

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Korea has successfully controlled the coronavirus disease 2019 (COVID-19) epidemic with relatively few confirmed cases and deaths numbering 11,719 and 273, respectively, as of June 6, 2020.1 However, Daegu, the fourth-largest city in Korea with about 2.5 million population, experienced an explosive increase in the number of COVID-19 patients in late February.2 Approximately 60%–70% of confirmed cases and deaths in Korea were recorded in Daegu.1
During an epidemic of infectious diseases, seroprevalence studies are important in demonstrating the widespread and undiagnosed infection in the general population.3 Public policies against infectious diseases can vary depending on the results of seroprevalence studies.3 Seroprevalence studies reported to date from several countries have shown that the seroprevalence levels are highly variable by region and time.456789101112131415 However, a significant fraction of the population has developed antibodies against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), suggesting that the infection is much more pervasive than implied by the number of confirmed cases.
The Korean strategy against COVID-19 consisting of massive testing, contact tracing, and quarantine has gained the attention of many countries as a model to control the COVID-19 pandemic. In particular, the rapid and extensive testing for coronavirus is a key element. In this sense, it is plausible that the size of undiagnosed missing cases in Korea may be substantially smaller than that of other countries. Alternatively, it is possible that the number of undiagnosed missing cases is substantial in spite of the Korean strategy due to the high proportion of asymptomatic and mildly symptomatic patients and the high transmission rate of COVID-19.1617
Although the epidemic of COVID-19 in Korea started on January 20, 2020,1 no seroprevalence data are available yet. Seroprevalence data provide an opportunity to evaluate the effectiveness of strategy containing COVID-19 via massive testing, contact tracing, and quarantine. Therefore, this preliminary study was performed to estimate the seroprevalence among individuals without previous history of COVID-19 diagnosis, who visited outpatient clinics of one hospital in Daegu, the epicenter of COVID-19 epidemic in Korea.
Go to : 
METHODS
Study subjects
This study was performed at Daegu Catholic University Hospital, a tertiary care medical center in Daegu, Korea. The study involved 198 cases who were recruited from patients and their guardians visiting outpatient clinics from May 25 to June 5, 2020 using bulletin boards and banners in the hospital. Inclusion criteria were: 1) subjects who were never diagnosed with COVID-19, 2) subjects who do not currently have any COVID-19-related symptom such as fever or cough, and 3) subjects who live in Daegu.
Measurement
We collected 3 mL of blood via antecubital vein. After centrifugation, serum was preserved at −70°C and defrosted upon testing. DIAKEY COVID-19 immunoglobulin (Ig)M/IgG Rapid Test Kit was used to perform the solid immunochromatographic assay (Shin Jin Medics Inc., Goyang, Korea). This device is preembedded with recombined COVID-19 envelop antigens including nucleocapsid (N) protein and RBD domain of spike (S) protein expressed by Escherichia coli. The specificity and sensitivity of antibody testing, obtained from 60 polymerase chain reaction (PCR)-positive specimens and 30 PCR-negative specimens, were estimated as 92% and 100%, respectively. Serum (10 µL) was infused into the test kit, and the results were obtained 15 minutes after the addition of buffer. Two doctors independently interpreted results by visual inspection. When both diagnosed the kit as positive, it was confirmed as positive case.
A self-administered questionnaire was used to collect information on age, gender, body weight, height, smoking history, history of doctor-diagnosed diabetes or hypertension, reason of current hospital visits, history of COVID-19 PCR test, history of COVID-19 related symptoms during the previous 5 months, and presence of COVID-19 confirmed cases among family, friends, or coworkers.
Statistical analyses
First, the seroprevalence was determined among all subjects and the exact binomial 95% confidence interval (CI) was calculated from the test for one proportion using z-statistics. Next, we compared seroprevalence among subgroups stratified by characteristics of study subjects, including age (< 40, 40–59, ≥ 60 years), gender, body mass index (BMI) (< 25, ≥ 25 kg/m2), smoking history (current, previous, never), history of doctor-diagnosed diabetes or hypertension (yes, no), reason for the current hospital visit (patient, guardian), and the presence of COVID-19 confirmed cases among close contacts (yes, no). Associations between seroprevalence and characteristics of study subjects were evaluated using χ2 tests or Fisher's exact tests. All statistical analyses were performed using SPSS 25 (IBM Corp., Armonk, NY, USA) and P < 0.05 was considered as statistically significant.
Finally, we roughly estimated the number of undiagnosed missing cases in Daegu. Instead of considering age and gender-specific seroprevalence due to the limitation of study sample, we used the seroprevalence among all subjects based on the total population size of Daegu, which was estimated at 2,438,031 according to 2019 statistics of resident registration. Although a total of 6,886 cases were confirmed by PCR as of June 6, 2020, the number of undiagnosed missing cases was similar whether or not the number of confirmed cases was considered.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Daegu Catholic University Hospital (approval No. CR-20-103) and written informed consent was obtained from all study participants.
Go to :
RESULTS
Table 1 lists the general characteristics of study subjects. The number of patients was 103 while that of guardians was 95. Only 3.5% of study subjects reported the presence of confirmed COVID-19 cases among close contacts such as family, friends, or coworkers. Subjects with a history of PCR testing or COVID-19-related symptoms during the previous 5 months were 7.1% and 9.1%, respectively. The age range was from 18 to 82 years and the mean age was 51.7 years. Half of the study subjects included men; 70.7% had a BMI < 25kg/m2, and 23.2% comprised current smokers. Subjects with a history of diabetes or hypertension constituted 9.6% and 18.7%, respectively.
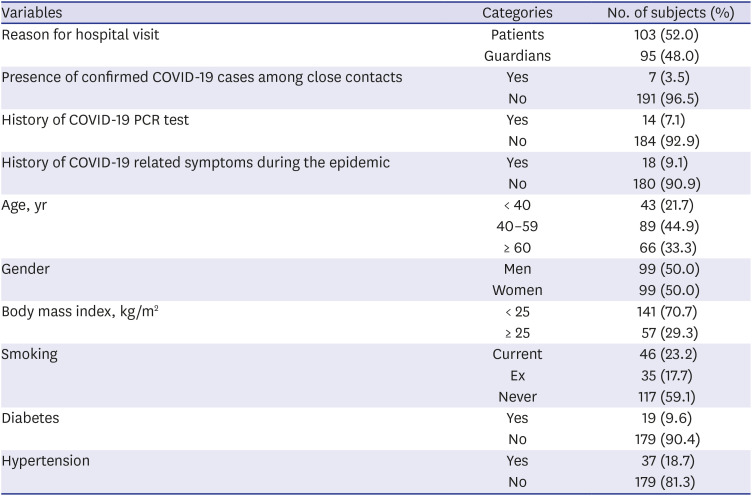
Table 1
General characteristics of study subjects
![]()
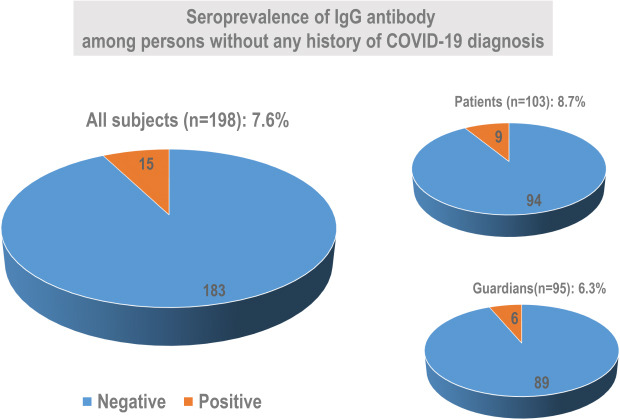
There were 15 positive IgG cases among 198 subjects who were never diagnosed with COVID-19 (Table 2). Seroprevalence was estimated at 7.6% (exact binomial 95% CI, 4.3%–12.2%). Among 15 positive cases, only one case had a PCR-confirmed case among their close contacts. Also, only 2 cases reported that they had experienced COVID-19-related symptoms. Seroprevalence was similar between patients and guardians. All positive cases were from different households.
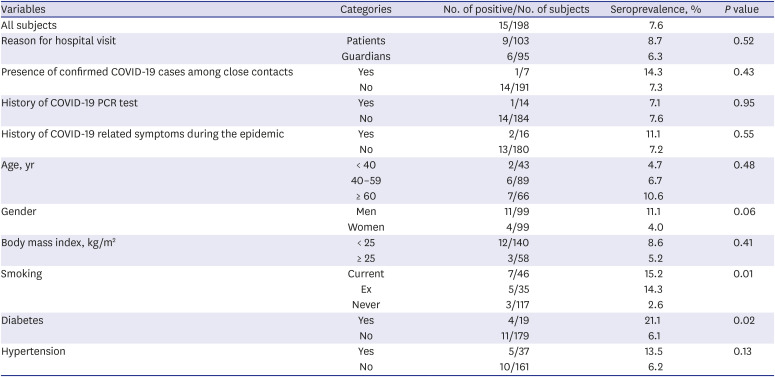
Table 2
Seroprevalence according to characteristics of study subjects
![]()
Table 2 presents seroprevalence according to the characteristics of study subjects. Seroprevalence varied significantly depending on cigarette smoking history or the status of diabetes. Seroprevalence of never smokers (2.6%) was significantly lower than that of current smokers (15.2%) or ex-smokers (14.3%) (P = 0.01). Diabetic patients (21.1%) also had a higher seroprevalence than those with non-diabetes (6.1%) (P = 0.02). Neither obesity nor hypertension status was related to seroprevalence.
Based on the seroprevalence in all subjects, the number of people with positive IgG in Daegu was estimated to be roughly 185,290 (95% CI, 104,835–297,439). As the total number of confirmed cases reported at Daegu as of June 6 were only 6,886, it was estimated that the number of undiagnosed missing cases may be 27-fold higher than the number of confirmed cases based on PCR testing in Daegu.
Go to :
DISCUSSION
Among subjects who were never diagnosed with COVID-19 in Daegu where demonstrated the epidemic peak in late February, the seroprevalence was 7.6%. Most of the IgG positive cases were asymptomatic during the epidemic. Also, only one case had a PCR-confirmed case among their close contacts. Although this study was conducted with a small size and unrepresentative sample, our finding suggests that the number of undiagnosed missing cases may be at least ten-fold higher than the total number of confirmed cases based on PCR testing.
Since the onset of the pandemic, Korea adopted a test-track-trace approach utilizing large-scale PCR tests and expansive tracing technology. In this scenario, a general belief is that there may be few undiagnosed missing cases. However, even under this stringent strategy of detecting all positive cases regardless of symptoms, a large number of missing undiagnosed cases was apparent. The missed undiagnosed cases may be related to the characteristics of SARS-CoV-2, especially the high proportion of infected patients who are asymptomatic or have only mild symptoms and the high transmission rate.1617 Our study suggests that any containment strategy may have a limited value with SARS-CoV-2 even though it is effective in flattening the epidemic curve.18
The accuracy and reliability of antibody tests for SARS-CoV-2 have been disputed.1920 The use of serological testing at the individual level such as immune passport, selecting vaccination target, and collecting therapeutic plasma is risky due to false-positive and false-negative cases.1920 However, different from the applications at the individual level, it is important to note that the estimated average seroprevalence at the population level is acceptable even with moderate sensitivity and sepcificity.3 Among many available serological methods, immunochromatographic assays are reported to show relatively lower sensitivity compared to other tests such as enzyme-linked immunosorbent assay (ELISA) or chemiluminescence immunoassay (CLIA).21 In fact, seroprevalence data are important to understand the scale and spread of the pandemic and predict the probability and timing of future waves of recrudescence.3 Also, it can address public health questions, such as the safety of relaxing stay-at-home orders or school closures and evaluations of alternative interventions.3
Often, seroprevalence data are linked to the concept of herd immunity, the minimum level of population immunity required to halt the spread of infection in the community.22 Assuming a basic reproduction number (R0) of 3 for SARS-CoV-2, the herd immunity threshold is estimated to be approximately 60%–70%.23 Judging from this threshold of herd immunity, the seroprevalence data worldwide including ours is far from the threshold of herd immunity. However, the most widely cited threshold of herd immunity was calculated based on unrealistic and simple assumption of homogeneous population susceptibility.24 When individual variation in susceptibility or exposure to SARS-CoV-2 was factored in a model, the threshold of herd immunity is much lower, closer to 10%–20%.24
One of the most important factors contributing to the heterogeneity of susceptibility of a population may involve exposure to other coronaviruses such as common cold, which is known as cross-immunity.25 A recent study clearly demonstrated that about half of blood samples collected before COVID-19 epidemic had T cell-mediated immunity against SARS-CoV-2.26 Cross-immunity may be one reason underlying the low mortality of COVID-19 in many Asian countries, where most coronavirus-related epidemics such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) originated.
This study has several limitations. First, the study subjects were recruited from outpatients and their guardians at a single hospital, limiting the generalizability of the current finding to Daegu. Also, the sample size was small. Second, the accuracy and reliability of serology assay are disputed due to the possibility of false-positive cases because of cross-reaction with another coronavirus such as common cold. Conversely, there can be false-negative cases as well. In a recent meta-analysis comparing several serological methods,21 the sensitivity of immunochromatographic assays was lower than that of ELISA or CLIA, but all methods yielded high specificity closer to 99%. Third, the situation in Daegu may differ from that of other places in Korea due to the outbreak during a short period. Although a large number of symptomatic and asymptomatic cases were detected in Daegu through massive PCR testing, contact tracing of confirmed cases was not performed as meticulously as at other places. Therefore, the current results may not be generalized to Korea.
In conclusion, this study suggests that the actual number of individuals infected with SARS-CoV-2 in Daegu, Korea greatly exceeds that of the PCR-confirmed number of cases. Although a large study based on a representative sample is required to confirm the current findings, even the stringent strategy of Korea designed to detect and quarantine all positive cases regardless of symptoms may not be successful in containing the COVID-19 pandemic.
Go to :
 XML Download
XML Download