

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Suicide attempt (SA) and non-suicidal self-injury (NSSI) in youths are major mental health problems and are steadily increasing.12 Suicide is the leading cause of death among youths.34 Korea is among the OECD countries with high teen suicide rates, even when several countries with the highest teen suicide rates including New Zealand or Iceland were excluded.5 NSSI is defined as a deliberate destruction of one's own body without suicidal intent, using methods that are not socially sanctioned. This concept was proposed in section of 3 of the Diagnostic and Statistical Manual of Mental Disorders-fifth edition (DSM-5) as a “condition for further study.”6 NSSI is more commonly observed among youths and young adults with an approximate life time prevalence of 18%–24%.2789 Although little research on the prevalence of NSSI in the Korean population is present, NSSI is commonly observed among Korean adolescents with a prevalence of at least 8.8% to 9.2%.101112 SA and NSSI have a profound impact on families and communities and incur massive societal costs.1314 Hence, considerable clinical attention is warranted to develop preventive strategies.
NSSI and suicidality are common reasons for emergency presentations in child and adolescent psychiatry. In Spain, among 328 mental health emergencies in a pediatric emergency department (PED), self-harm behavior, irrespective of degree of suicidal intent, was the second most common reason for presentation in females (29%).15 In a Canadian study, NSSI within the previous 24 hours was recorded in 45% of the 468 cases of youths who presented with mental health emergencies.16 Recently, a significant increase in the number of emergency department visits for self-inflicted injury among adolescents has been observed worldwide,17 which is the most important reason for the increase in overall visits.18 Therefore, suicide and NSSI are major emergency psychiatric problems in youths and the PED plays an important role as a gateway to psychiatric management through coordinating transfers or referrals to child and adolescent psychiatry units.19 It is crucial that children and adolescents with SA and/or NSSI be assessed and managed properly.
However, to the best of our knowledge, most preceding studies concerning PED utilization or emergency psychiatric visits of children and adolescents were performed in Western countries, and there is a paucity of literature on the PED utilization for psychiatric problems in Korea. From 2016 to 2018, 2,842 children and adolescents visited the PED for psychiatric problems,20 but their reasons for visiting the PED, their psychiatric diagnosis, and method of management have not been studied. Therefore, this study aimed to investigate the incidence of PED admission due to psychiatric problems in children and adolescents and to identify demographic and clinical characteristics of youths who visited the PED for SA and/or NSSI in the past 59 months at a tertiary hospital.
Go to : 
METHODS
Patient population
We conducted this retrospective chart review of the children and adolescents who presented to the PED at Asan Medical Center for psychiatric problems between January 2015 and November 2019. Youths who were 18 years of age or younger and who visited the PED for any psychiatric problem were included in the study. If any individual visited on more than one occasion during this period, the clinical data for each visit were collected. Cases were not included in this study if there was an absence of appropriate psychiatric evaluation by a psychiatrist (e.g., medical treatment was done only by pediatricians, youths and his or her guardians refused to contact a psychiatrist, and the purpose of PED visit was a non-medical reason such as administrative affair).
Data collection
Demographic variables at the time of visit including age, sex, school year, special education, parental marital status, living status, and accompanying guardian at the PED were collected. Other clinical data including the date of visit, psychiatric diagnosis according to DSM-5, comorbid pediatric diagnosis, presence of SA or NSSI, presence of violence, abuse, bullying, length of stay in the PED, use of psychotropic medication and disposition after psychiatric intervention (e.g., follow-up loss, outpatient referral, admission to psychiatric ward, transfer to another hospital for admission to a psychiatric ward, and admission to pediatric ward) were thoroughly reviewed based on medical records. Psychiatric diagnosis was made by a psychiatry resident in the PED and further confirmed by the board-certified child and adolescent psychiatrists. The lifetime diagnosis of a psychiatric disorder and lifetime history of abuse or bullying, SA, and NSSI prior to the PED visit were also reviewed.
Statistical analysis
We counted a number of visits on a monthly basis during the observation period. The cases of SA or NSSI at the time of visit were counted separately. We compared demographic factors and clinical characteristics of children and adolescents who visited the PED for SA and/or NSSI and those without both SA and NSSI. A student's t-test was used to analyze continuous variables such as age, school years, and length of stay in the PED. A chi-square test or Fisher's exact test was used for categorical variables to compare between-group differences. Multivariate logistic regression analysis was performed to identify independent predictive factors of SA and/or NSSI. All statistical analyses were performed using SPSS (ver. 24; IBM SPSS Statistics, IBM Corporation, Armonk, NY, USA). A two-tailed P < 0.05 was considered significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Asan Medical Center (IRB No. 2019-1597). As this study was conducted retrospectively, the requirement for informed consent was waived.
Go to :
RESULTS
During the 59-month observation period, a total of 194 youths visited the PED for psychiatric problems and 46 youths (23.7%) visited the PED for SA and/or NSSI at least once. A total number of 336 visits were made by 194 youths, while the number of visits for SA and/or NSSI was 91 (27.1% of PED visits). Among 91 visits related to SA and/or NSSI, 41 visits (n = 36) were due to SA only, 44 visits (n = 31) were due to NSSI only, and 6 visits (n = 6) for co-occurring SA and NSSI.
Among the 47 visits due to SA, drug intoxication (n = 38) was the most common, followed by hanging (n = 5) and falling (n = 4). A total number of 30 youths (15.5%) had a lifetime history of SA. In total, 16 youths had attempted suicide 1 time, 5 had attempted 2 times, 3 had attempted 3 times, 2 had attempted 4 times, and 4 had attempted 5 times or more. Of the 30 youths with a lifetime history of SA, 26 also had a history of NSSI in the past.
Of the 50 visits due to NSSI, cutting (n = 46) was the most frequent, followed by hitting or banging (n = 4). Among the 73 youths (37.6%) who had a lifetime history of NSSI, it was found that 11 youths had injured themselves 1 time, 3 had injured 2 times, 1 youth had injured 4 times, and 1 youth had injured 6 times, while 57 youths had 6 or more incidences of NSSI. It was found that 26 of the 73 youths who had a lifetime history of NSSI also had attempted suicide.
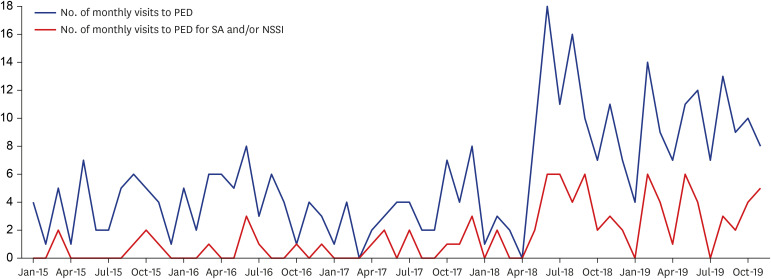
Fig. 1 shows that the number of total visits began to show an increase in May 2018 and the peak was observed in June 2018 with 18 visits occurring this month. The mean monthly visit number was 3.6 in year of 2015, while the number was 7.9 in 2018. Interestingly, a similar pattern was observed in the number of visits for SA and/or NSSI, suggesting that the increase in PED visits was related to an increase in SA and/or NSSI. There were 6 visits for SA and/or NSSI out of 43 PED visits (14.0%) in the year of 2015 while the rate was 13.2% in 2016, followed by 23.3% in 2017 and 34.7% in 2018.
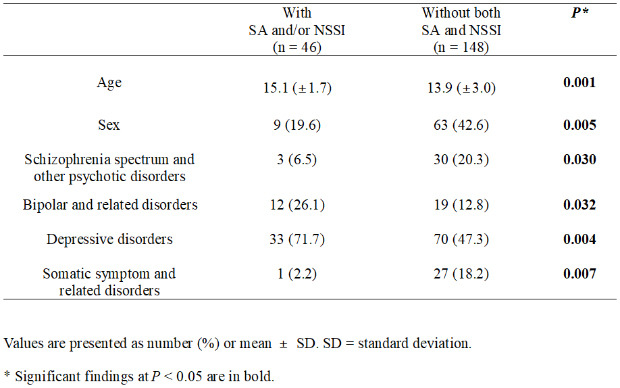
The demographic characteristics of the children and adolescents with SA and/or NSSI and those without both SA and NSSI are presented in Table 1. Mean age and school year were higher in youths with SA and/or NSSI (P = 0.001, P = 0.001, respectively). There was a higher proportion of girls among children and adolescents who visited the PED due to SA and/or NSSI than among those without SA and/or NSSI (P = 0.005) and they were more likely to report parental absence (P = 0.023). There was no statistically significant difference for special education, living status, and accompanying guardian at the PED between the two groups. Youths with SA and/or NSSI were more likely to have multiple PED visits (visit range 2–9) than those without both SA and NSSI (P = 0.068).
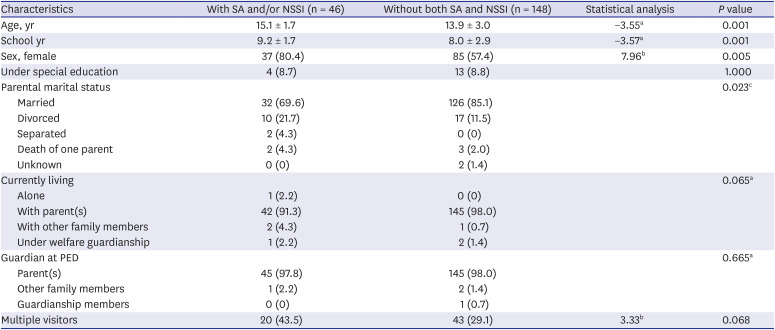
Table 1
Demographic characteristics of youths with a history of SA or NSSI and those without
Data are presented as mean ± standard deviation or number (%).
SA = suicide attempt, NSSI = non-suicidal self-injury, PED = pediatric emergency department.
at-test; bχ2 test; cP was calculated by a Fisher's exact test.
![]()
Table 2 shows the comparison of psychiatric diagnosis according to DSM-5 category at the time of PED visit. Youths with SA and/or NSSI were at a greater risk of bipolar and related disorders (P = 0.032) and depressive disorders (P = 0.004), while youths without both SA and NSSI had higher chance of schizophrenia spectrum and other psychotic disorders (P = 0.030), as well as somatic symptom and related disorders (P = 0.007). There were 14 youths (7.2%) who had experienced abuse (5 individuals with physical abuse, 3 with sexual abuse, 2 with neglect, 1 with emotional abuse, and 3 with more than 2 types of abuse) and 53 youths (27.3%) with a history of bullying; however, no significant difference was observed when we compared the prevalence rate of abuse and bullying between youths with SA and/or NSSI and those without both SA and NSSI.
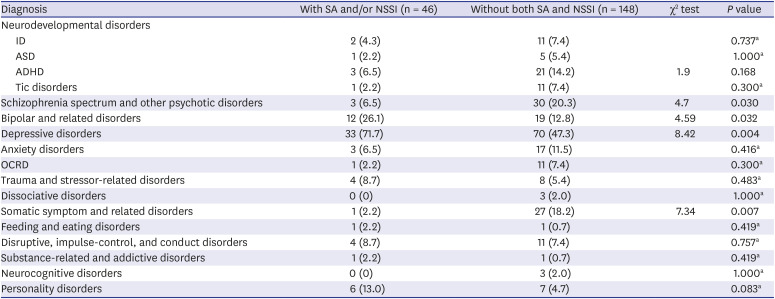
Table 2
Comparisons of psychiatric diagnosis between youths with suicide attempt or NSSI and those without
SA = suicide attempt, NSSI = non-suicidal self-injury, ID = intellectual disability, ASD = autism spectrum disorder, ADHD = attention-deficit hyperactivity disorder, OCRD = obsessive-compulsive and related disorder.
aP was calculated by a Fisher's exact test.
![]()
Demographic factors and psychiatric diagnosis which were significantly different between two group differences were entered into multivariate logistic regression analysis (Table 3). After adjusting for all other variables, bipolar and related disorders (odds ratio [OR], 6.72; 95% confidence interval [CI], 1.21–37.48), depressive disorders (OR, 9.59; 95% CI, 2.09–43.96), and somatic symptom and related disorders (OR, 0.12; 95% CI, 0.01–0.94) were independent predictors of youths' SA and/or NSSI.

Table 3
Predictive factors for suicide attempt or non-suicidal self-injury of youths
![]()
We also analyzed the acute psychiatric management of each PED visit (Table 4). Children and adolescents with SA and/or NSSI stayed significantly longer in the PED (P = 0.007). They were more likely to be prescribed psychotropic medications (P = 0.003), but there was no difference in disposition of the PED visitors after psychiatric intervention.

Table 4
Acute management in the pediatric emergency department of youths presenting with suicide attempt or non-suicidal self-injury and those without
Data are presented as number (%) or mean ± standard deviation.
SA = suicide attempt.
aχ2 test; bP was calculated by a Fisher's exact test; ct-test.
![]()
Go to :
DISCUSSION
We conducted a retrospective chart review of children and adolescents who presented to an emergency service. Our results show that NSSI and suicidality are one of the main reasons for child and adolescent psychiatric presentation at the PED and account for 27% of the PED visits for psychiatric problems. This is in line with previous studies on emergency mental health care151621 which reported that NSSI and suicidality accounted for 29%–45% of the PED visits for psychiatric problems. Our results suggest the importance of proper evaluation and management of SA and/or NSSI in emergency child and adolescent psychiatry.
Our results show that there was an increase in PED visits by children and adolescents in one general hospital over the past 5 years. Moreover, this tendency was related to the increased number of visits for reasons related to SA and/or NSSI. This finding is consistent with previous research, which indicate that PED visitation in youths was increasing and the largest increase was found in adolescents due SA or self-inflicted injury.182223 SA and NSSI have been reported to be prevalent in Korean children and adolescents,1011122425 and our study showed that more Korean youths are presenting to the PED for psychiatric problems, especially those relating to suicidality and NSSI. Considering these results together, the PED has a significant role in the acute management of high-risk psychiatric children and adolescents. In other words, the ED offers an important treatment setting as a frontline contact for those with suicidality or NSSI and moreover, it is relatively easily accessible.2627
A steep increase in the number of PED visits was observed during May 2018. One possible explanation for this could be the copycat effect. In High School Rapper 2, which was a popular survival hip-hop show broadcasted from February 2018 to April 2018, self-harm was mentioned in the lyrics of the rap and wounds of self-injury were exposed several times during the show. Several studies have previously shown a rapid and sustained increase in suicide following a celebrity's completed suicide in Korea.2829 The strong effect of the media has been suggested as a reason for copycat suicides, and new media including Instagram are particularly important as potential risk factors for NSSI.303132 Although we could not delineate a causal relationship between increased SA or NSSI and social phenomenon or media in this study, improvement in media reporting and the implementation of preventive strategies for high-risk populations might be important in reducing harmful behaviors among adolescents.3334
In our study, youths with SA and/or NSSI were older and more likely to be girls, to have parents who were not married, and to have a diagnosis of bipolar or depressive disorders. These findings are in agreement with previous research about risk factors for suicidality or NSSI. Female sex,353637 having one or more psychiatric disorders,3638 and having mood disorders such as major depressive disorder and bipolar disorder were reported to be associated with SA among adolescents.39404142 Parental divorce or absence4344 as well as a negative relationship or impaired communication with an individual's parents was also found to be a risk factor for suicide.454647 Depressive disorder was the strongest predictor of future SA.484950 For NSSI, female sex and being of middle or high school age had an increased risk of engaging in NSSI.515253 The risk for NSSI was higher among individuals who had mood disorders,54 where both depressive disorder and bipolar disorder were associated with increased risk for NSSI.5556 Parental divorce also had an impact on self-harm.4457 Previous research showed that SA and NSSI share several common risk factors5859 Moreover, as we found in this study, SA and NSSI frequently co-occur,16 and SA and NSSI are risk factors for each other5859 Future studies are needed to investigate shared and specific risk factors.
Considering that NSSI and suicidality were found to be the main reasons for presenting to a child and adolescent emergency psychiatric service, it seems crucial for physicians at PEDs to provide proper crisis intervention and referral to mental health services when appropriate.60 Our results indicate that youths with SA and/or NSSI tended to have multiple visits, stayed longer at the PED, and had prescribed more psychotropic medication. This is in accordance with previous studies, which have shown psychiatric problems are associated with a longer PED stay than non-psychiatric problems.616263 Furthermore, the rate of antidepressant prescription or medication adjustment was up to 50% if the ED visits were associated with SA or NSSI.6465 As continuous mental health care can prevent future suicide,66 high-risk youths who present to the ED with SA and/or NSSI require more clinical attention. Hence, the PED is one of the most important departments in a general hospital for the provision of acute management in cases of SA and/or NSSI in children and adolescents, with an important role in referring those with high risk to the correct mental health services.276768697071
The findings of our study should be interpreted in the context of some limitations. First, because this study was conducted at one tertiary hospital, it does not represent the national population. Thus, a multicenter study or study using national public health data, such as National Health Insurance Service, is recommended. Second, we conducted a retrospective chart review and therefore the quality of the medical records could not be standardized as they were recorded by different psychiatrists. However, we did cross-check our cases and found moderate agreement. Third, the diagnoses of mood disorders and comorbid psychiatric disorders were not based on structured interviews. Fourth, data may be missing depending on the decision of the emergency physicians to refer the ED patients to psychiatrists, and cases were excluded when youths or their guardian refused to contact a psychiatrist, which could result in a selection bias.
Despite these caveats, our study is the first to evaluate presentation to the child and adolescent emergency psychiatry services in Korean children and adolescents and to show a high incidence and the clinical characteristics of youth with SA and/or NSSI in Korea. Our study suggests that the PED could play an important role in assessing high-risk youths and referring them to mental health services.
Go to :
 XML Download
XML Download