the time to MDR-TB treatment initiation in Korea.
METHODS
Study subjects and design
The Korea Centers for Disease Control and Prevention (KCDC) implemented a National TB Expert Review Committee (NTBERC) to approve the use of bedaquiline and delamanid in MDR-TB patients, following the official notification in September 2016. If physicians want to prescribe bedaquiline and delamanid for their patients, they should mandatorily submit a written application form and documents consists of medical history, imaging, and microbiological test results, rationales of new drug use, and tentative treatment regimen. If new drug use is approved, regular reports on treatment progress should be submitted to the NTBERC.
We included patients who submitted application forms for novel drug use to the NTBERC from September 1, 2016 to November 30, 2019. We retrospectively reviewed their medical records. As the main purpose of this study was to evaluate the impact of mDST on MDR-TB treatment initiation, patients who were previously diagnosed with DR-TB or started MDR-TB treatment prior to reporting DST results were excluded.
Data collection
Patient data were retrospectively collected from the submitted application forms and documents, which were anonymized and then provided to the researchers by the KCDC. For cases without sufficient data, the KCDC contacted individual physicians to obtain additional information. The following data were collected: demographic data, TB history, type of healthcare facility, microbiological results, DST results, and radiological data. If mDST was performed after reporting the pDST result, it was excluded from the analysis.
Definition
We analyzed the treatment episode at the time when the application form was submitted to the NTBERC. The day of initial treatment was defined as the day when the anti-TB drug was first administered. Baseline data were defined as the data collected at the time of initial treatment initiation. The day of MDR-TB diagnosis was defined as the day of issue of the DST report. The day of MDR-TB treatment initiation was defined as the day when the treatment started with at least two second-line anti-TB drugs.
Three periods were defined as indicators to assess the impact of mDST. Time to MDR-TB treatment initiation was defined as the period from the day of initial treatment to the day of MDR-TB treatment. Time to MDR-TB diagnosis was defined as the period from the day of initial treatment to the day of MDR-TB diagnosis. Treatment delay was defined as the period from the day of MDR-TB diagnosis to the day of MDR-TB treatment.
Statistical analysis
Categorical variables are presented as frequencies and percentages and continuous variables are presented as medians with interquartile range (IQR). Pearson's χ2 test or Fisher's exact test were used to compare categorical variables. Pearson's χ2 test for trend was used to assess annual trends in the coverage of mDST. Given the non-normal distribution of the data, Kruskal-Wallis test was used to assess intergroup differences in continuous variables and Jonckheere-Terpstra test was used to assess annual trends in the time to MDR-TB treatment initiation. A Cox proportional hazards model was used to determine the predictors of shorter time to MDR-TB treatment initiation. A P value < 0.05 was considered significant. Statistical analyses were performed using SPSS Statistics, version 22.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
During the study period, 813 patients from 85 hospitals submitted application forms to the NTBERC. During data collection and verification, 192 (23.6%) patients were excluded for the following reasons: 151 were previously diagnosed with MDR/RR-TB, 11 were previously diagnosed with DR-TB other than MDR/RR-TB, 3 started MDR-TB treatment prior to reporting DST results, and 27 had insufficient medical records.
A total of 621 patients were finally included. All of them were patients with laboratory-confirmed pulmonary MDR/RR-TB. Their baseline characteristics are shown in Table 1. Their median age was 53 years, 418 (67.3%) patients were male, 370 (59.6%) were new cases, and 277 (44.6%) had smear-positive sputum at baseline.
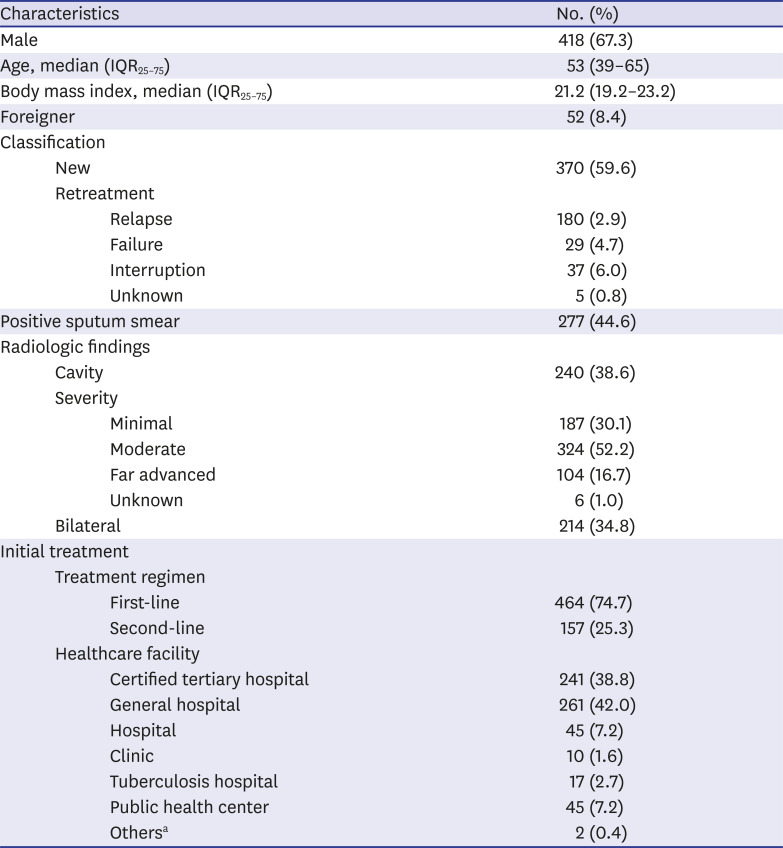
Table 1
Baseline characteristics of the 621 patients with multidrug/rifampin-resistant tuberculosis
![]()
Initial treatment was started with first-line regimens in 464 (74.7%) and second-line regimens in 157 (25.3%) patients. Initial treatment was started most commonly in a general hospital (42.0%), followed by certified tertiary hospitals (38.8%), hospitals (7.2%), public health centers (7.2%), TB hospitals (2.7%), and private clinics (1.6%). For MDR-TB treatment, 303 patients (48.8%) were transferred to other healthcare facilities. MDR-TB treatment was started most commonly in a certified tertiary hospital (56.2%), followed by general hospitals (23.2%), TB hospitals (20.0%), and hospitals (0.6%).
Coverage of mDST
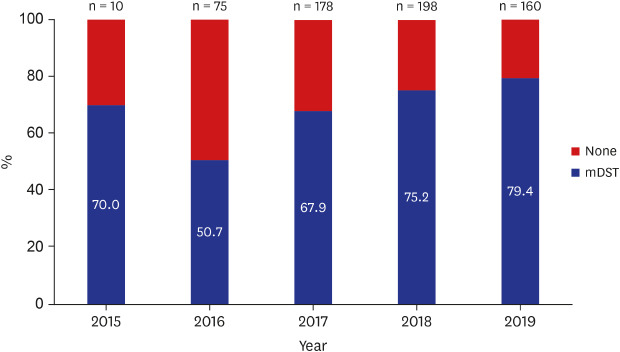
Of the 621 patients, mDST was performed in 442 (71.2%) patients; X-pert alone in 109 (17.6%), LPA alone in 199 (32.0%), and both Xpert and LPA in 134 (21.6%) patients (Table 2). The coverage of mDST has gradually increased to 70% in 2015, 50.7% in 2016, 67.9% in 2017, 75.2% in 2018, and 79.4% in 2019 (P for trend = 0.001) (Fig. 1). Additional mDST to detect fluoroquinolone resistance were performed in 13 patients; MTBDRsl (Hain Lifescience, Nehren, Germany) in 9 patients and target sequencing in 4 patients.
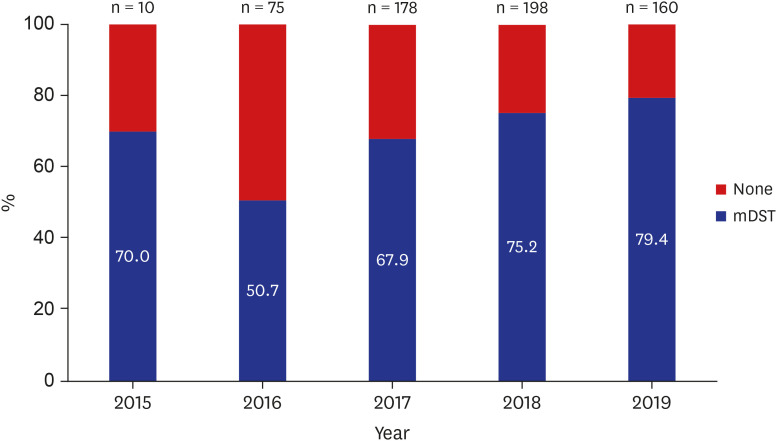

Fig. 1
Annual trends in coverage of mDST (P < 0.001, P for trend < 0.001).
mDST = molecular drug susceptibility testing.
![]()
Table 2
Coverage rate of mDST among patients with multidrug/rifampin-resistant tuberculosis
Data are presented as number (%).
mDST = molecular drug susceptibility testing, LPA = line probe assay.
*P for trend < 0.001.
![]()
mDST was performed more commonly in retreatment case (74.9%, 188/251) than in new case (68.6%, 254/370), but it was not statistically significant (P = 0.107). The coverage rate of mDST was the highest in TB hospitals (82.4%), followed by certified tertiary hospitals (81.3%), public health centers (77.8%), general hospitals (69.0%), hospitals (33.3%), and clinics (10.0%) (Supplementary Table 1).
Decision test for MDR-TB treatment
MDR-TB treatment was decided upon by the result of Xpert in 156 (25.1%), LPA in 202 (32.5%), and pDST in 263 (42.4%) patients (Table 3). The proportion of mDST as a decision test for MDR-TB treatment has gradually increased to 70% in 2015, 40% in 2016, 51.7% in 2017, 62.1% in 2018, and 66.2% in 2019 (P for trend < 0.001).

Table 3
Decision test for multidrug-resistant tuberculosis treatment
Data are presented as number (%).
mDST = molecular drug susceptibility testing, LPA = line probe assay, pDST = phenotypic drug susceptibility testing.
*P for trend < 0.001.
![]()
There was a gap between performing mDST and deciding treatment based on its result. Of the 442 patients who underwent mDST, 84 (19.0%) did not decided MDR-TB treatment based on the results of mDST; 22 (5.0%) had invalid mDST results (n = 16: indeterminate result, n = 6: susceptible to rifampin) and 62 (14.0%) had valid results but did not adhere to them.
Time to MDR-TB treatment initiation
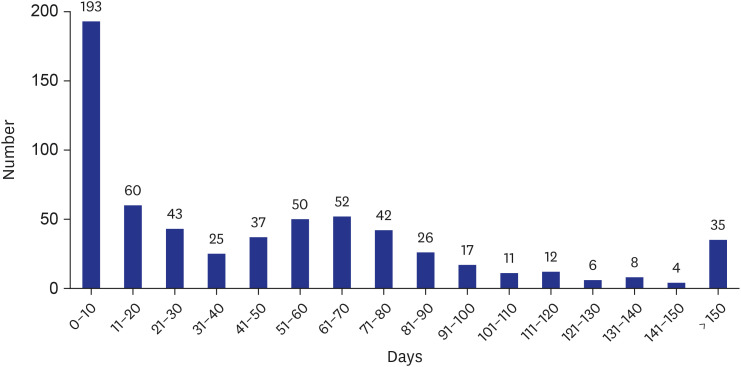
Median time to MDR-TB treatment initiation was 35 days (IQR25–75 0–72), median time to MDR-TB diagnosis was 26 days (IQR25–75 0–58), and median treatment delay was 6 days (IQR25–75 2 –14) (Table 4). Time to MDR-TB treatment has gradually decreased during the study period, mainly due to the reduction in time to MDR-TB diagnosis (P = 0.003) rather than the reduction in treatment delay (P = 0.124).

Table 4
Annual trends in time to MDR-TB treatment initiation
Data are presented as median (interquartile range25–75).
MDR-TB = multidrug-resistant tuberculosis.
aJonckheere-Terpstra test.
![]()
The distribution of time to MDR-TB treatment initiation is shown in Fig. 2. Of the 621 patients, 296 (47.7%) started MDR-TB treatment within 30 days of initial treatment initiation.
Time to MDR-TB treatment initiation was significantly different among diagnostic methods. When MDR-TB treatment was decided by the Xpert test, median time to MDR-TB treatment initiation was 0 days, which was significantly shorter than the 22 days for LPA and the 72 days for pDST (P < 0.001) (Table 5). Median treatment delay was 2 days for Xpert, which was also significantly shorter than the 5 days for LPA and the 13 days for pDST (P < 0.001), respectively.

Table 5
Time to MDR-TB treatment initiation by diagnostic method
Data are presented as median (interquartile range25–75).
MDR-TB = multidrug-resistant tuberculosis, LPA = line probe assay, pDST = phenotypic drug susceptibility testing.
aKruskal-Wallis test.
![]()
In multivariate analysis, the independent predictors of shorter time to MDR-TB treatment initiation were retreatment case (adjusted hazard ratio [aHR], 1.30; 95% confidence interval [CI], 1.10–1.54), Xpert testing (aHR, 2.42; 95% CI, 2.03–2.88), and LPA testing (aHR, 1.83; 95% CI, 1.55–2.16) (Table 6). Transfer-out to other healthcare facilities was negatively associated with a shorter time to MDR-TB treatment initiation (aHR, 0.74; 95% CI, 0.63–0.88).
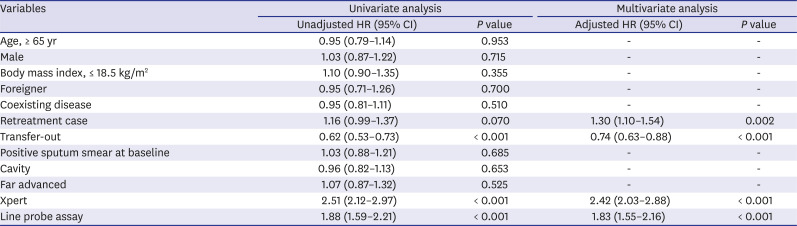
Table 6
Predictors of shorter time to multidrug-resistant tuberculosis treatment initiation
![]()
DISCUSSION
This study showed that mDST coverage is gradually increasing in Korea. mDST contributes to reducing the time to MDR-TB diagnosis and thus the time to MDR-TB treatment initiation. The time to MDR-TB treatment initiation was reduced to a median of 35 days, compared to about 3 months in a previous study using pDST.21 Our results could provide a snapshot of current status of mDST use and impact of mDST on initiation of MDR-TB treatment in Korea. In this study, 71.2% of MDR-TB patients underwent mDST and 47.7% started MDR-TB treatment within 30 days of initial treatment. Second-line regimen was started as initial treatment in 25.3% of patients, most of them were detected by Xpert assay.
We included 621 patients with MDR/RR-TB over 3 years. This number of patients is estimated to be approximately one-third of the MDR-TB patients who are notified annually in Korea.22 Therefore, our results possibly represent the current nationwide status of mDST coverage among MDR-TB patients.
We identified some challenges related to the use of mDST in Korea. First, mDST coverage varied by healthcare facility. It was higher in TB hospitals, public health centers, and tertiary certified hospitals, but lower in clinics and hospitals. This finding suggests that access to mDST is limited, particularly in primary and secondary healthcare facilities in the private sector.
Second, there were some cases of noncompliance with the TB guidelines. The 2017 Korean TB guidelines,19 which was effective during the study period, recommended mDST should be performed in patients at risk of DR-TB including retreatment case. However, 25% (188/251) of retreatment case did not perform mDST. In addition, 14% (62/442) of patients with valid results did not adhere to mDST results, which cause a delay in MDR-TB treatment initiation. There may be several reasons why the attending physician did not switch to a second-line drug regimen even though they recognized rifampin-resistance detected by mDST: favorable treatment response to the first-line drugs, failure to recognize mDST result by mistake, or the possibility of false positive mDST results. For some MDR-TB patients, the therapeutic response to the first-line drug may be favorable, but generally the final treatment outcome is poor, so the therapy should be switched to the second-line drugs, and if a patient had a low-risk of drug resistance, the same DST or other form of mDST should be repeated again. New TB guidelines recommend performing mDST as an initial test to all TB patients and, if rifampin resistance is confirmed, further confirming at least resistance to fluoroquinolones using mDST.1720 While the rapid DST of fluoroquinolone has yet to be licensed in Korea, this year the Korean CDC will install the mDST of fluoroquinolone for free.
Third, treatment delay from diagnosis to treatment initiation is still lengthy and was not significantly reduced during the study period. Median treatment delay from MDR-TB diagnosis to MDR-TB treatment initiation was 6 days, which accounts 17% of the total time to MDR-TB treatment initiation. Complex operational and health system factors are involved in this treatment delay. One of these may be the lack of a system that immediately reports DST results to physicians in each hospital. Transfer-out to other hospitals can also cause treatment delays. In the present study, transfer-out to other hospitals for MDR-TB treatment occurred in 48.8% of patients and was revealed as an independent predictor for treatment delay. A thorough reporting system and efficiently organized transfer system for MDR-TB patients might contribute to further shortening the time to MDR-TB treatment initiation.
Fourth, the coverage rate of LPA was 53.6%, which was higher than the 39.1% for Xpert. This is probably because LPA was introduced earlier, and thus the LPA-based algorithm was already implemented in each hospital. In addition, LPA can be used more widely because it can be performed using culture isolates in smear negative cases. The superiority of diagnostic accuracy between these two tests is unclear. However, in terms of shortening the time to MDR-TB treatment initiation, the Xpert-based algorithm is much better than the LPA-based algorithm. Compared to LPA, Xpert has reduced treatment delays as well as time to MDR-TB diagnosis. The reduction in treatment delay is probably due to the rapid and predicted turnaround time of Xpert, which could ensure that subsequent MDR-TB treatment starts earlier. In addition, Xpert is more sensitive in detecting resistance-conferring mutations in smear-negative sputum.23 Considering that more than 50% of patients were smear negative at baseline in our study, the Xpert test is more appropriate, as an initial test, than LPA.
There is a growing awareness that mDST should not be implemented alone, but should be part of a comprehensive algorithm along with other diagnostic methods.24 In some countries, such as South Africa1112 and Myanmar,14 the culture-based pDST was replaced by the Xpert-based algorithm. In a study conducted in Taiwan,25 the use of Xpert as an initial test, followed by two LPAs (MTBDRplus and MTBDRsl) simultaneously, was more effective than phenotypic culture-based DST. Further research is needed regarding how to integrate mDST in diagnostic algorithms for TB in Korea.
Our study has some limitations. We could not evaluate the impact of mDST on clinical outcomes such as treatment outcomes and mortality. Second, selection bias may have influenced our results. Our patients were MDR/RR-TB patients who had difficulty in constructing an effective regimen with existing anti-TB drugs. In addition, 23.6% of patients were excluded mainly because they were previously diagnosed with DR-TB. Therefore, our results may not reflect the overall situation of TB or MDR-TB patients in Korea.
As the use of mDST is expanding, the time to MDR-TB treatment initiation is gradually shortening in Korea. To further shorten the time to MDR-TB treatment initiation, additional efforts are needed to improve the entire process of MDR-TB treatment, which include universal access to mDST, the DST reporting system, the patient transfer system, adherence to mDST results, and optimal integration of mDST into the diagnostic algorithm.
 XML Download
XML Download